


Abstract
Background One-third of Canadian children are overweight or obese. This problem carries considerable concern for negative impacts on current and future health. Promoting healthy growth and development is critical. This review synthesized evidence on the effectiveness of behavioural interventions for preventing overweight and obesity in children and adolescents.
Methods We updated the search of a previous Cochrane review. Five databases were searched up to August 2013. Randomized trials of primary care–relevant behavioural (diet, exercise and lifestyle) interventions for preventing overweight and obesity in healthy normal- or mixed-weight children or youth aged 0–18 years were included if 12-week postbaseline data were provided for body mass index (BMI), BMI z-score, or prevalence of overweight or obesity. Any study reporting harms was included. Meta-analyses were performed if possible. Features of interventions showing significant benefits were examined.
Results Ninety studies were included, all with mixed-weight populations. Compared with controls, interventions showed a small but significant effect on BMI and BMI z-score (standardized mean difference –0.07, 95% confidence interval [CI] –0.10 to –0.03, I2 = 74%), a reduction in BMI (mean difference –0.09 kg/m2, 95% CI –0.16 to –0.03, I2 = 76%) and a reduced prevalence of overweight and obesity (risk ratio [RR]; RRintervention – RRcontrol 0.94, 95% CI 0.89 to 0.99, I2 = 0%; number needed to treat 51, 95% CI 29 to 289). Little evidence was available on harms. There was variability across efficacious interventions, although many of the interventions were short-term, involved school-aged children and were delivered in educational settings.
Interpretation Behavioural prevention interventions are associated with small improvements in weight outcomes in mixed-weight populations of children and adolescents. No intervention strategy consistently produced benefits. Registration: PROSPERO no. CRD42012002754
Childhood and adolescence are characterized by substantial physical growth and development. Weight gain is expected and desirable as children get taller and older. However, children and teens who are overweight or obese face social, emotional and physical challenges, and if excess weight is retained into adulthood, there is a greater risk for obesity-related health problems.1–5 For those aged 5–19 years, the World Health Organization defines overweight as > 85th centile and obesity as > 97th centile; for children aged 2–5 years the cut-offs are more conservative (overweight > 97th centile, obesity > 99.9th centile).6 Using these standards, almost one-third (31.5%) of the elementary and secondary school-aged children and youth in Canada are overweight or obese. This situation calls for preventive efforts to promote healthy weight in childhood and adolescence, and also as a means to build a strong foundation for maintaining healthy weight in adulthood.
Treatment of obesity in children and adolescents is an active area of research, and a number of systematic reviews have been published recently.7–13 In addition, reviews have been published about the prevention of obesity in children,14 including community-,15 home-16 and school-based17–19 interventions, and using diverse approaches such as educational programs,20 reduction of screen time,21 and behavioural strategies associated with diet and physical activity.22 This review provides a synthesis of the effectiveness of interventions for the prevention of childhood obesity that are feasible for use in primary care or for referral in the community and examines the features of efficacious interventions.
Methods
Search strategy
A recent high-quality (11/11 AMSTAR rating)23 Cochrane Review examined interventions for preventing obesity in children.17 Cochrane Reviews are often considered gold standard, and, upon evaluation, it was determined that their search strategy addressed our key questions. For these reasons and to avoid duplication, our protocol was designed to update their search. We searched Embase, MEDLINE, Cochrane Central Register of Controlled Trials, PsycINFO and CINAHL from Jan.1, 2010 (just prior to the date of the last Cochrane search) to Aug. 1, 2013. The Medline strategy appears in Appendix 1 (available at www.cmajopen.ca/content/3/1/E23/suppl/DC1). The Cochrane group also provided a list of citations being considered for their next update. Reference lists of included studies and pertinent reviews were searched for studies not captured by our search. A focused grey literature search of Canadian sources was undertaken for recent reports on obesity in Canada.
Population, intervention, comparator, outcome and setting statement
The PICOS (population, intervention, comparator, outcome, setting) framework was (P) normal- or mixed-weight children and youth aged 0–18 years; (I) behavioural interventions for prevention of weight gain; (C) no intervention, usual practice or minimal component; (O) change in body mass index (BMI), BMI z-score or prevalence of overweight and obesity, and harms of interventions; and (S) generalizable to primary care in Canada. Additional details are provided in Box 1.
