


Abstract
Background: Poor health of health care workers affects quality of care, but research and health data for health care workers are scarce. Our aim was to compare physical/mental health among health care worker groups 1) within nursing homes and pediatric hospitals, 2) between the 2 settings and 3) with the physical/mental health of the Canadian population.
Methods: Using cross-sectional data collected as part of the Translating Research in Elder Care program and the Translating Research on Pain in Children program, we examined the health of health care workers. In nursing homes, 169 registered nurses, 139 licensed practical nurses, 1506 care aides, 145 allied health care providers and 69 managers were surveyed. In pediatric hospitals, 63 physicians, 747 registered nurses, 155 allied health care providers, 49 nurse educators and 22 managers were surveyed. After standardization of the data for age and sex, we applied analyses of variance and general linear models, adjusted for multiple testing.
Results: Nursing home workers and registered nurses in pediatric hospitals had poorer mental health than the Canadian population. Scores were lowest for registered nurses in nursing homes (mean difference -4.4 [95% confidence interval -6.6 to -2.6]). Physicians in pediatric hospitals and allied health care providers in nursing homes had better physical health than the general population. We also found important differences in physical/mental health for care provider groups within and between care settings.
Interpretation: Mental health is especially poor among nursing home workers, who care for a highly vulnerable and medically complex population of older adults. Strategies including optimized work environments are needed to improve the physical and mental health of health care workers to ameliorate quality of patient care.
As the world's population grows and ages, pressures on physicians and other skilled health care workers increase. Care provided in hospitals and, increasingly, in nonacute settings such as nursing homes becomes more complex. This generates higher demands both for and on health care workers. Demands are costly on health care workers' well-being (e.g., burnout, stress, job dissatisfaction, injury, abuse) and increase the risk of physical and mental health problems.1-5 The resulting losses in workforce productivity (turnover, poor retention, absenteeism) represent substantial costs to the health care system.6-8 Simultaneously, good health of health care workers is linked to safe, high-quality patient care.9-13 Understanding and measuring the health of the health care workforce is an initial and necessary aspect of delivering optimal patient care.14
The health of Canadian physicians15,16 and nurses17 is well documented. Canadian physicians are healthier than the general Canadian population: more than 90% report good to excellent health.15 Still, mental health concerns are common among Canadian physicians, with almost 25% reporting a 2-week period of depressed mood, 20% reporting anhedonia, more than 25% stating that mental health concerns made it difficult to handle their workload, and nearly 25% reporting poor work-life balance.16 In nurses, pain is a common problem, with 37% reporting pain severity levels that prevented them from carrying out their normal activities of daily living.17 More female nurses than other female employees reported back problems (19% v. 25%), and more nurses (9%) experienced depression than did other employees (7% of women, 4% of men).17 There are few reports documenting the health of other Canadian health care workers (e.g., care aides, allied health care providers, nurse educators, managers), and comparisons of various health care worker groups (including physicians and nurses) within and across multiple care settings and with the general population are especially lacking.
Using representative data from 2 existing cohorts of Canadian health care workers (physicians, registered nurses, licensed practical nurses, care aides, allied health care providers, nurse educators and managers) from 2 different settings (nursing homes and pediatric hospitals), we aimed to compare the physical/mental health of health care worker groups 1) within each of the 2 settings, 2) between the 2 settings and 3) with that of the Canadian population. Our research questions were:
1. How does physical/mental health differ among various health care worker groups within nursing homes and pediatric hospitals?
2. How does the physical/mental health of health care workers of the same group differ between the 2 settings?
3. How does the physical/mental health of health care workers in the 2 settings differ from that of the Canadian population?
Methods
Design
This was a cross-sectional analysis of survey data collected from health care workers in nursing homes and pediatric hospitals. Nursing home data were collected in the Translating Research in Elder Care (TREC) program,18 a longitudinal pan-Canadian program (2007-2022) of applied health services research aiming to improve the quality of care and life of frail, older nursing home residents and the quality of work life for their paid care staff. Data used in this study were collected in the TREC program's second wave of surveys (July 2009-June 2010). Pediatric hospital data were collected in the Translating Research on Pain in Children (TROPIC) program (April 2006-March 2012), which aimed to promote the quality of life of infants and children by improving pain management in pediatric settings.19,20 Data used in this study were collected April-August 2011. Both research programs were funded by the Canadian Institutes of Health Research. We compared physical/mental health data collected in the TREC and TROPIC programs to Canadian normative 36-item Short Form Health Survey (SF-36) data.21
Settings and samples
Both the TREC program and the TROPIC program collected data from all major health care worker groups in their respective settings,18,20 which we used in this study.
