


Abstract
Background The clinical armamentarium for anticoagulation has expanded substantially since the recent approval of dabigatran, rivaroxaban and apixaban for the prevention of stroke in atrial fibrillation. However, patients in the general population often differ from participants in clinical trials. In this study, we assessed the uptake of these novel oral anticoagulants in Ontario, Canada, within the first 2 years after dabigatran’s approval for this indication.
Methods Using data on province-wide prescription volumes, we conducted a time-series analysis of prescription trends between October 2010 and September 2012 for all orally administered anticoagulants (warfarin, dabigatran and rivaroxaban) that were available in this period. We stratified dabigatran prescription rates by age group (20–39, 40–59, 60–64, 65–84 and ≥ 85 yr). We compared the proportion of dabigatran prescriptions to patients aged 65 or older with similar data from the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) study.
Results Over the 24-month study period, we found that prescriptions for the novel anticoagulants rose more than 20-fold, to represent 21.1% of all prescriptions of oral anticoagulants by September 2012. The rise in prescriptions was due primarily to an increase in dabigatran use. Prescription rates of dabigatran were highest among people aged 85 years or more, a group at increased risk of bleeding who are markedly older than the average participant in the clinical trial in which the drug was tested (71 yr). In September 2012, most of the dabigatran prescriptions were for the lower-dose formulation (110 mg) in the older groups (58.8% of dabigatran prescriptions in the 65–84 age group and 93.6% in the oldest group).
Interpretation We observed rapid growth in the uptake of the novel oral anticoagulants since their approval for use in patients with atrial fibrillation, especially among those aged 85 years or more. This increase in use in the oldest group, a population at high risk of bleeding, signals the need to evaluate outcomes of use of novel oral anticoagulants in the clinical setting.
Atrial fibrillation affects about 350 000 Canadians, with a prevalence heavily skewed toward higher age groups.1,2 Anticoagulants required for the prevention of stroke in these patients eclipse all other drugs in their frequent and clinically significant benefit and harm: a March 2013 report by the Canadian Institute for Health Information highlighted anticoagulants as the drug class most commonly associated with hospitalizations in seniors due to adverse events from 2006 to 2011.3
Dabigatran and rivaroxaban have been approved for use in patients undergoing orthopedic surgery since 2008. The approval of novel oral anticoagulants for atrial fibrillation began in October 2010 with dabigatran, followed by rivaroxaban in January 2012 and apixaban in December 2012.4 The recommendation of their use as first-line therapy in the Canadian Cardiovascular Society guidelines represents an expansion of the clinical armamentarium for stroke prophylaxis.5 However, patients in real clinical settings often differ from participants of randomized trials used to inform the development of these guidelines.6 With respect to novel oral anticoagulants, age is of particular interest given the increased risk of bleeding among older patients and the lack of an antidote.7–10