Inclusion and exclusion criteria
The inclusion and exclusion criteria for this review are provided in Box 2.
Study selection, quality assessment and data abstraction
Titles and abstracts were reviewed independently in duplicate. Citations marked for inclusion by either team member went on to full-text screening, which was also done independently in duplicate. Randomized trials were assessed using the Cochrane Collaborations’s tool for risk-of-bias assessment.24 Overall strength of the evidence (assessed as high, moderate, low or very low quality) was determined using the Grading of Recommendations Assessment, Development and Evaluation framework (GRADEpro [computer program], version 3.2 for Windows; available at www.ims.cochrane.org/revman/gradepro).25 Interrater disagreements were resolved through discussion. One team member completed full abstraction and a second verified all extractions. All data were re-verified before analysis.
Data analysis
For meta-analyses, means and standard deviations (SD) were used for continuous outcomes (i.e., BMI and BMI z-score), and counts data were used for the binary outcome (i.e., prevalence). Whenever possible, immediate posttreatment data were used, otherwise the data point closest to the end of the intervention was selected. If studies reported results for boys and for girls, we entered these data separately into the meta-analyses. For studies with more than one intervention arm, we combined data from similar groups to do a pair-wise comparison with the control group.24 If groups were substantially different, we included the data for each arm compared with the control group but split the sample size for the control to avoid a unit-of-analysis error and double counting.24 Cochran’s Q (α = 0.05) and I2 (≥ 75% = substantial heterogeneity) statistics were used to quantify statistical heterogeneity between studies. Statistical analyses were performed using Review Manager version 5.3, STATA version 12 and GRADEpro.
Standardized mean difference (SMD) was chosen as a summary measure of effect to allow us to combine data for BMI and BMI z-score in a single meta-analysis; if a study reported both outcomes, we used the nonstandardized data. This strategy, which is consistent with the approach taken in 2 major reviews on this topic,13,17 increases the pool of studies, thereby increasing the power to detect a difference in weight change between groups. A second meta-analysis included only studies that reported change in BMI and used mean difference (MD) as the summary measure of effect. The DerSimonian and Laird random-effects model with inverse variance26 was used to generate SMDs for BMI and BMI z-score (< 0.2 = very small effect, ≥ 0.2 and < 0.5 = small effect, ≥ 0.5 and < 0.8 = medium effect; ≥ 0.8 = large effect)27 and MD for BMI alone. For the outcome of BMI and BMI z-score, we did sensitivity analyses based on age groups (0–5, 6–12 and 13–18 yr), intervention type (diet, exercise, diet plus exercise and lifestyle), intervention setting (noneducational, educational only and educational plus other) intervention duration (≤ 12 mo and > 12 mo), sex and study risk of bias rating (low, unclear and high). For BMI alone, we did a single sensitivity analysis based on intervention type.
The outcome of change in the prevalence of overweight and obesity in children and adolescents pre- and postintervention compared with the control group underwent meta-analysis using the difference in risk ratio (RRIntervention – RRControl) and its standard error (SE), and the summary measures of effect were generated using the DerSimonian and Laird random-effects model with inverse variance.26 The estimate of absolute risk reduction and number needed to treat were calculated based on the prevalence of overweight and obesity postintervention.
Efficacious interventions were identified from studies in the meta-analysis of BMI and BMI z-score that significantly favoured the intervention group at postassessment. The choice of intervention characteristics to examine (target sex and age, estimated number or frequency of sessions, group sessions, family involvement and staff training) was informed by a similar list in another systematic review,13 to which we added intervention duration, type and setting, based on our belief that primary care professionals might want to consider these features when making referrals or recommending programs to their patients and their families.
