


Abstract
Background: Since 2016, abortion care has undergone several important changes, particularly related to the provision of medical abortion using mifepristone. We aimed to document characteristics of the abortion care workforce in Canada after the update of clinical practice guidelines of mifepristone use for medical abortion.
Methods: We conducted a national, web-based, anonymized, bilingual (English/French) survey. We collected demographics and clinical care characteristics of physicians and nurse practitioners who provided abortion care in 2019. Between July and December 2020, we distributed the survey through professional organizations, including The College of Family Physicians of Canada and The Society of Obstetricians and Gynaecologists of Canada. We present descriptive statistics.
Results: Overall, 465 respondents representing all 10 provinces and 3 territories in Canada completed the survey. Of these, 388 (83.4%), including 30 nurse practitioners, provided first-trimester medical abortion, of which 350 (99.4%) used mifepristone. Two hundred and nineteen (47.1%) respondents provided first-trimester surgical abortion, 109 (23.4%) provided second-trimester surgical abortion and 115 (24.7%) provided second- or third-trimester medical abortion. Half of respondents reported fewer than 5 years of experience with any abortion care. Respondents reported providing a total of 48 509 abortions in 2019, including 32 345 (66.7%) first-trimester surgical abortions and 13 429 (27.7%) first-trimester medical abortions. In Quebec, only 1918 (12.5%) of reported abortions were first-trimester medical abortions. Primary care providers provided 34 540 (71.2%) of the total abortions. First-trimester medical abortions represented 44.4% (n = 2334) of all abortions in rural areas, as opposed to 25.6% (n = 11 067) in urban areas.
Interpretation: The increased availability of medical abortion facilitates abortion access, especially in primary care and rural settings, and where surgical abortion is not available. Rejuvenation of the workforce is a critical contributor to equitable access to abortion services.
In 2019, about 84 000 medical and surgical abortions were reported to the Canadian Institute of Health Information.1 One-third of women in Canada will have an abortion in their lifetime.2 According to our first Canadian Abortion Provider Survey (CAPS) in 2012, abortion care was provided by fewer than 300 physicians, many of whom focused their practice on abortion care.3 In contrast with rates greater than 80% in many European countries,4–8 fewer than 4% of abortions were medical.9 Procedures were provided by high-volume providers in specialized health care clinics, with limited access in rural areas.3,10,11 In 2016, the United Nations Human Rights Commissioner expressed concern over inequitable access to abortion services in Canada, and called on the Canadian government to improve equitable access.12
Several important health system and service changes have occurred since then. In 2017, mifepristone, the gold-standard medical abortion drug,13 became available in Canada.14–16 Restrictive regulations around prescribing and dispensing mifepristone were removed later that year.17 Evidence supporting the effective and safe provision of medical abortion using mifepristone by a range of primary health care professionals18,19 led to Health Canada’s approval of provision of medical abortion by nurse practitioners.20 The Society of Obstetricians and Gynaecologists of Canada issued evidence-based clinical practice guidelines on medical abortion in 201613 and on surgical abortion in 2018.21
We hypothesize that these changes have the potential to facilitate provision of abortion care, especially office- and primary care–based medical abortion, and rural abortion care. Documentation of the Canadian abortion workforce after these changes and the knowledge translation of these changes into practice is limited.22–24 We conducted a national survey of abortion providers in Canada, aiming to explore the characteristics and distribution of the workforce and the services they provide.
