


Abstract
Background: The aim of this study was to explore the population-wide distribution in the practice of leisure-time physical activity among Canadian youth and how physical activity level is influenced by contextual features of the environment.
Methods: We studied the self-reported leisure-time physical activity of 54 832 Canadians aged 12 to 17 years. Observations were structured according to a 4-level geographic hierarchy. The outcome studied was a dichotomous indicator that referred to achieving (or not) the recommended daily level of leisure-time physical activity. To investigate the influence of the contextual features, we conducted multilevel logistic regressions.
Results: For both girls and boys, significant variations were observed between health regions and between neighbourhoods within the provinces. Girls who lived in an urban setting showed lower odds of achieving the recommended physical activity level, as did those surveyed during the winter. Boys surveyed during the winter also showed lower odds of achieving the recommended level, but living in an urban setting had no effect on activity levels. Analysis of province-level residuals showed that girls living in Quebec were less likely to achieve the recommended activity level as compared with the national mean, and girls living in Ontario and British Columbia were more likely to achieve that threshold. Boys living in Ontario were more likely to achieve the recommended activity level as compared with the national mean. Youth had up to a 17% increased chance of achieving the recommended physical activity level if they lived in a context with a higher activity achievement level.
Interpretation: Leisure-time physical activity was associated with environmental factors at multiple geographic scales among Canadian youth. The variation was more important at the neighbourhood level. The results provide rationale for further investigation into how leisure-time physical activity is promoted in different contexts.
Leisure-time physical activity (LPA) provides fundamental health benefits for young people,1 including increased physical fitness, reduced adiposity, favourable risk profiles for cardiovascular and metabolic disease, and reduced symptoms of depression.2-5 Among young people, the growth period is a critical time for the development of factors that have a great influence on health in adulthood, such as achieving optimal bone health.6
Understanding what influences youth to engage in LPA contributes to evidence-based planning of public health interventions, as effective programs will target factors known to contribute to physical (in)activity.7 Research into correlates or determinants of LPA has focused mostly on individual-level factors.8 Among them, indicators of socioeconomic status such as education9 and biological factors such as body mass index10 have been associated with differences in participation in LPA. However, contextual factors such as the quality of the built or social environment are less studied but are thought to have widespread effects that may vary across geographic settings.8,11,12
A better understanding of the influence of geographic settings (local to national) on LPA among youth can inform the development of multifaceted interventions, which likely offer the best chance for success.13
The aim of this study was to explore the population-wide distribution of LPA among young Canadians and the influence of area-based characteristics, while taking into account individual factors. The objectives were to describe the geographic variations in LPA among Canadian youth and explore the contribution of contextual factors to explain these variations.
Methods
Data source, study population and sample size
We used the Canadian Community Health Survey (CCHS), 2003 to 2012. The CCHS provides self-reported information for a nationally representative sample of the community-dwelling civilian population aged 12 years or more in the 10 Canadian provinces.14 The sample for this study included youth aged 12-17 years for whom complete information on ethnic origin, education level, body mass index and geographic location was available. Pregnant girls and respondents interviewed by proxy were excluded.
Structure of observations
We structured observations according to a 4-level geographic hierarchy based on Statistics Canada 2006 census administrative units. When a place of residence was located in a census metropolitan area or a census agglomeration, the "neighbourhood" corresponded to the census tract; otherwise it was attributed to the municipality (census subdivision). The combination of census tract and census subdivisions enables the creation of comparable neighbourhood units for the entire Canadian population, whether they are located in an urban or a rural setting, and to consider the idiosyncrasies of the characteristics of place of residence. To take into account changes in the boundaries of the health regions during the study period, we harmonized the geographic structure using a digital boundary file reflecting the boundaries of the health regions as of October 2011.15 A detailed methodology of the geographic structure has been given by Lalonde and Lebel.16 We used ArcMap 10.1 software for geospatial processing. The final hierarchical structure comprised 6004 neighbourhoods within 112 health regions.