Results
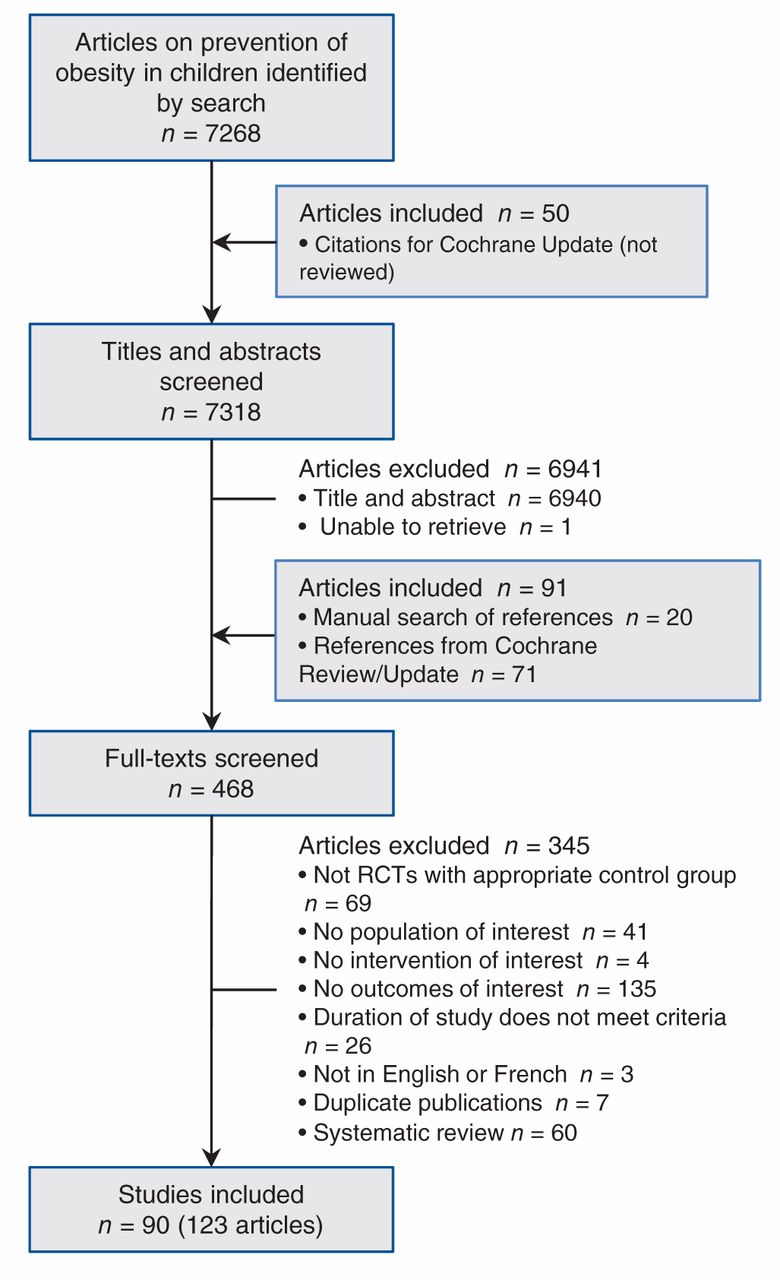
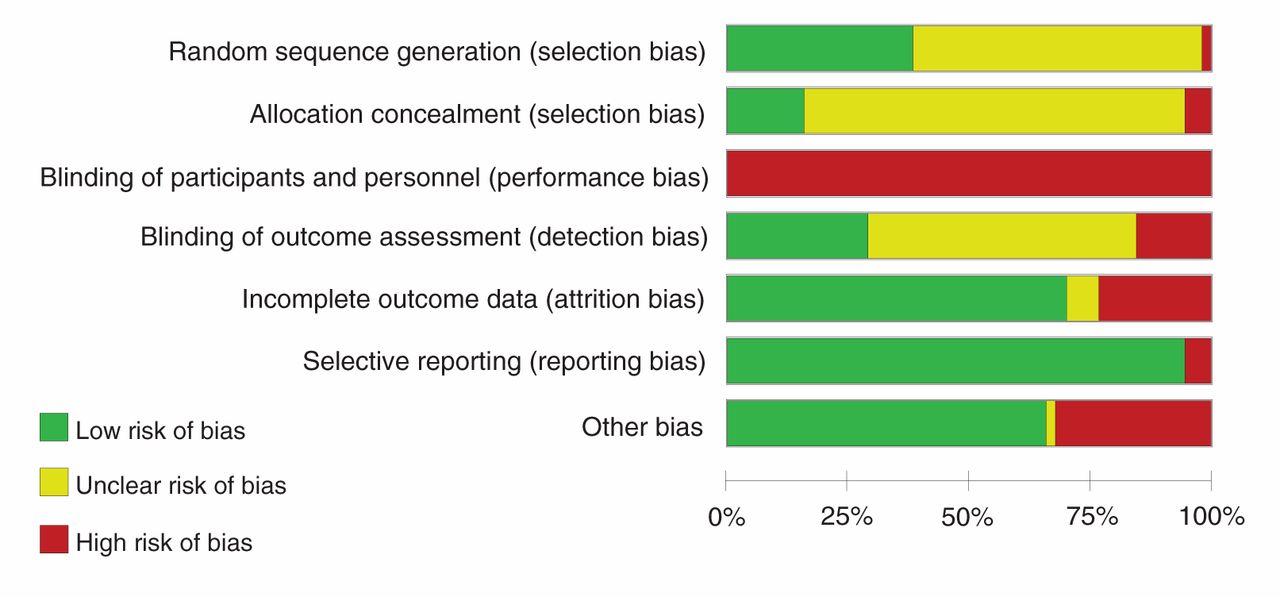
Figure 1 presents the search and selection results. We included 123 papers representing 90 studies. This total includes 28 studies from the 2011 Cochrane review,28–55 16 studies the Cochrane group was considering for their update,56–71 10 studies from the pool of as yet unreviewed citations from the Cochrane group (some of which were also found by our search)72–81 and 36 unique studies identified in our search.82–117 Ratings for risk of bias in individual studies were mostly unclear or high (Figure 2; see Appendix 