Methods
Study design and settings
From July to December 2020, we conducted a national survey of health care professionals who provided abortion services in 2019 in Canada (Appendix 1, available at www.cmajopen.ca/content/10/3/E856/suppl/DC1). Physicians and nurse practitioners who either performed surgical abortions or prescribed the medication for medical abortions were eligible to participate. We followed the Checklist for Reporting Results of Internet E-Surveys.25
Survey instrument
The 2019 CAPS was developed by members of the Contraception and Abortion Research Team — Groupe de recherche sur l’avortement et la contraception.26 To address our study aims, we adapted our 2012 survey instrument3,9,27 and incorporated latest evidence and expert opinions using a modified Delphi method, followed by piloting.28–31 We describe the development of our survey instrument in detail elsewhere.28
This web-based, anonymized survey was cross-sectional, national, self-administered and available in both English and French. The French version of the survey was professionally translated and reviewed by French-speaking abortion experts. The CAPS included a consent statement, and sections on demographics, clinical characteristics of abortion provision, administrator- or facility-level data, care of diverse populations and provider experience with stigma and harassment (Appendix 2, available at www.cmajopen.ca/content/10/3/E856/suppl/DC1).
The survey used a complex skip-pattern logic so that respondents only saw relevant questions. Questions critical for skip-pattern logic and data analysis were mandatory. Respondents could change answers on their current screen, but could not go back to previous screens. To increase survey completion rate, respondents could progress through the survey without answering the remaining nonmandatory questions. They could request remuneration (gift certificate of $50). We collected data through the secure server of the British Columbia Children’s Hospital Research Institute Research Electronic Data Capture platform.32
Recruitment
To reach potential participants, we distributed bilingual, generic survey links through multiple collaborating health care professional organizations, including The College of Family Physicians of Canada and The Society of Obstetricians and Gynaecologists of Canada. In addition, we recruited via publicly available sources in Canada, such as abortion clinics and hospital departments of obstetrics and gynecology, and of family medicine; we also recruited from our web-based community of abortion practice (www.caps-cpca.ubc.ca). We employed a modified Dillman technique to maximize the response rate, which included recruitment partners emailing survey reminders 1, 2 and 4–6 weeks after the initial invitation was distributed.33
Statistical analysis
As this was a web-based, anonymized survey with recruitment via distribution of a generic survey link that offered financial incentive, we screened all incoming responses for fraud using nonsensical answer combinations in the demographics. After we detected potential fraud, we adapted and combined multiple validated fraud detection components into a complex algorithm, details described elsewhere.34 Data cleaning included removing respondents who did not complete our eligibility confirming questions or who appeared to be duplicate entries.34
