


Abstract
Background: The Canadian National Advisory Committee on Immunization recommends universal vaccination against pertussis in pregnancy. We assessed the cost-effectiveness of vaccination with tetanus–diphtheria–acellular pertussis (Tdap) vaccine in pregnancy in Canada.
Methods: We conducted a cost-utility analysis comparing a vaccination program to no program corresponding with the 2017 Canadian guideline for economic evaluation from the Canadian Agency for Drugs and Technologies in Health. We developed 2 models — part decision tree, part Markov model — to estimate the long-term cost and quality-adjusted life-years (QALYs) for pregnant women and their infants. We obtained epidemiologic data from 2006 to 2015, and derived costs and utility values from relevant sources. Results were reported in 2019 Canadian dollars. We obtained expected values through probabilistic analysis, with methodologic and structural uncertainty assessed through scenario analyses. The analysis adopted an acquisition price of Tdap vaccine of $12.50, with scenario analysis conducted to identify the threshold price for vaccination to be cost-effective.
Results: In the base-case scenario, for every 1000 pregnant women vaccinated, the program would lead to a gain of 0.3 QALYs, occurring solely in infants, at an increased total cost of $12 987, or $44 301 per QALY gained. Based on a threshold of $50 000 per QALY gained, vaccination would have been cost-effective in 6 of the 10 years included in the model (range of incremental costs $20 463–$100 348 per QALY gained). The threshold cost for Tdap vaccine to be cost-effective over the 10-year horizon was $14.03.
Interpretation: Based on a threshold of $50 000 per QALY gained, vaccination against pertussis in pregnancy would be cost-effective if the acquisition cost per vaccine were $14.03 or less. Province- and territory-specific analyses should be done to inform local decision-making.
Pertussis is an endemic respiratory disease caused by the bacterium Bordetella pertussis. Globally, there are about 24 million cases and 160 000 deaths from pertussis in children less than 5 years of age every year.1 Canada introduced whole-cell pertussis vaccine into the routine vaccination schedule in 1943 and replaced it with acellular pertussis vaccine, which has a better safety profile, in 1997–1998. In Canada, pertussis vaccines are given to all children at ages 2, 4, 6 and 18 months, 4–6 years and 10–15 years (Quebec: 2, 4 and 12 mo, and 4–6 yr) (Appendix 1, Supplemental Table S1, available at www.cmajopen.ca/content/8/4/E651/suppl/DC1).2
During 2012–2015, pertussis incidence increased markedly in Canada, to 3.6–13.4/100 000 per year,3 and frequent outbreaks continue to occur globally.4–10 Young infants have the highest burden of pertussis in Canada.11 During 1999–2015, 76% of 1402 children admitted to hospital with pertussis were infants aged 3 months or less. Infants aged less than 2 months had the highest annual incidence of hospital admission and intensive care unit admission (116 and 33 per 100 000, respectively). As current infant vaccination programs starting at age 2 months cannot protect these youngest, most vulnerable infants, pertussis vaccination during each pregnancy is recommended in Canada, as well as in other countries.12,13
In February 2018, the Canadian National Advisory Committee on Immunization recommended that all pregnant women receive pertussis vaccine (in the form of tetanus–diphtheria–acellular pertussis [Tdap] vaccine) in every pregnancy, ideally at 27–32 weeks’ gestation.12 Vaccination against pertussis in pregnancy has proved to be highly (nearly 90%) effective in preventing pertussis disease in infants aged less than 3 months in the United Kingdom and United States,14–16 and in decreasing the risk of hospital admission, intensive care unit admission and hospital length of stay.17
Assuming that vaccination against pertussis in pregnancy is 90% effective in preventing hospital admission for pertussis among infants aged less than 3 months, admission of about 825 infants with pertussis to tertiary care centres in Canada could have been prevented via maternal vaccination during 1999–2015. However, the cost-effectiveness of this strategy is an important consideration. The objective of the present study was to assess the cost-effectiveness of vaccination in pregnancy with Tdap vaccine in Canada.