2 for details about individual studies, www.cmajopen.ca/content/3/1/E23/suppl/DC1). Table 1 provides a summary of the features of the included body of evidence (see Appendix 3 for details about individual studies, www.cmajopen.ca/content/3/1/E23/suppl/DC1). The weight range of children in the studies varied (i.e., they were unselected or mixed-weight populations, not populations solely of children who were normal weight).
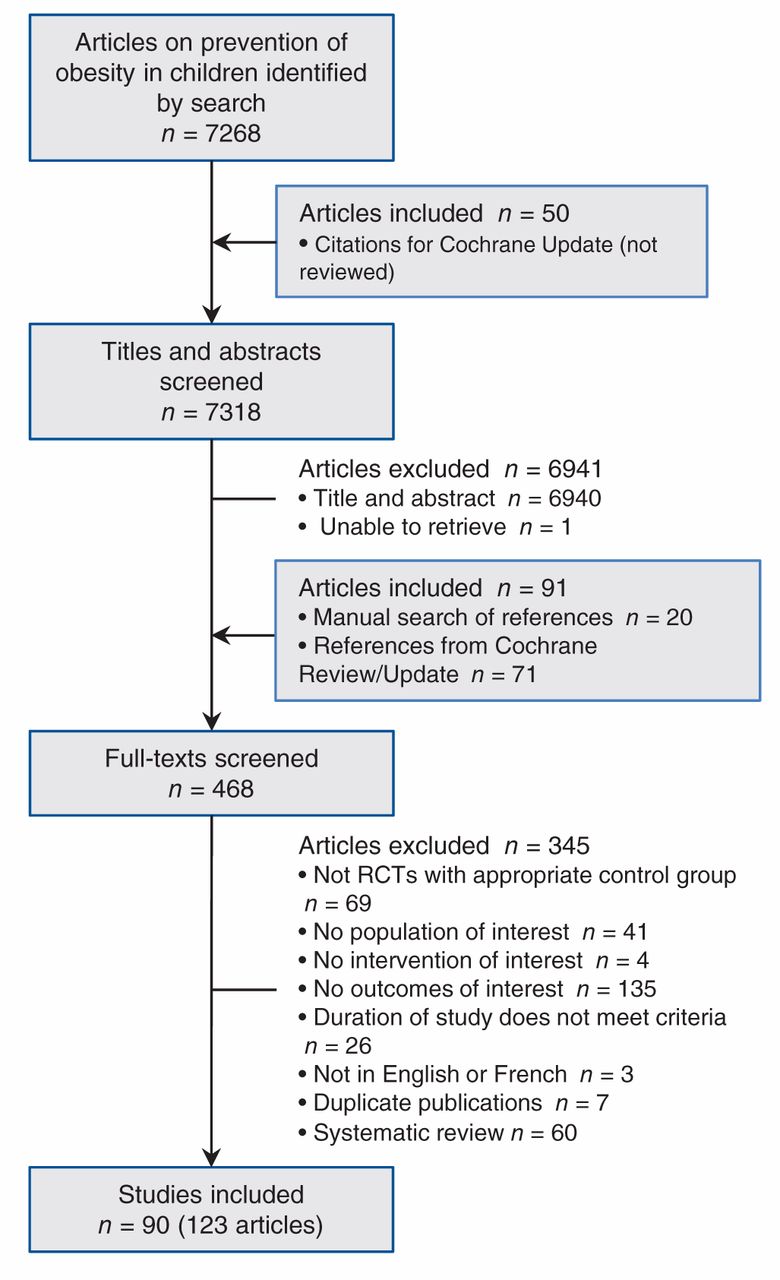
Selection of studies evaluating interventions to prevent overweight and obesity in children and youth. RCT = randomized controlled trial.