We conducted descriptive analyses to describe the workforce demographics and the type of abortion care provided by respondents. We included questions that were not answered by all respondents in the analysis. The denominator for each reported percentage consists of the number of respondents who answered that question. We used R Statistical Software to generate descriptive analyses using proportions and medians with interquartile ranges (IQRs), as appropriate.
Ethics approval
This study was approved by the University of British Columbia Children’s and Women’s Research Ethics Board (H18-03313).
Results
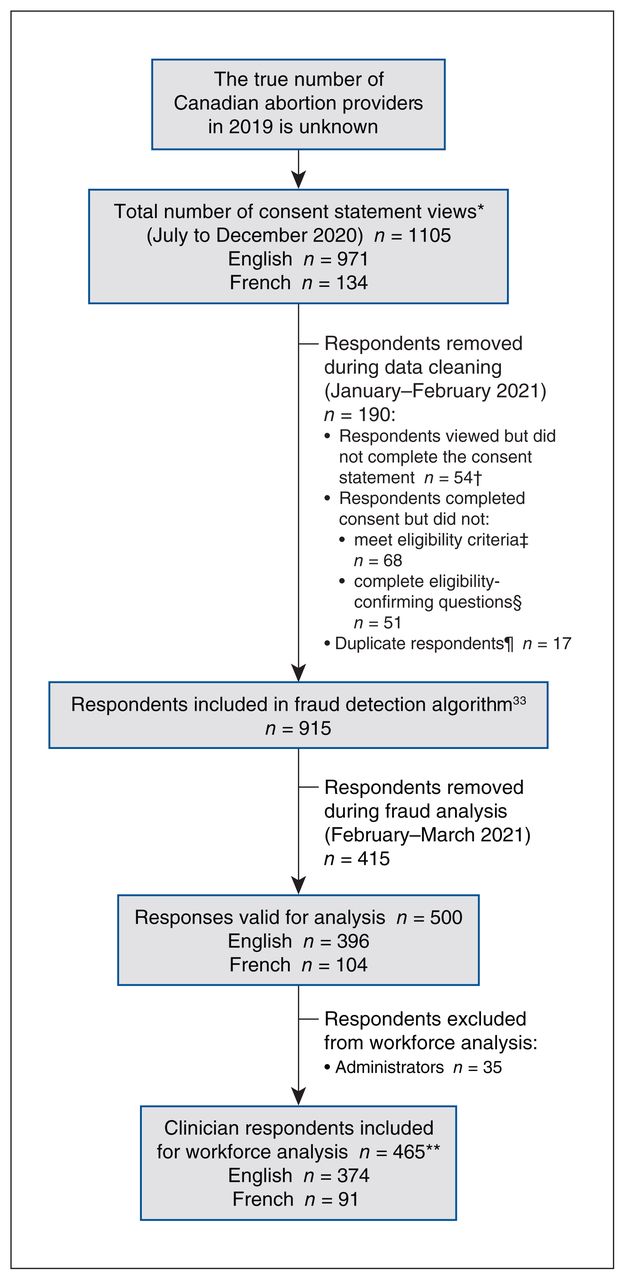
The flow of respondents from recruitment to data analysis is depicted in Figure 1. We included 465 clinician respondents for analysis. The completion rate was 69.5%. The response rate for each question was greater than 60%. It took respondents 30–80 minutes to complete the survey. The 435 physicians and 30 nurse practitioners reported providing 48 509 abortions in 2019 (Table 1), which represents over half of the total number of abortions reported in Canada in 2019.1 By specialty, 280 primary care providers, 145 general obstetrician–gynecologists and 40 specialists in maternal–fetal medicine responded. Most respondents in all specialties were women (n = 395, 84.9%). The median age was 42 (IQR 36–50) years, and respondents younger than 40 years formed the largest age group among primary care physicians (n = 123, 46.2%) and obstetrician–gynecologists (n = 60, 43.5%).

Respondent flow chart, informed by the Checklist for Reporting Results of Internet E-Surveys (CHERRIES).25 *Consent statement views recorded on Research Electronic Data Capture (REDCap) platform.32 †The participation rate was 95.1%. ‡Per programming in REDCap, respondents who did not answer mandatory inclusion criteria questions correctly were automatically exited from the survey. This included a question confirming that they had not taken the survey before. §Manual removal of respondents who exited the survey before completing mandatory eligibility questions. ¶Duplicate analysis was conducted using R Statistical software, flagging matching demographics, followed by manual review of all flagged respondents. We did not collect Internet Protocol addresses or use cookies, as per our research ethics board request, to maintain respondent anonymity. **Of 465 respondents, 323 (69.5%) completed the survey, defined as completing the last survey section.
Characteristics of abortion provider respondents by specialty
Characteristics of provider practice
Among respondents, 388 (83.4%) provided first-trimester medical abortions, 219 (47.1%) provided first-trimester surgical abortions, 109 (23.4%) provided second-trimester surgical abortions and 115 (24.7%) provided second- or third-trimester medical abortions (Table 1). Of respondents who provided first-trimester medical abortions, 350 (99.4%) used mifepristone; few reported using methotrexate–misoprostol or misoprostol alone. Most primary care providers offered first-trimester medical abortion (n = 275, 98.2%), 70.0% (n = 196) exclusively. Most (n = 24, 60.0%) specialists in maternal–fetal medicine provided second- or third-trimester medical abortions exclusively, and obstetrician–gynecologists offered the full range of abortion services, with most (n = 88, 60.7%) offering first-trimester medical and surgical abortions and 62 (42.8%) offering both first- and second-trimester surgical abortions (Table 1).