Methods
Design
The decision problem or research question was whether vaccination against pertussis in pregnancy should be funded by the relevant public health care payer. To answer this question, we conducted a cost-utility analysis that compared pertussis vaccination to no vaccination. The analysis was conducted over a lifetime horizon from a health care payer perspective (incorporating the lifetime costs and effects of the vaccination and subsequent events). Our analysis corresponded with the 2017 Canadian guidelines for economic evaluation from the Canadian Agency for Drugs and Technologies in Health.18
Model structure
We developed a de novo model that included decision tree and Markov model elements to estimate the long-term cost and quality-adjusted life-years (QALYs) associated with vaccination versus no vaccination for both infants and pregnant women (Figure 1; Appendix 2, available at www.cmajopen.ca/content/8/4/E651/suppl/DC1).19 For infants, the short-term decision tree estimated the following outcomes: proportion who, by 12 months of age, would have had no pertussis, mild pertussis (no hospital admission) or pertussis requiring hospital admission (with and without encephalitis and chronic encephalitis), or would have died. For pregnant women, a decision tree estimated the following outcomes: proportion with no pertussis, mild pertussis, severe pertussis (cough illness with apnea, cyanosis, vomiting or urinary incontinence), pneumonia without hospital admission or pneumonia with hospital admission, or who died. For both infants and women, for each of the outcomes, we created a Markov model with a 1-year cycle and a lifetime horizon (up to age 110) with the states of alive and dead.

Markov models to estimate the long-term cost and quality-adjusted life-years associated with vaccination with tetanus–diphtheria–acellular pertussis vaccine v. no vaccination in pregnancy. (A) Infants. (B) Women.
Model parameter values
To select the parameters used in our model, we conducted a targeted search of the English-language literature on costs and utilities to identify the most pertinent recent data applicable to the Canadian context (Appendix 1, Supplemental Table S2; Appendix 2). Data required to facilitate estimation of transition probabilities included the probability of pertussis in infants and adults, the severity of pertussis cases and the duration of symptoms, the effectiveness of vaccination, and the incidence of vaccination-related adverse events and their duration. We divided adverse events following vaccination into local (defined as a sore upper arm that is slightly red, swollen and tender) and systemic (defined as a low-grade fever, headache, body ache and decreased energy).
In addition, costs and utility values for each potential outcome were required. We obtained these from the literature through a detailed targeted review and selected them based on their fitness for purpose (i.e., relevance to the decision problem), credibility and consistency. We assessed fitness for purpose based on the contemporaneous nature of the data and the relevance to the specific outcomes. We assessed credibility based on the appropriateness of the methodology adopted to derive the data estimates, and assessed consistency by adopting parameter values from the literature using similar methods and approaches.
As pertussis is a cyclical disease, with peaks occurring every 3–4 years asynchronously across Canada,20 we used epidemiologic data relating to infant infection for 2006–2015.21
Base case
The model estimated 71 cases of pertussis disease per 100 000 among all infants less than 1 year of age, with 68% of cases in those aged less than 2 months and 18% in those aged 2–4 months.21 This would translate to about 284 cases per year among all infants aged less than 1 year (assuming an annual birth cohort of 400 00022), including 192 cases in those aged less than 2 months and 52 cases in those 2–4 months of age. High rates of hospital admission occur in this age group (estimated at 87% for infants < 2 mo of age and 84% for those aged 2–4 mo).6 It was estimated that, among all infants less than 12 months of age admitted to hospital, death would occur in 0.8% and encephalitis in 0.5%, with chronic encephalitis developing in 33% of those with acute encephalitis.2,23
The model estimated 0.6 cases per 100 000 pregnant women per year, with pneumonia requiring hospital admission occurring in 1 in every 10 million. Overall, 31% of cases in pregnant women were assumed to be mild and 67% severe, with severity unknown in 2%.24
Symptom duration was estimated at 93 days for pregnant women and 75 days for infants.25
Based on a cohort study by Amirthalingam and colleagues26 with a sample size of 72 781, the model estimated overall vaccine effectiveness (in infants and pregnant women) to be 91% (95% confidence interval [CI] 0.88–0.94) against pertussis and 95% (95% CI 0.79–1.00) against death from pertussis. A recent systematic review27 showed that vaccination effectiveness in preventing pertussis in infants of vaccinated women ranged from 69% in a small (n = 96) case–control study28 to 91% in 3 other studies.16,26,29 The authors of the systematic review found only 1 study with an estimate of vaccination effectiveness in reducing deaths from pertussis.26
The model estimated local adverse events following vaccination to occur at a prevalence of 15% and a time to full recovery of 7 days.30,31 Systemic reactions were estimated to occur in 6% of cases, with a time to full recovery of 7 days.30,31 Anaphylaxis was estimated to occur once per 200 000 doses, with a time to full recovery of 2 days.31,32
Statistical analysis
Long-term outcomes were discounted at a rate of 1.5% per annum, with costs expressed in 2019 Canadian dollars. In the base-case scenario, we obtained expected values of costs and QALYs through probabilistic analysis. We obtained values for all uncertain data through random sampling from their probability distributions and, for the epidemiologic data, the year from which the data were taken, also drawn randomly.