Aggregated risk-of-bias assessment of included studies. Summary data from each study are available in Appendix 2 (www.cmajopen.ca/content/3/1/E23/suppl/DC1).
Change in body mass index and body mass index z-score
Seventy-six studies were included in the meta-analysis assessing change in BMI and BMI z-score.28–47,49–62,64–66,68–74,77–90,94,95,97,98,100–104,107–109,111–113,115–117 Figure 3 shows a small but significant effect in the intervention group compared with control groups (also Table 2). Tests for subgroup differences showed no differences in effect on BMI and BMI z-score across treatment type, intervention duration, participants’ sex or age, or study risk-of-bias rating, but did show a difference depending on intervention setting (Table 2). Interventions in education settings showed significant improvements for program participants compared with controls, whereas programs located in noneducation settings or in combined education plus other settings showed no difference (Table 2). Subanalysis by intervention type found only diet-plus-exercise participants had a significantly lowered BMI and BMI z-score compared with controls (Table 2). Both boys and girls who took part in interventions showed significantly better results than control groups (Table 2). Improvements were observed for children participating in interventions who were aged 6–12 years and for youth, but not for children aged 0–5 years (Table 2). Interventions lasting 1 year or less demonstrated significant benefits for participants compared with control groups, but longer programs did not (Table 2). Finally, more improvement was observed in the intervention group compared with the control group across all levels of study risk of bias (Table 2).
Eight trials met the inclusion criteria but could not be pooled because 1) baseline or follow-up values were missing, and no change from baseline data were provided; 2) only an effect size or p value was reported without group-level data, or 3) only general statements were made that no difference between study groups was observed at postassessment.63,67,76,96,99,106,110,114 Most of these studies reported no significant difference in BMI changes or BMI z-scores between intervention and control groups.63,67,76,99,110,114 One study by Wen and colleagues96 reported a significantly lower mean BMI for children participating in the intervention compared with control participants. In a randomized intervention study, Bellows and colleagues106 observed different effects based on age and weight status; 3- to 5-year-olds and children who were already overweight or obese showed no increase in BMI, but 4- to 5-year-olds and children who were normal weight showed increasing BMI.
Change in body mass index
Fifty-seven trials were included in the meta-analysis assessing only change in BMI.28, 30,32–38,40–47,49–56,58–60,62,64,66,68–73,77–80,82,83,87,89,94,95,97,98,101,103,104,107,108,113,115,116 A small but significant change favouring intervention participants was observed compared with control-group participants (Table 2). After a subgroup analysis based on intervention type (diet, exercise, diet plus exercise or lifestyle), the effect was only significant for diet-plus-exercise programs compared with control conditions (MD –0.15 kg/m2, 95% confidence interval [CI] –0.25 to –0.03, I2 = 76%).