Of 48 509 reported abortions, 13 429 (27.7%) were first-trimester medical abortions, 32 345 (66.7%) were first-trimester surgical abortions and fewer than 5% were secondor third-trimester services. Primary care providers reported providing most (n = 34 540, 71.2%) of the total abortions, including most first-trimester medical abortions (71.4%), most first-trimester surgical abortions (73.9%) and half of the second-trimester surgical abortions (48.6%). Nurse practitioners reported providing 327 (2.4%) first-trimester medical abortions. Obstetrician–gynecologists and maternal–fetal medicine subspecialists provided most of the second- or third-trimester medical abortions (99.3%). Most respondents reported fewer than 5 years of experience with first-trimester medical abortion ((n = 223, 61.3%) and half of respondents (n = 209, 47.7%) had fewer than 5 years of experience with any abortion care. Among subspecialists in maternal–fetal medicine, a median of 5% (IQR 5%–10%) of their practice focused on abortion and contraception care; this proportion was a median of 15% (IQR 5%–30%) among primary care providers. Less experience providing first-trimester medical abortions was associated with a lower median focus of practice on abortion and contraception care (10% for those with < 5 yr experience v. 20% for those with > 20 yr experience).
Abortion providers and procedures by region
Most respondents were from Ontario (n = 153, 32.9%), Quebec (n = 107, 23.0%) and BC (n = 91, 19.6%) (Table 1). Providers of first-trimester medical abortions made up the largest proportion of respondents in every region, except in Quebec, where those who provided first-trimester surgical abortions made up a higher proportion (n = 84, 78.5%) (Table 2). Exclusive first-trimester medical abortion provision was reported by 44.5% (n = 207) of all respondents, but only by 10.3% (n = 11) of respondents in Quebec, as they mostly reported offering both first-trimester medical abortion and first-trimester surgical abortion (n = 57, 53.3%). The largest number of abortions reported in every region were first-trimester surgical abortions. Quebec had the lowest proportion of abortions that were first-trimester medical abortions (n = 1918, 12.5%).
Characteristics of abortion providers by region
Location of abortion provider practice
Figure 2 depicts respondents’ abortion clinical practice location and range of health care services provided at that location by type of abortion service. Most respondents reported providing first-trimester medical abortions outside of a hospital (n = 228, 66.5%), often in locations that provided other reproductive or general health care (n = 222, 97.4%). First-trimester surgical abortions were distributed between community hospitals (n = 77, 47.2%), academic hospitals (n = 49, 30.1%) and clinics outside of hospitals (n = 37, 22.7%); second-trimester surgical abortion services were less frequently provided outside of the hospital (n = 13, 20.6%) and shifted slightly toward the academic hospitals (n = 27, 41.5%). Second- and third-trimester medical abortions were exclusively reported in the hospital, particularly academic hospitals (n = 44, 64.7%). Providers’ practice location (hospital or outside of hospital) varied depending on type of abortion provided (Figure 2). Seventy-four respondents provided care at a second location within their primary province. A few respondents (n = 18, 3.9%) travelled to a second province to provide care, including 7 (38.9%) who travelled to the territories.

Respondents’ abortion clinical practice location and range of health care services provided at that location by type of abortion service. Note: Respondents indicated location and other types of care for each abortion service they provided.
Rural versus urban providers
Canada-wide, almost 4 in 10 respondents (38.9%) were classified as rural (Table 3). Broken down by specialty, 128 (46.2%) primary care providers, 50 (35.2%) obstetrician–gynecologists and none of the subspecialists in maternal–fetal medicine practised in a rural area. Almost all (n = 165, 92.7%) rural respondents provided first-trimester medical abortions, compared with 78.1% (n = 218) of urban respondents; exclusive first-trimester medical abortion provision was reported in 56.2% (n = 100) and 38.0% (n = 106) of rural and urban providers, respectively. Fewer abortions, and fewer of each individual type of abortion, were reported by providers in rural areas (n = 5259, 10.9%). First-trimester medical abortions represented 44.4% (n = 2334) of all abortions in rural areas, as opposed to 25.6% (n = 11 067) in urban areas.