We assessed methodologic and structural uncertainty through scenario analyses. We conducted analyses using epidemiologic data specific to each year. In addition, we conducted analysis using different discount rates (0% and 3%), as well as a time horizon of 50 years for estimating long-term costs and QALYs.
As the acquisition cost of Tdap vaccine in this context is confidential and thus was uncertain, analysis adopted a price of $12.50 (plus $4.50 in administration costs) for illustrative purposes, with scenario analysis conducted to identify the threshold price for vaccination to be cost-effective. Because vaccination would be given at routine care, the model assumed no additional program costs.
Ethics approval
Ethics approval was not required because of the study type.
Results
In the base-case scenario, with epidemiologic data across the period from 2006 to 2015, the Tdap vaccination program would cost an additional $17 000 per 1000 pregnant women vaccinated ($17 per woman) but would reduce the costs of treatment for pertussis per 1000 pregnant women vaccinated, for both infants (by $12 987) and women (by $1.00). The program would lead to a gain of 0.3 QALYs per 1000 pregnant women vaccinated, occurring solely in infants. This would lead to an incremental cost per QALY gained of $44 301 (Table 1).
Cost-effectiveness per 1000 pregnant women of vaccination in pregnancy with tetanus–diphtheria–acellular pertussis vaccine
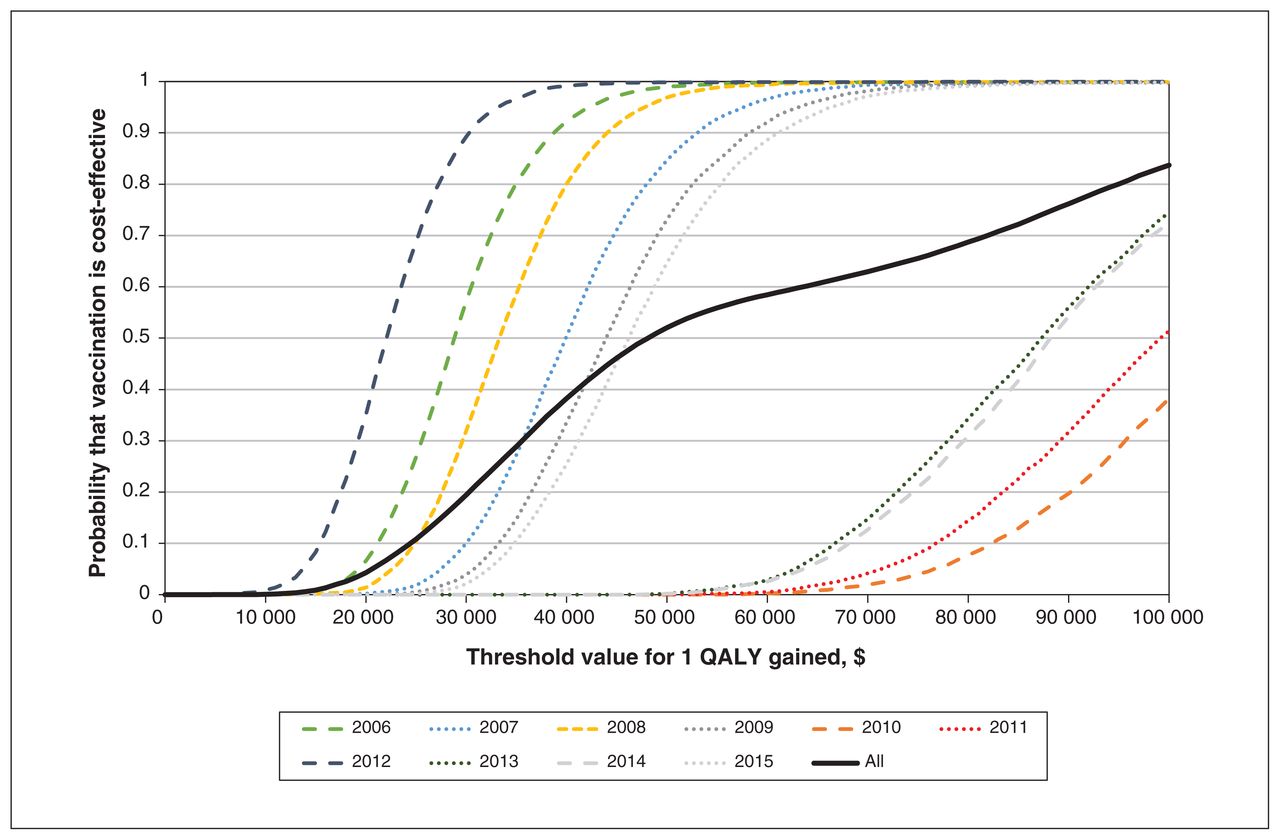
At a threshold of $50 000 per QALY gained, the probability that vaccination would be cost-effective is 52% (Figure 2). At a threshold of $100 000 per QALY gained, the probability that it would be cost-effective is 84%. If the acquisition cost of Tdap vaccine were $14.03, the incremental cost per QALY gained from vaccination would be $50 000 (Figure 3). Thus, if the willingness to pay per QALY gained were $50 000 and the cost of Tdap vaccine were no more than $14.03, vaccination would be cost-effective.