The setting of the TREC program was a representative, randomly selected sample of 30 urban nursing homes in Canada, stratified by province (Alberta, Manitoba, Saskatchewan), size category (small [< 80 beds], medium [80-120 beds], large [> 120 beds]) and owner-operator model (public not-for-profit, voluntary not-for-profit, private for-profit).18 The overall survey response rate was 62%.
The setting of the TROPIC program was the 15 Canadian tertiary level pediatric hospitals (in British Columbia, Alberta, Manitoba, Ontario, Quebec and Nova Scotia) at the time of the study, 8 of which met the eligibility criterion of having at least 4 separate pediatric units. All 8 eligible facilities agreed to participate in the TROPIC program.19,20 The overall survey response rate was 44%.
Measurements and outcomes
All health care workers completed online surveys, except care aides, who completed computer-assisted structured personal interviews. We measured physical/mental health using the SF-8 Health Survey,22 a shortened version of the SF-36. The SF-36 is one of the most widely used health assessment tools21 and is rigorously designed and psychometrically robust.23-36 The SF-8 measures 8 health domains, each rated with the use of a 5- or 6-point Likert scale (Appendix 1, available at www.cmajopen.ca/content/5/4/E791/suppl/DC1).22 We scored the SF-8 using the proprietary algorithm obtained with the scale.22 We first assigned appropriate SF-36 scores, based on general US population data, to each corresponding SF-8 item response category (Appendix 1). We then generated 2 summary scores with a possible range of 0-100 (higher = better) for physical/mental health by assigning regression-based physical/mental weights to each SF-8 domain score and adding a physical or mental health intercept constant.22 These standard scoring methods were purposely designed by their developers to ensure that the SF-36 and SF-8 physical/mental component summary scores are comparable.22,37
Statistical analysis
We used SAS 9.4 (SAS Institute) for all statistical analyses. We calculated frequency counts and proportions for categorical data, and means and standard deviations for continuous data. To compare TREC, TROPIC and Canadian normative data, we standardized our SF-8 data for age and sex, using the same method (simple direct standardization) and population (Statistics Canada data from 199938) as a report on Canadian normative SF-36 data (which, to the best of our knowledge, are the only Canadian normative data available for an SF health survey).21 Specifically, we weighted total means based on underlying population characteristics. The Canadian normative SF-36 data were based on a prospective cohort study that included a random sample of 9423 Canadians aged 25 years or more living in the community.21 Normative data are essential to determining population average scores for countries or for age or sex groups, which we can validly compare our health care worker subgroups to. We calculated means, standard deviations, 95% confidence intervals (CIs) and floor/ceiling effects for each SF-8 health domain and calculated physical/mental component summary scores by health care worker group and health care setting. Floor and ceiling effects are defined as the proportion of participants selecting the response option reflecting the worst or best, respectively, possible health status. We compared age- and sex-adjusted SF-8 physical/mental component summary scores of all care provider groups in both settings with corresponding SF-36 scores for the Canadian population.21 We used analyses of variance, including pairwise post hoc comparisons adjusted for multiple testing (Dunnett method39-41). We compared age- and sex-adjusted SF-8 health domain scores and physical/mental component summary scores among health care workers within each health care setting. We used general linear models, adjusted for age, sex, education and job experience, and including pairwise post hoc comparisons adjusted for multiple testing (Tukey-Kramer method41-43). Using the same statistical method, we also compared SF-8 health domain scores and summary scores between the 2 settings for registered nurses, allied health care providers and managers. In all analyses, we deleted records with missing items listwise. Missing item rates were minimal (≤ 3% for all items except for sex of allied health care providers in nursing homes, which was missing in 7% of cases), and items were missing completely at random (Little missing completely at random test44 p = 0.4).