We conducted this study to determine the prescribing patterns of oral anticoagulants in Ontario, Canada’s largest province, since the arrival of novel oral anticoagulants. We focused on changes in prescription rates by age group.
Methods
Data collection
We obtained data on dispensed medications for Ontario residents aged 20 years or more who filled prescriptions for an oral anticoagulant (warfarin, dabigatran or rivaroxaban) between October 2010 (when the first novel oral anticoagulant, dabigatran, was approved for use in atrial fibrillation) and September 2012. Aggregate monthly prescription volumes were acquired from IMS Brogan (Canadian CompuScript Audit), which collects prescription records from nearly two-thirds of Canadian retail pharmacies regardless of payer type. These data are extrapolated to jurisdictional prescription volumes by means of standardized weighting methods and are used frequently to evaluate prescription trends.11–13
Statistical analysis
We used linear regression, accounting for first-order autoregressive residuals, to evaluate prescription trends in a time-series analysis. When temporally sequenced data are used in regression analysis, often the error term is not independent through time, adversely biasing the standard error estimates. The autoregressive error model corrects for this serial correlation or autoregression.14
We calculated monthly prescriptions per 100 000 population for all oral anticoagulants. Because rivaroxaban prescriptions accounted for only 3.9% of total prescriptions by the end of the study period, they were not included in subsequent analyses. We stratified dabigatran prescription rates by age group (20–39, 40–59, 60–64, 65–84 and ≥ 85 years). Furthermore, using the χ2 test, we compared the percentage of dabigatran prescriptions filled by people aged 65 or older with similar data reported from the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) study.15 A sensitivity analysis was also undertaken that evaluated only new prescriptions and excluded refill prescriptions. Population data were based on the 2011 Canadian census.16
Results
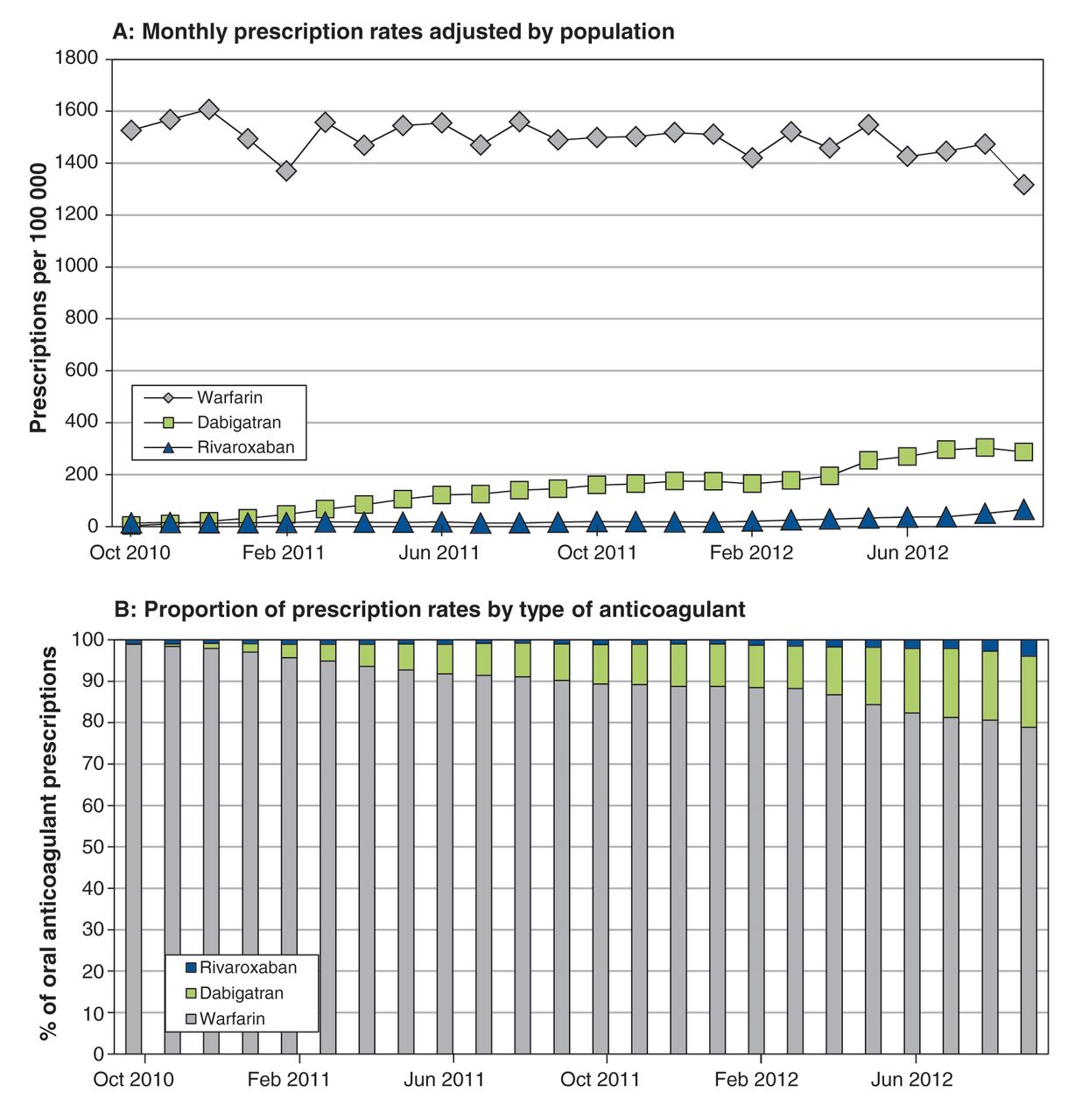
During the 24-month study period, monthly prescriptions of novel oral anticoagulants increased more than 20-fold, from 16 to 336 prescriptions per 100 000 population. The change in prescribing patterns was due primarily to an increase in dabigatran use, which rose from 3 to 274 prescriptions per 100 000 population (ptrend < 0.001; Figure 1A). By September 2012, dabigatran represented 17.2%, and rivaroxaban 3.9%, of all oral anticoagulant prescriptions (Figure 1B). Monthly prescriptions of warfarin over the study period decreased from 1526 to 1316 per 100 000 (ptrend = 0.007).

Monthly prescription rates for warfarin, dabigatran and rivaroxaban in Ontario among adults aged ≥ 20, adjusted by population (A) and proportion of prescription rates by type of anticoagulant (B).