Outcome
The dependant variable was a dichotomous indicator of LPA that refers to achieving (or not) the recommended daily level of physical activity. Physical activity level was assessed with the use of an index based on 18 different physical activities for which duration, intensity and energy expenditure were considered.17 Guidelines recommend that young people aged 12-17 should accumulate an average of at least 60 minutes of moderate to vigorous physical activity daily.18,19 An "active" youth is one who achieves an index of energy expenditure of at least 30 kcal/kg per week17 with a frequency of 5 times/week or more. This achievement corresponds to walking briskly (4.3 metabolic equivalents) for 1 hour a day, 7 days a week.20 We estimated physical activity level using a validated index of energy expenditure that considers the frequency, duration and intensity of 18 types of self-reported LPA.21 Given the absence of a measure of exercise intensity in the CCHS, we derived thresholds from a table of metabolic equivalents for various activities.21
Individual variables
To account for the documented influences of individual characteristics on LPA among youth,22-24 we used age, ethnic origin, highest education level of the household and body mass index (based on self-reported height and weight) as control variables.
Cycle and season
The CCHS contains data collected over 12 months (cycle 2003 and 2005) and 24 months (cycle 2007, 2009 and 2011). The exact date of sampling allowed for the inclusion of season in the explanatory model. Three season categories were created: summer (July to October), winter (February and March) and transitional (combining November to January and April to June).
Area-based variables
We considered 3 independent area-based variables. The first was the census metropolitan-influenced zone, which indicates areas that are urban (inside census metropolitan areas or census agglomerations), urban outskirt (commuting flow to urban area 30% or more) and rural (commuting flow to urban area less than 30%).25
The 2 other area-based variables were the neighbourhood material and social deprivation levels. The measures of deprivation are based on the factor score of 2 dimensions resulting from a principal component analysis that estimates the material and social deprivation of the neighbourhood using Canada-wide census information (proportions of adults who live alone, are single parents, do not have a high school diploma and are unemployed, and the mean income of the area).26 The distribution of the neighbourhood deprivation levels was broken into quintiles by province for all census units.
Statistical analysis
We used multilevel analysis to estimate the impact of contextual factors on LPA. The use of multilevel analysis is recommended to account for the clustering of people within areas and to break down the variance in the outcome being studied into between- and within-area components.27,28 Thus, to investigate the influence of the contextual variables, we conducted a series of multilevel logistic regression analyses using the Bayesian estimation procedure as implemented via Markov chain Monte Carlo methods in MLwiN 2.28 software.29 The benefits of this type of analysis as compared to a standard logistic regression are to produce unbiased estimates of the random effects and to provide a measure to compare the relative effectiveness of different models in accounting for the variations in LPA, the deviance information criterion.27
All analyses were stratified by sex to control for the differences in physical maturation between girls and boys during puberty.30
The modelling strategy was based on 4 incremental models to estimate the effect of the additional groups of variables in the fixed part of the models on the between-area variance (random part of the models). The equation for the models is provided in Appendix 1 (available at www.cmajopen.ca/content/4/3/E436/suppl/DC1). The first (null) model showed the distribution of LPA between the geographic levels (random part) without covariates. The second model introduced the control variables of cycle and season, the third model introduced the metropolitan-influenced zone, and the fourth model introduced the neighbourhood material and social deprivation indices.
We used the deviance information criterion to compare the goodness of fit31 of each model with that of the previous model (∆ deviance information criterion). We used the median odds ratio (OR) to translate the area-level variance to an OR scale, which has a consistent and intuitive interpretation.32 The median OR can be compared directly with a regular OR and allows one to estimate the relative importance of the unexplained area-level variation (here province, health region and neighbourhood) compared with other variables included in the model. Variation in the median OR was considered significant when 1.96 times its standard error (SE) remained lower than the between-area variance.
All the models present the odds of achieving the recommended LPA for each characteristic considered (fixed part). We analyzed the between-area variance structure (random part) using the median OR (i.e., province, health region and neighbourhood).