Change in prevalence of overweight and obesity
Thirty studies were included in the meta-analysis assessing change in prevalence of overweight and obesity (Figure 4).28,29,33,38,42,45,46,48,57,58,61,62,69,71,72,75,78,81,85–87,91–95,102,105,115,116 Intervention participants were more likely to show a reduction in prevalence and less risk of being overweight or obese compared with control participants: 39.8% of participants were overweight or obese at preintervention to 35.3% of participants at postintervention compared with 33.4% overweight or obese at baseline to 31.5% at postassessment (ratio of RR 0.94, 95% CI 0.89 to 0.99, I2 = 0%; absolute RR 1.96%, number needed to treat 51, 95% CI 29 to 289). In a cluster-randomized trial that could not be pooled, Bürgi and colleagues94reported no difference in the change in prevalence of overweight in children who had completed a lifestyle intervention focusing on physical activity, nutrition education, screen time and sleep.

Effect of prevention interventions on change in prevalence of overweight or obesity. Values less than 1 indicate a change in prevalence of overweight or obesity in favour of the intervention. 1 = intervention arm 1; 2 = intervention arm 2; F = female; M = male; ob = obese, ow = overweight (overweight and obese are not combined in either extension); RR = risk ratio.
Harms
Only 3 studies were found that addressed the identified harms. A school-based diet intervention study by Foster and colleagues42reported on negative impacts on body image and suggested that there was no difference between groups, but no data was provided. A study by de Heer and colleagues56 reported a diet-plus-exercise intervention was delivered without any major incidents. The third study by Yin and colleagues117 examined the effects of a physical activity program on more than 500 elementary school children reported 43 events and adverse event incident rates of 0.03 in year 1, 0.02 in year 2 and 0.01 in year 3. No examples of adverse events were provided in the study, but the authors reported that 67% were mild in nature, 21% were moderate and 12% were severe.117
Features of efficacious interventions
Sixteen studies showed a significant benefit of intervention compared with the control groups in terms of a reduced BMI and BMI z-score at postassessment (see Figure 3). Interventions in these studies were designated as efficacious; Table 3 presents their individual features. Overall, 14 programs were situated in educational settings, 15 involved group sessions, 4 incorporated family involvement and 6 specified that staff training was provided. Intervention duration ranged from 12 weeks to 3 years. Ten programs lasted 1 year or less and 8 were in place for 6 months or less. Most interventions (n = 13) were offered to mixed-sex groups and more than half (n = 9) involved children who were elementary school age. Intervention type varied (diet [n = 4], exercise [n = 5], diet plus exercise [n = 5] and lifestyle [n = 2]) as did location (Europe [n = 7], United States [n = 4], Australia [n = 2], China [n = 1], Egypt [n = 1] and Israel [n = 1]).
Interpretation
Main findings
We found a substantial number of studies that involved mixed-weight populations and no studies exclusively involving normal-weight children; therefore, we cannot determine the effectiveness of the interventions for prevention of weight gain for that specific group. Compared with the control groups, prevention interventions in mixed-weight populations of children and adolescents showed a small effect in terms of a lowered BMI and BMI z-score and a reduced prevalence of overweight and obesity. For overweight or obese children and youth, these changes are not clinically meaningful, although for preventing unhealthy weight gain, they could become clinically meaningful over time. Program benefits must be considered against harms. Only 3 of the 90 included studies reported on adverse consequences of participation; therefore, we are unable to draw conclusions regarding harmful effects of prevention interventions. Many efficacious interventions lasted less than 1 year, involved children who were elementary school age and were implemented in educational settings, but there was too much variation across programs to isolate any determining features of effectiveness.
Our updated review added 62 studies to the evidence included in the most recent Cochrane Review.17 The overall findings of this review are similar to other recent reviews that included school-based interventions for the prevention of obesity in children and adolescents.14,17,18 Some differences were observed across subgroup analyses: for example, we found a small but significant effect for change in BMI and BMI z-score for youth aged 13–18 years that was not observed in the Cochrane Review.17 We also used a more rigorous approach for subgrouping intervention type by adding a lifestyle category to better reflect current evidence. Furthermore, going beyond conventional measures of adiposity (e.g., BMI and BMI z-score) used by previous reviews,13,17 we also looked at prevalence of overweight and obesity to help inform the direction of evidence in a more intuitive way. Consistent with other reviews, we found no studies involving primary prevention of weight gain in children who were normal weight. It is not surprising that primary prevention programs have not been evaluated. It would be hard to separate out normal-weight children in a school population, to motivate them to attend an out-of-classroom intervention, or to motivate most parents of these children to take them to a community intervention for weight maintenance. It is unlikely that a randomized trial will be done.