Characteristics of abortion providers by rural or urban practice location
Guidelines
Respondents were asked to specify which guidelines they follow to provide abortion care; 434 responded to this question. More than 90% of respondents across all specialties (Table 1) and in most regions (Table 2) reported following the clinical practice guidelines of The Society of Obstetricians and Gynaecologists of Canada. Fewer than 3% reported in a free-text response that they followed guidelines from organizations other than of the National Abortion Federation or The Society of Obstetricians and Gynaecologists of Canada, most commonly the Collège des médecins du Québec.
Interpretation
We conducted a national survey on the abortion workforce and their services in 2019 and had respondents from all provinces and territories in Canada. Among respondents, most provided first-trimester medical abortions, which contributed to a quarter of all reported abortions. Although half of the respondents provided first-trimester surgical abortions, this contributed to two-thirds of all abortions. A quarter of respondents provided second-trimester surgical and secondor third-trimester medical abortions. Most respondents were primary care providers, and they provided two-thirds of all abortions. As gestational age increased, there was a shift toward obstetrician–gynecologists and specialists in maternal–fetal medicine delivering hospital-based abortions.
As in our 2012 survey, most respondents were from the most populous provinces (BC, Ontario and Quebec), roughly in proportion to the provincial populations.3 Most respondents were women, consistent with general analyses of the primary care workforce and our 2012 survey.3,36,37 We noted substantial rejuvenation among the abortion provider workforce; almost half of respondents were younger than 40 years, and half of primary care providers and a third of obstetrician–gynecologists indicated fewer than 5 years of abortion experience. Other evidence describing growth in the abortion workforce is emerging;22,24,38–42 this growth appears to be associated with the 2017 introduction of mifepristone in Canada and the subsequent removal of restrictive regulations. Our data indicate that nurse practitioners contribute to provision of first-trimester medical abortions.
Almost all of the respondents who provided first-trimester medical abortions reported use of a mifepristone regimen. The increase in the proportion of reported first-trimester medical abortions, from 3.8% in our 2012 survey9 to 27.7%, aligns with Canadian health administrative data.42 Reassuringly, almost all participants reported following The Society of Obstetricians and Gynaecologists of Canada guideline for abortion care.13 Regulations from the Collège des médecins du Québec initially required a potential provider of first-trimester medical abortions to learn to provide surgical services and still requires specific clinical training for physicians. Unsurprisingly, contrary to other provinces, very few respondents in Quebec provided first-trimester medical abortions exclusively.
As in our 2012 survey,3,9,27 most respondents were primary care providers. However, in 2019, the total number of abortions was distributed between a higher number of respondents (n = 465 v. 178) who, in general, reported a lower proportion of their overall practice was focused on abortion care. Most first-trimester medical abortions were provided outside hospitals by physicians delivering other reproductive or general health care services. The arrival of mifepristone for first-trimester medical abortions and removal of restrictive regulations likely facilitated the move of abortion care into office-based, primary, comprehensive reproductive and general health care settings. This is consistent with a qualitative, national study of abortion-providing and nonproviding physicians and health system stakeholders, which found that removal of restrictive regulations on mifepristone medical abortion facilitated implementation of abortion care in the primary care setting.22
Rural respondents reported a tenth of the overall procedures; 23.7% of reproductive age females (15–44 yr) in Canada lived rurally in 2019.43 However, almost half of these abortions were first-trimester medical abortions, in contrast with a quarter in urban areas. In addition, almost half of the providers of first-trimester medical abortions were located in rural areas. These findings highlight the important contribution of mifepristone to abortion care in rural areas and the related potential to decrease urban–rural access disparities. 22,44 Surgical abortion and second- or third-trimester services, provided by trained clinicians able to manage more complex patients, require surgical facilities or hospital-based settings, and are critical to provide the full range of abortion care. Quebec was the region with the fewest first-trimester medical abortions; this low percentage is corroborated by statistics from this province that show the proportion of first-trimester medical abortions as 3.6%, 7.9% and 11.9% for 2018, 2019 and 2020, respectively.45 Mixed methods research that included interviews with physicians and stakeholders in Quebec identified multiple barriers to implementation of mifepristone, including ongoing restrictive provincial medical policies, lack of human resources and infrastructure.22,46–48
This research informs knowledge translation activities that have the potential to facilitate education and abortion care provision, as well as consideration for similar removal of restrictive regulations in Quebec and international settings. Future qualitative research with providers, health system managers and patients will be needed to better understand service gaps, facilitators and barriers, and details on the patient journey through abortion care. Research leveraging complete data on the number of abortion providers and distribution of health services may be possible through the use of health administrative data.