Ethics approval
We obtained ethics approval for the TREC program from the University of Alberta, University of Calgary, University of Saskatchewan and University of Manitoba. Operational approval was obtained from all relevant health care organizations. Ethics approval for the TROPIC program was obtained from the health research ethics boards of the appropriate Canadian universities and the participating hospital ethics boards (where applicable).
Results
Our sample included 3064 health care workers, 2028 (169 registered nurses, 139 licensed practical nurses, 1506 care aides, 145 allied health care providers and 69 managers) in nursing homes and 1036 (63 physicians, 747 registered nurses, 155 allied health care providers, 49 nurse educators and 22 managers on 32 independent hospital care units) in pediatric hospitals (Table 1). Registered nurses and allied health care providers in pediatric hospitals tended to be younger, better educated and more experienced than their counterparts in nursing homes. Women were overrepresented (81%-96%) in all provider groups except for physicians (52%).
Comparison of SF-8 health domain scores within and between the 2 settings
Table 2 shows the age- and sex-adjusted SF-8 subscores by care provider group and study setting. Floor effects were minimal (0 or almost 0) across SF-8 subscores and care provider groups, but ceiling effects varied substantially. Higher proportions of physicians and managers had maximum health domain scores. Registered nurses in nursing homes scored lower than those in pediatric hospitals on all but 2 of the adjusted health domain scores (Table 3). Allied health care providers in nursing homes scored higher than their counterparts in pediatric hospitals on 4 of the 8 domains. We found no significant differences in health domain scores for managers between the 2 settings.