Apart from the null model, the reference category was age 12-15 years, white, living in a highly educated household, reporting a normal weight, surveyed during summer, living in an urban setting (for models 3 and 4) and living in the least-deprived neighbourhoods (model 4).
We used the province-level residuals and associated SE to plot and rank the odds (and 95% confidence interval [CI]) of achieving the LPA threshold for each province. In this way, provinces that differed from the national mean (individual, neighbourhood and regional effects) could easily be identified.
Results
The final sample was 54 832 observations. The distribution of all variables used in the analyses is found in Table 1. Apart from body mass index, where some substantial differences were observed, the distributions were comparable for the 2 sexes. The largest difference was in the outcome: 9908 girls (36.9%) and 14 540 boys(51.9%) achieved the recommended LPA level (Table 1).
Models on girls' leisure-time physical activity
For girls, the null model showed a significant difference in achieving the recommended LPA level between health regions and neighbourhoods but not between provinces (Table 2, random part). Introducing individual characteristics (model 2), and thus controlling for age, ethnic origin and body mass index, showed lower odds of achieving the recommended LPA level among girls surveyed during winter (OR 0.58, 95% CI 0.54-0.62) or the transitional season (OR 0.66, 95% CI 0.62-0.70) as compared to summer. No differences in LPA level were observed over the study period, but significant variation between health regions remained.
Introducing the metropolitan-influenced zone of the neighbourhood (i.e., urban, urban outskirt or rural) (model 3) suggested that a lower likelihood of achieving the recommended LPA level existed for girls in urban areas compared with those in urban outskirt areas (OR 1.12, 95% CI 1.04-1.21) or rural areas (OR 1.13, 95% CI 1.04-1.23). Furthermore, the location of the neighbourhood did not explain much of the significant variation observed between health regions (Var 0.014, SE 0.005), but there was an important increase in the variation explained at the neighbourhood level (Var 0.026, SE 0.009). The median OR indicated that girls living in an urban neighbourhood had a 12% increased chance of achieving the recommended LPA level if they lived in a health region with a higher achievement of recommended LPA level (median OR 1.12) and a 17% increased chance if they lived in a province with a higher achievement level (median OR 1.17).
Introducing the deprivation level of the neighbourhood (model 4) showed no significant association in achieving the recommended LPA level and reduced goodness of fit as compared with model 3 (Table 2).
Models on boys' leisure-time physical activity
For boys, the null model showed a significant difference in achieving the recommended LPA level only between health regions (Table 3). Introducing individual characteristics and season (model 2) showed lower odds of achieving the recommended LPA level among boys surveyed during winter (OR 0.55, 95% CI 0.51-0.59) or the transitional season (OR 0.70, 95% CI 0.67-0.74) as compared with summer. A slight but statistically significant decrease in LPA was observed from 2003 to 2012 (OR 0.98, 95% CI 0.96-0.99). Importantly, the individual characteristics improved the goodness of fit of the model but did not explain the variation between health regions, which suggests a homogeneous distribution of these characteristics between areas.
Unlike for girls, type of neighbourhood was not associated with the odds of achieving the recommended LPA level (model 3). Nevertheless, the model showed significant variation between health regions (Var 0.017, SE 0.005) and between neighbourhoods (Var 0.023, SE 0.009) within provinces. The median OR indicated that boys had a 13% increased chance of achieving the recommended LPA level if they lived in a health region with a higher achievement of recommended LPA level (median OR 1.13) and a 16% increased chance if they lived in a neighbourhood with a higher achievement level (median OR 1.16).
The deprivation level of the neighbourhood (model 4) showed no significant association with achieving the recommended level of LPA and reduced the goodness of fit as compared with model 3 (Table 3).