Limitations
The main limitation of our study is the limited ability to determine the representativeness of our sample. The true number of abortion providers in Canada is unknown, partly owing to the sensitive nature of this work, and partly as it is not recorded systematically. Therefore, we do not know the denominator of eligible respondents from which to calculate a response rate. We mitigated this issue with our broad recruitment strategy, and by analyzing and interpreting our data with a focus on the internal consistency of the responses, comparing results with those from our 2012 sample. Our extensive recruitment strategy engaged the key professional organizations of physicians and nurse practitioners in Canada, many of which collaborated on our study. Despite the unanticipated impact of COVID-19, we recruited a larger number of providers than in our 2012 survey, most of whom indicated having less than 5 years’ abortion experience, which we believe is consistent with our hypothesized increase in the workforce.44,48,49 We detected fraudulent respondents in our survey and applied a rigorous fraud detection algorithm.34 We are confident that our final sample includes valid respondents.
Conclusion
The increased availability of medical abortion, as reported by our survey respondents, facilitates abortion access, especially in primary care and rural settings, and where surgical abortion is not available. Rejuvenation of the workforce is a critical contributor to equitable access to abortion services.
Acknowledgements
The authors thank the Women’s Health Research Institute of the British Columbia Women’s Hospital, the BC Women’s Hospital, The Society of Obstetricians and Gynaecologists of Canada and the Canadian Nurses Association for their in-kind support. In addition, they thank the survey respondents for their meaningful contribution to our research.
Footnotes
Competing interests: Regina Renner reports speaker fees from Merck. Sheila Dunn reports research grants from the Canadian Institutes of Health Research (CIHR) and the Ontario Ministry of Health and Long-term Care for other research related to abortion. She is co-lead of the abortion working group with The Society of Obstetricians and Gynaecologists of Canada. Wendy Norman reports grants from CIHR for other research related to family planning; payment for expert testimony from the Ontario Ministry of the Attorney General; and support for travel from CIHR, the Public Health Agency of Canada and the University of British Columbia and Monash University. No other competing interests were declared.
This article has been peer reviewed.
Contributors: All of the authors contributed to the conception and design of the work. Regina Renner, Madeleine Ennis and Arianne Albert acquired, analyzed and interpreted the data. Regina Renner and Madeleine Ennis drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This work was supported by the Canadian Institutes of Health Research (CIHR) (PJT-162201). Wendy Norman is supported by a CIHR and Public Health Agency of Canada Chair in Applied Public Health Research (2014–2024, CPP-329455-107837). In-kind support was provided by the Women’s Health Research Institute of the British Columbia Women’s Hospital, The Society of Obstetricians and Gynaecologists of Canada and the Canadian Nurses Association.
Data sharing: Our ethics approval has specified that none of the primary data are available to persons or agencies outside of our research team and, therefore, cannot be accessed.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/10/3/E856/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2022 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
Article tools