Comparison of SF-8 summary scores between health care workers and the Canadian population
Compared to the Canadian population, physicians and allied health care providers in nursing homes had statistically significantly higher overall physical health scores, and care aides had lower overall physical health scores (Table 4). Except for managers, all nursing home provider groups had lower overall mental health scores than the Canadian population. The same was true for registered nurses in pediatric hospitals.
Comparison of SF-8 summary scores within and between the 2 settings
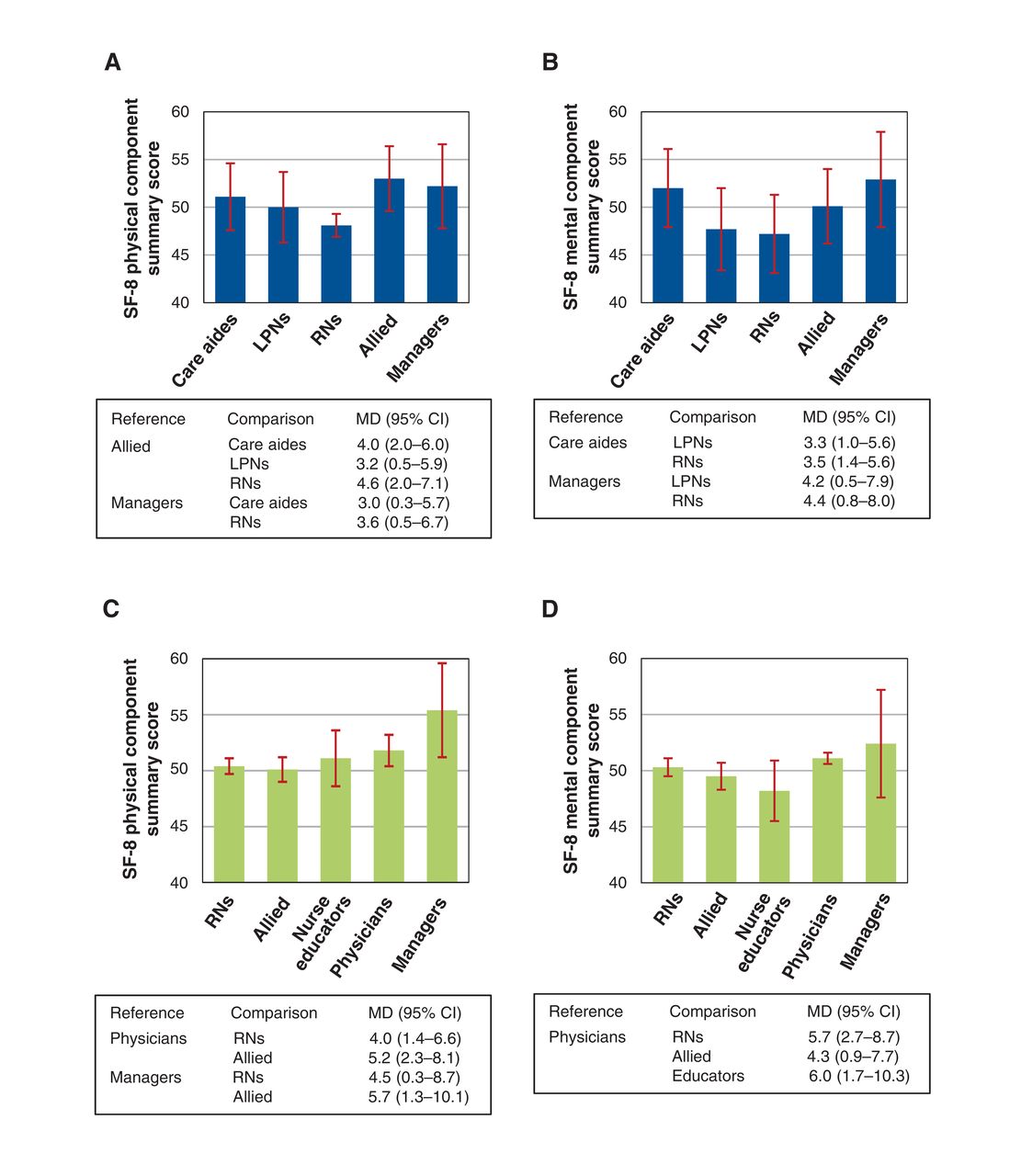
In nursing homes, allied health care providers had higher physical health scores than registered nurses (Figure 1, A). Mental health scores were higher for allied health care providers and managers than for nurses (Figure 1, B). In pediatric hospitals, physical and mental health summary scores did not differ significantly among health care provider groups (Figure 1, C and D).
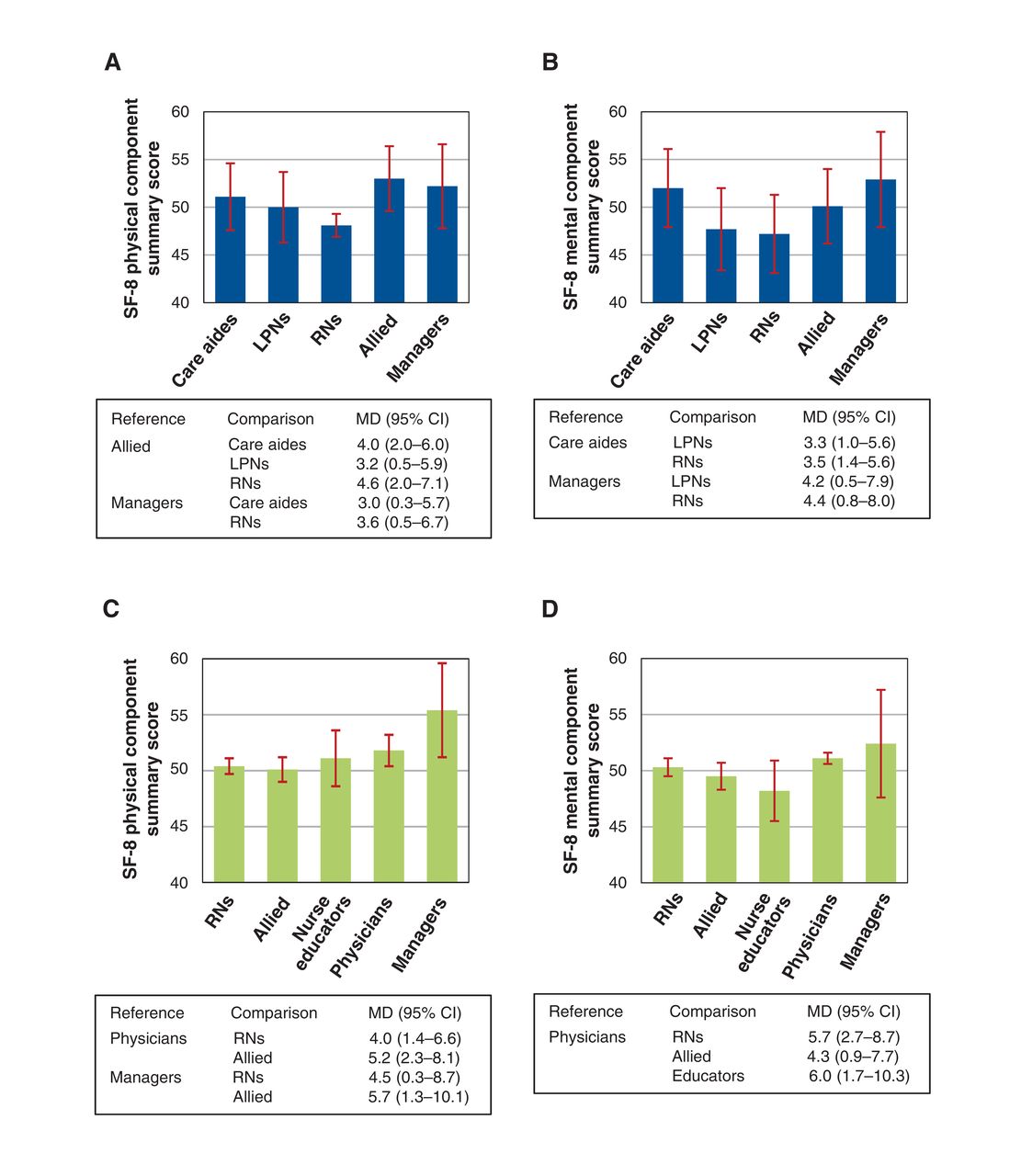
Physical health (A) and mental health (B) of selected health care workers in nursing homes, and physical health (C) and mental health (D) of selected health care workers in pediatric hospitals. Error bars represent 95% confidence intervals (CIs). Note: allied = allied health care providers, LPN = licensed practical nurses, MD = mean difference (mean for reference minus mean for comparison), RN = registered nurse, SF-8 = 8-item Short Form Health Survey.
Figure 2 illustrates health differences between nursing homes and pediatric hospitals. Physical and mental health scores were lower for registered nurses in nursing homes than for those in pediatric hospitals. Physical and mental health scores of the other health care worker groups did not differ significantly.