Variation between provinces
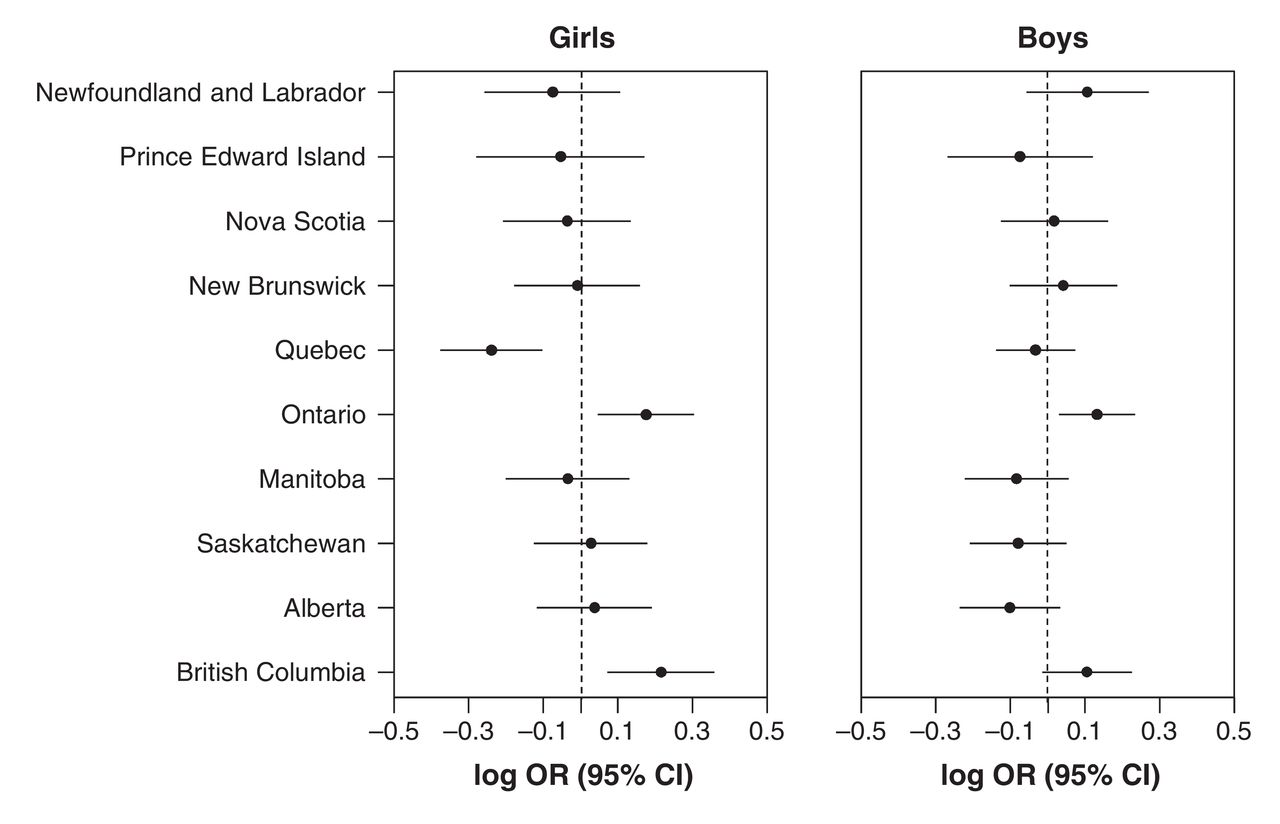
Analysis of province-level residuals showed that girls living in Quebec were less likely to achieve the recommended level as compared with the national mean, and girls living in Ontario and British Columbia were more likely to achieve that threshold (Figure 1). Boys living in Ontario were more likely to achieve the recommended LPA level as compared with the national mean (Figure 1).

Province-level residuals of the logarithm of the odds ratio (OR) for achieving the recommended level of leisure-time physical activity among girls and boys. CI = confidence interval.
Interpretation
In this study, we explored differences in reported LPA among Canadian youth according to their geographic context and focused mainly on contextual factors. We applied a 4-level model that controlled for age, ethnic origin, household education level and body mass index. We found that, beyond individual characteristics, the contextual characteristics were associated with the odds of accumulating an energy equivalent of at least 60 minutes of moderate to vigorous LPA. Moreover, these contextual influences were sometimes different between girls and boys.