Limitations
First, the included studies involved mixed-weight populations; thus, we cannot directly answer the question of weight-gain prevention specifically in normal-weight children and adolescents. Second, risk of bias was unclear in most studies, primarily because of the lack of information about or lack of procedures to ensure random sequence generation, allocation concealment and blinding of participants, personnel and outcome assessment, and other sources of bias (i.e., study underpowered or analysis did not account for clustering). Potential reporting bias was also identified across a number of outcome and comparison-based study groupings. Third, statistical heterogeneity was high for the outcome of BMI and BMI z-score, which could primarily be attributed to small versus large treatment effects observed across studies (Figure 3). Other possible factors for heterogeneity (e.g., intervention type, setting and duration, participants’ sex and age, and study risk of bias) were explored (see Table 2). Fourth, because we only looked at features of interventions that showed a significant benefit over the control condition, we cannot comment whether these characteristics differ in any way from interventions that failed to show a difference. Finally, a language filter was applied in our search because of limited resources available to appropriately handle (e.g., screening, translation and interpretation) publications in other languages; therefore, only publications in English or French were captured by our search.
Conclusion
Small improvements in weight outcomes with questionable clinical importance were found. The small magnitude of effect observed across studies suggests the need for trials with larger sample sizes that are powered to detect small differences across subgroups. Moreover, the paucity of studies involving very young children warrants further research in this context. Finally, the diversity of intervention strategies and unexplained heterogeneity limits the generalizability of the small effect found in our review for a mixed-weight population; future research involving normal-weight children is required.
Supplemental information
For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/lookup/suppl/doi/10.9778/cmajo.20140053/-/DCI

(See Figure 3B for part 2). Effect of prevention interventions on change in body mass index (BMI) and BMI z-score. Values less than 0 indicate a change in BMI in favour of the intervention. 1 = intervention arm 1; 2 = intervention arm 2; CI = confidence interval; F = female; M = male; SD = standard deviation; SMD = standardized mean difference; z = BMI z-score.