Physical health (A) and mental health (B) of registered nurses (RNs), allied health care providers (allied) and managers in nursing homes and pediatric hospitals. Error bars reflect 95% confidence intervals (CIs). Note: MD = mean difference (mean for nursing homes minus mean for pediatric hospitals), SF-8 = 8-item Short Form Health Survey.
Interpretation
In this study of normative SF-8 data for multiple health care worker groups in Canadian nursing homes and pediatric hospitals, physicians had better physical health than the Canadian population. Except for managers, all nursing home health care worker groups had lower mental health than the Canadian population. Within nursing homes, allied health care providers had better physical and mental health than registered nurses, and managers had better mental health than registered nurses. Registered nurses, especially those working in nursing homes, were at particularly high risk for poor health. Registered nurses in both settings had lower mental health than the Canadian population, and those working in nursing homes scored lower on 6 SF-8 subdomains and on the physical/mental health summary scores than those working in pediatric hospitals.
There is evidence that physicians have lower age- and sex-specific mortality rates and better health habits than respective groups in the general population.15,45,46 Although our findings support this, other studies suggest that rates of physical/mental health problems among physicians are as high as or higher than those among the general population.47,48 We found better (but not statistically significantly so) physical/mental health among physicians than among other health care workers, and international evidence suggests better health among physicians than among other health care workers.49-51 However, those studies did not differentiate among physician work settings.