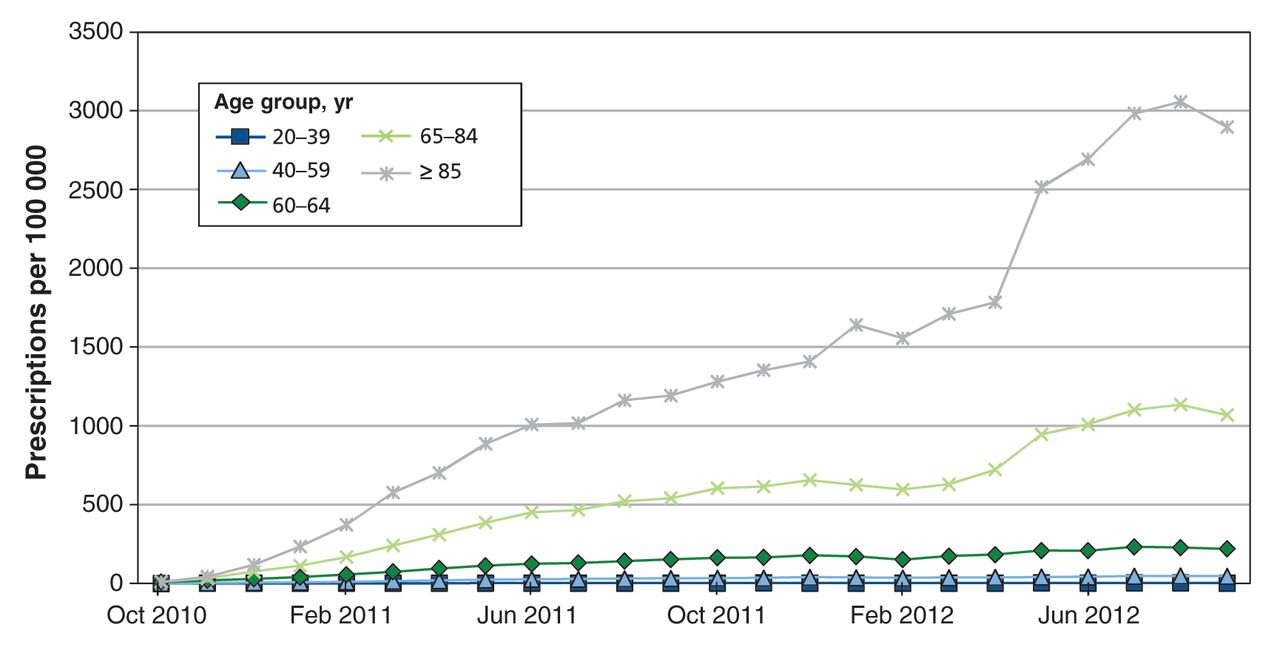
Dabigatran prescription rates were highest among patients aged 85 or more, and next highest among those 65–84 years of age (Figure 2). Since April 2012, the proportion of dabigatran prescriptions filled by patients 65 or older exceeded the proportion of participants in the same age group enrolled in dabigatran arms of the RE-LY trial (87.3% v. 83.2%, p < 0.001). In September 2012, most of the dabigatran prescriptions were for the lower dosage (110 mg/d) in the older groups in our study (58.8% of prescriptions in the 65–84 age group and 93.6% in the oldest group).

Age-stratified monthly prescription rates for dabigatran in Ontario among adults aged ≥ 20, adjusted by population.
When we restricted the analysis to new prescriptions of dabigatran, the trends by age group were similar to those in the main analysis (Appendix 1A, available at www.cmajopen.ca/content/1/3/E115/suppl/DC1). Although the rates of new prescriptions across age groups appeared to plateau over time, the relative distribution of new dabigatran prescriptions across age groups remained stable over time, with the largest proportion in the oldest group (Appendix 1B).
Interpretation
We found a rapid uptake of dabigatran in Ontario in the 24 months after its approval for atrial fibrillation, with onset preceding its coverage by the Ontario Public Drug Programs in April 2012. The rate of warfarin prescription declined with the rise in use of novel oral anticoagulants, and use of rivaroxaban did not increase substantially from baseline over the study period, even after its approval for use in atrial fibrillation in January 2012. We also observed that dabigatran was heavily prescribed to patients aged 85 or more, especially the lower-dose formulation.