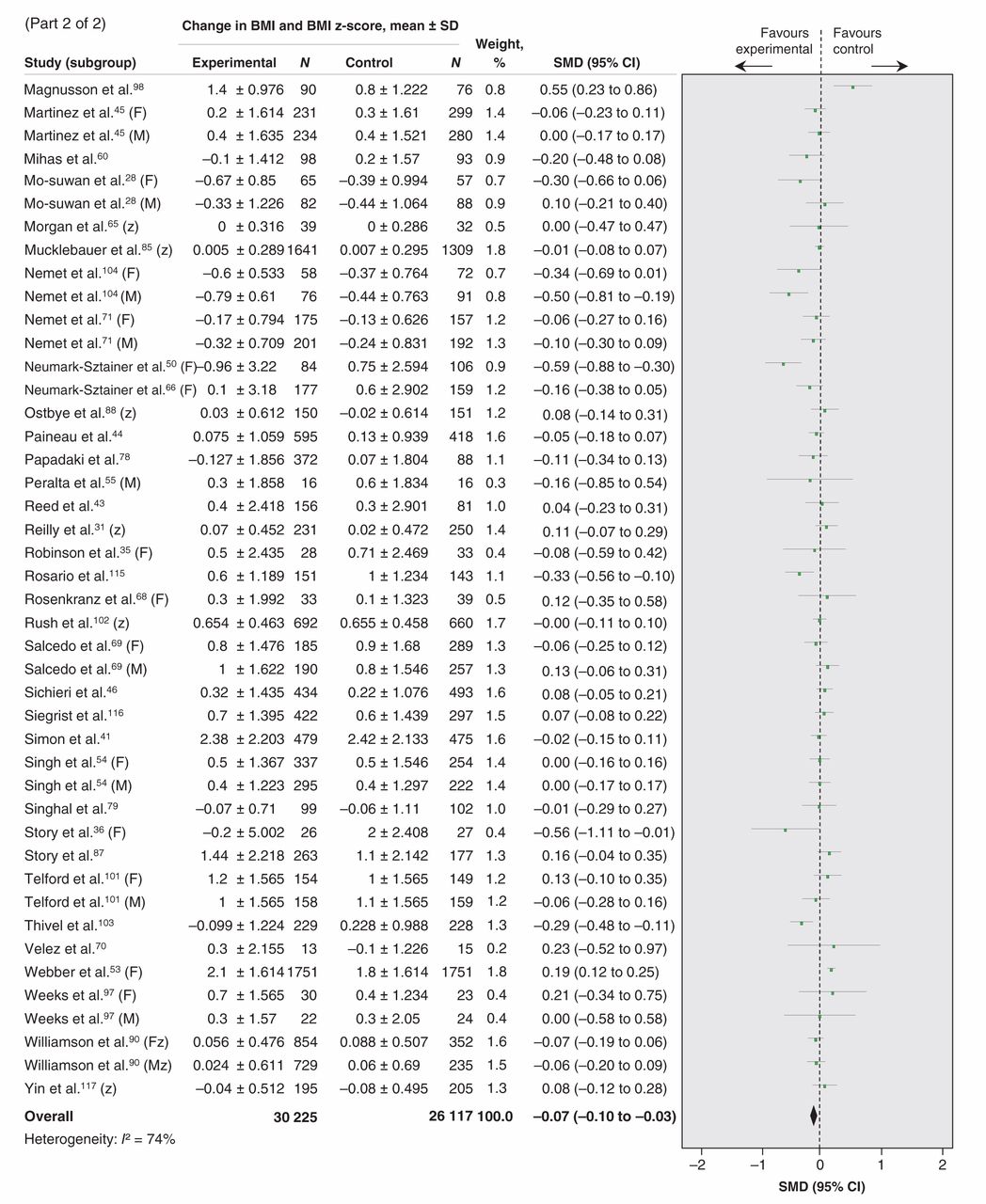
Effect of prevention interventions on change in body mass index (BMI) and BMI z-score. Values less than 0 indicate a change in BMI in favour of the intervention. 1 = intervention arm 1; 2 = intervention arm 2; CI = confidence interval; F = female; M = male; SD = standard deviation; SMD = standardized mean difference; z = BMI z-score.
Acknowledgements
Rachel Warren, Eva Tsakonas and Mary Gauld contributed to the relevance and quality assessment, and data-extraction phases. We are grateful to Maureen Rice for the search and to Sharon Peck-Reid for database management and formatting of the report. Sarah Connor Gorber and Amanda Shane (Scientific Officers, Public Health Agency of Canada) contributed to the original protocol development and review of drafts of the technical report. Similarly, Patricia Parkin, Maria Bacchus, Neil Bell, Paula Brauer and Elizabeth Shaw (members of the Child Obesity Working Group of the Canadian Task Force on Preventive Health Care) provided comments on the protocol and initial analyses.
Footnotes
-
Contributors: Leslea Peirson, Donna Fitzpatrick-Lewis, Katherine Morrison, Donna Ciliska, Meghan Kenny and Parminder Raina were involved in conceptualizing the study, data interpretation and writing and reviewing the manuscript. Leslea Peirson and Donna Fitzpatrick-Lewis were involved in developing the methods, collecting the data and coordinating the project. Muhammad Usman Ali conducted the data analyses and interpretation. All of the authors revised the manuscript, approved the final version submitted for publication and agreed to act as guarantors of the work.
-
Competing interests: Donna Ciliska and Parminder Raina have received grants from the Canadian Institutes of Health Research. No other competing interests were declared.
-
Funding: Funding was provided by the CIHR (www.cihr-irsc.gc.ca). The CIHR had no role in the study design, data analysis, interpretation or decision to submit the paper for publication. Parminder Raina holds a Tier 1 Canada Research Chair in Geroscience and the Raymond and Margaret Labarge Chair in Research and Knowledge Application for Optimal Aging.
-
Disclaimer: The views expressed herein are the opinions of the authors and do not necessarily represent the views of the CIHR or the Canadian Task Force on Preventive Health Care.
References
- © 2015, 8872147 Canada Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.