Front-line staff are at particularly high risk for health problems; this is best documented among nurses.52,53 In the United States, 18% of nurses employed in hospital settings were found to have depressive disorders, compared to 9% of the general population.13 Nurses are at greater risk for musculoskeletal injuries and infections due to blood-borne pathogens than other health care workers and are at greater risk for breast cancer than other female health care workers.53 Nurses working in hospitals have a higher risk of tuberculosis than those working in other settings.53 In a cross-sectional survey of nearly 19 000 nurses across all types of settings in Canada, more female nurses than other employed women reported musculoskeletal conditions (34% v. 27%), migraine (18% v. 17%), cancer (1.8% v. 0.7%), stomach/intestinal ulcers (4% v. 3%), thyroid conditions (10% v. 8%) and medically unexplained physical symptoms (7% v. 5%).17 Both female and male nurses reported higher rates of asthma, bowel disorders, hypertension, cardiovascular and related conditions, 3 or more chronic conditions and depression.17 We found only 1 study comparing the health of registered nurses and managers in acute care settings: in a cross-sectional survey of 347 randomly selected employees from 7 hospitals within the major Athens area, managers' scores were 3-14 points higher than those of registered nurses on 6 of the 8 SF-36 health domains.50
Limitations
To compare our data to Canadian normative population-based data, we had to standardize our SF-8 data for age and sex to the same population (Statistics Canada, 199938) to which we compared our data.21 Our data were collected in 2009-2011, so the population data we used were outdated. Statistics Canada data indicate that the 2011 population38 was older than that in 1999 (31% v. 44% aged 45 yr), but otherwise the 2 populations were comparable. Using 2011 population data for standardization might have altered our results slightly but would have prevented comparison of our results with the only available normative SF health data for the Canadian population. Because our analyses were descriptive and our study was cross-sectional, our results show statistical associations but no causality. As some subsamples (physicians, educators, managers) were rather small, some of the nonsignificant findings may have been due to a lack of power. Future studies can use our reported effect sizes to determine adequate sample sizes for health care provider groups included in this study. Differences in health scores among health care worker groups in this study ranged between 1.9 and 5.6. For the SF surveys, minimum differences of 3-5 are generally considered clinically important.54-59 Although most of the differences identified in this study were within that range, some were below 3, which suggests limited clinical relevance. As the TREC and TROPIC data were collected at slightly different time points (about 1 yr apart), differences in health scores may have been influenced by different context conditions in the health care system. Finally, the SF-8 is a rather generic measure that does not allow differentiation between specific physical and mental health concerns. More specific measures are needed to guide interventions tailored to improve health care workers' health.
Conclusion
Health was especially poor among registered nurses in nursing homes, who care for a highly vulnerable and medically, functionally and socially complex population of older adults. The mental health of health care workers in nursing homes was notably worse than that of the general population, and registered nurses in nursing homes had worse physical and mental health than those in pediatric hospitals. Although most research focuses on patient health or the general population, we cannot neglect health care workers in highly complex and stressful environments. Their health affects quality of care. Health measures are largely influenced by individual characteristics, but features of work environments such as available resources, communication and leadership may also contribute. These work environment characteristics are modifiable and provide starting points for interventions to improve worker health and well-being.
Supplemental information
For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/5/4/E791/suppl/DC1.
Acknowledgements
The authors thank all care facilities and health care workers who participated in the Translating Research in Elder Care (TREC) and Translating Research on Pain in Children (TROPIC) programs for their contribution to this study. They also acknowledge all TREC and TROPIC team members who are not coauthors on this manuscript.
Footnotes
Competing interests: None declared.
Contributors: Carole Estabrooks, Peter Norton, Jennifer Knopp-Sihota and Matthias Hoben conceived the study. Matthias Hoben developed the analysis plan, carried out the statistical analyses and drafted the manuscript. Jennifer Knopp-Sihota, Maryam Nesari and Stephanie Chamberlain assisted with the statistical analyses and drafted sections of the manuscript. Carole Estabrooks is the principal investigator of the Translating Research in Elder Care (TREC) program, and Janet Squires, Peter Norton and Greta Cummings are coinvestigators with TREC and contributed to the collection of TREC survey data. Bonnie Stevens is the principal investigator of the Translating Research on Pain in Children (TROPIC) program, and Janet Squires, Greta Cummings and Carole Estabrooks are coinvestigators with TROPIC and contributed to the collection of TROPIC survey data. Matthias Hoben, Jennifer Knopp-Sihota, Stephanie Chamberlain, Peter Norton and Carole Estabrooks interpreted the data. All of the authors assisted with the development of the analysis, revised the manuscript for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: The Translating Research in Elder Care program was funded by Canadian Institutes of Health Research (CIHR) grant-in-aid MOP 53107. The Translating Research on Pain in Children program was funded by CIHR operating grant CTP-79854. The funding agency had no role in the study design, data collection, data analysis, data interpretation, writing of the report or decision to submit the article for publication.
References
- Copyright 2017, Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
Article tools