Results of our study are consistent with those in 2 reports of prescription trends for novel oral anticoagulants. A nationally representative survey in the United States reported an increase in physician visits involving dabigatran prescription as a proportion of oral anticoagulants, from 3.1% in the fourth quarter of 2010 to 18.9% one year later.17 At end of the study period, 87% of dabigatran-related physician visits were by patients 65 or older. In New Zealand, the prevalence of dabigatran use among patients aged 80 and over was 1300 per 100 000 population, and 80.1% of prescriptions were for patients 65 or older.18
In keeping with the Canadian Cardiovascular Society guidelines first published in January 2011 and updated in April 2012, which recommend the use of novel oral anticoagulants over warfarin,5,19 dabigatran has been actively integrated into the care of patients with atrial fibrillation. Although novel oral anticoagulants represent an opportunity to improve anticoagulation uptake, the US Food and Drug Administration (FDA) noted that postmarketing use of dabigatran “might be different from its use in the RE-LY trial … e.g., different patient populations.”20 Our results corroborate this perspective: we found that prescription rates of dabigatran were most accelerated among patients 85 or older, a group at increased risk of bleeding who are markedly older than the average participant in the clinical trial in which the drug was tested (71 yr).21
In contrast to the overall RE-LY trial results, which suggested a lower risk of major bleeding with dabigatran 110 mg than with warfarin,22 a recent network meta-analysis by the Canadian Agency for Drugs and Technologies in Health found comparable risks of major bleeding (the definition of which includes intracranial hemorrhage) among patients 75 years or older.23 This corroborates findings of a subgroup analysis involving RE-LY participants 80 or older submitted to the US FDA by the trial sponsor that showed equivalent risk of major bleeding with dabigatran 110 mg (5.25% per year) compared with warfarin (4.70% per year).24 Because no effective reversal agent exists for dabigatran,9 this difference in safety outcomes between the overall RE-LY trial cohort and the subgroup experiencing the most rapid “real-world” uptake may have an unexpected impact in clinical practice as knowledge from the RE-LY trial is swiftly adopted.
Limitations
Our study has several limitations. First, the use of prescription volume rather than patient volume creates potential bias in cases of differential prescribing frequency. However, our results are comparable to those generated by patient-based methodologies,17 and our analysis that was restricted to new prescriptions of dabigatran yielded trends similar to those of the main analysis.
Second, we were unable to stratify prescription volume by indication, and thus the data included prescriptions for novel oral anticoagulants in patients undergoing orthopedic surgery. However, their contribution to the overall prescription pattern was likely small: dabigatran and rivaroxaban have been approved for use in patients undergoing orthopedic surgery since 2008, but prescriptions remained low until their approval for use in atrial fibrillation.
Finally, our study period for capturing data on prescriptions ended just as rivaroxaban prescribing for atrial fibrillation would have been starting and before apixaban was approved for use in atrial fibrillation.
Conclusion
We observed rapid growth in the uptake of the novel oral anticoagulants, in particular dabigatran within the 2 years after its approval for use in patients with atrial fibrillation. Although results of the RELY-ABLE study, which looked at the long-term effects of dabigatran in patients completing the RE-LY trial, suggest long-term safety and efficacy of dabigatran in the phase IV trial setting,25 growth in the uptake of novel oral anticoagulants in very old patients, a group at high risk of bleeding, signals the need to evaluate outcomes in clinical practice to better guide the use of these agents.
Supplemental information
For reviewer comments and the original submission of this manuscript, please see at www.cmajopen.ca/content/1/3/115/suppl/DC1
See related commentary in CMAJ by Coppens and colleagues at www.cmaj.ca/lookup/doi/10.1503/cmaj.131291.
Acknowledgements
The authors are grateful to IMS Brogan for providing prescribing data, and Andrew Day at the Kingston General Hospital Clinical Research Centre for assistance with statistical analysis. Yan Xu is supported by a studentship from the Heart and Stroke Foundation of Ontario as well as the Ontario Drug Policy Research Network; the latter is funded by a grant from the Ontario Ministry of Health and Long-Term Care Drug Innovation Fund. The opinions, results and conclusions reported in this paper are those of the authors and are independent from sources of funding or data. No endorsement by the Ontario Ministry of Health and Long-Term Care or IMS Brogan is intended or should be inferred.
Footnotes
-
Competing interests: Christopher Simpson reports receiving speaker fees from Boehringer Ingelheim and Bayer Canada, and serving on an advisory board for Bristol-Myers Squibb. Dar Dowlatshahi reports receiving travel and speaker honoraria from Boehringer Ingelheim and has served on advisory boards for Bayer Canada, Bristol-Myers Squibb and Pfizer. No competing interests declared by Yan Xu, Anne Holbrook and Ana Johnson.
-
Contributors: Yan Xu contributed to conception and design of the study. Yan Xu and Ana Johnson acquired the data. Yan Xu was involved in data analysis, and all authors contributed to data interpretation. Yan Xu drafted the manuscript, which all of the authors provided revisions for important intellectual content. All of the authors approved the final version submitted for publication.
-
Funding: This study was funded by the Canadian Institutes of Health Research — Drug Safety and Effectiveness Network (grant no. PAS 126297).
References
- © 2013 Canadian Medical Association or its licensors
In this issue

{kind=link}
{kind=link}
Article tools