As in other Canadian investigations,33,34 substantially fewer girls than boys achieved the recommended LPA level (36.9% v. 51.9%). This finding reinforces the need to consider sex-specific requirements when planning public health interventions related to LPA. A proposed area of improvement involves strategies to ensure equitable access to resources, including availability of and access to suitable physical education classes and organized sports that may be subject to sex-related inequities.35,36
Season had a highly significant influence. For both sexes, winter was observed as a major barrier to performing LPA, even when the potential addition of compulsory physical education classes was taken into account. This finding supports previous evidence of an influence of seasonality on LPA among various populations, including young Canadians.37,38 For this reason, seasonality needs to be taken into account when developing interventions and programs targeting physical activity.
Contrary to previous findings,39 living in an urban outskirt or rural area as compared to an urban neighbourhood was associated with higher odds of meeting physical activity guidelines among girls. This observation suggests that facilities in urban areas may be more suitable for boys,40 for whom this measure was not significant in our study. Analysis of the between-neighbourhood variance showed that most of the variation in LPA among Canadian youth occurred between urban neighbourhoods. This suggests that greater inequalities in opportunities for LPA exist in urban neighbourhoods.
The relatively poor odds of achieving the recommended LPA level among girls living in Quebec seen on analysis of provincial-level residuals raises the question as to why girls in that province tend to be less active than other Canadian girls. Investigation is warranted into how physical activity is promoted in Quebec as compared to in Ontario and British Columbia, where girls had higher LPA levels than the national mean.
The introduction of area-based indices of material and social deprivation led to poorer goodness of fit of the overall models. As such, we have drawn no conclusions about their association with the odds of achieving the LPA guidelines. A recent analysis of the influence of these indices among Quebec high school students showed that those from materially and socially privileged backgrounds were proportionally more active than those from disadvantaged backgrounds.41 However, the authors did not account for the country-wide variation and the hierarchical structure of the information. More context-specific investigations are required to explore the causes of these contrasting observations.
Limitations
Several limitations need to be kept in mind when interpreting our results. Although the sample was distributed over a 10-year period, the cross-sectional design of the study limits our ability to establish causal inferences, particularly with respect to contextual effects. Also, the CCHS data on LPA aim to account for all activities completed over a 3-month period before the administration of the survey. For that reason, the accuracy of recall regarding duration and frequency of physical activity is questionable, as recall of nonrepeating activities would likely be more difficult and there would likely be a bias toward LPA in which participants are registered (e.g., lessons, league sports). Also, the survey does not indicate whether the activity is performed as part of a compulsory physical education class, even though that might have a significant influence on the age group studied. Last, we did not account for physical activity performed for utilitarian purposes such as active transport, which is more common in central, often deprived, neighbourhoods.42 The inclusion of this type of activity would have given a more complete picture of daily physical activity and may have enhanced the effects of contextual features.
Conclusion
This exploratory analysis provides insight into the contextual differences regarding the level of LPA among Canadian youth based on a large sample, a combination of individual and contextual information, and a multilevel framework. The results highlight important inequalities in LPA levels among Canadian youth and show context-specific variations between provinces, health regions and neighbourhoods. These findings provide valuable new information to guide future research aimed at better understanding why young people's LPA levels are unequally distributed in Canada.
Supplemental information
For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/4/3/E436/suppl/DC1
Acknowledgements
Funding: This study was partly funded by the Evaluation Platform on Obesity Prevention in the Quebec Heart and Lung Institute Research Center, Laval University, and the Fonds de recherche du Québec - Santé (grant number FRQS-31022).
Footnotes
Competing interests: None declared.
Contributors: Charles Nadeau, Owen Waygood and Alexandre Lebel conceived and designed the study. Charles Nadeau, Ramona Fratu and Alexandre Lebel obtained access to the data, and Charles Nadeau and Ramona Fratu performed the statistical analyses. All of the authors contributed to the interpretation of the results, drafting the paper and reviewing it critically for inportant intellectual content. All of the authors gave approval of the final version to be published and agreed to act as guarantors of the work.
References
- Copyright 2016, Joule Inc. or its licensors
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.