Cost-effectiveness acceptability curve for pertussis vaccination during pregnancy in Canada. Costs are presented in 2019 Canadian dollars. Note: QALY = quality-adjusted life-year.

Estimated incremental cost per quality-adjusted life-year (QALY) gained by acquisition cost of pertussis vaccine. Costs are presented in 2019 Canadian dollars.
Scenario analyses
Analysis by each year of epidemiologic data showed that the estimates are highly dependent on annual disease burden, which fluctuates owing to the natural cycling of disease (Table 2). Based on a threshold of $50 000 per QALY gained, vaccination would have been cost-effective in 6 of the 10 years included in the model (range $20 463 in the year with the highest disease burden to $100 348 in the year with the lowest disease burden). The probability that vaccination would be cost-effective (assuming a threshold of $50 000 per QALY gained) ranged from a high of greater than 99% to a low of less than 1% (Figure 3).
Scenario analyses relating to year of epidemiologic data, discount rate, time horizon and source of vaccine effectiveness
Because vaccination during pregnancy is expected to be implemented more widely in the future, we applied a discount rate, which resulted in incremental costs of $29 365 for a rate of 0% to $75 872 for a rate of 5% (Table 2). Adopting a reduced time horizon of 50 years for estimating long-term costs and QALYs led to an increase in the incremental cost per QALY to $54 398.
We performed a scenario analysis using the lower estimate of vaccination effectiveness (69% reduction in pertussis cases), from the case–control study,28 and found that vaccination would not be cost-effective under this scenario (incremental cost $55 031) (Table 2).
Interpretation
Our cost-effectiveness analysis showed that vaccination in pregnancy with Tdap vaccine would be cost-effective in Canada if the acquisition cost of the vaccine alone were no more than $14.03 per dose at a threshold of $50 000 per QALY gained. This is based on national data and disease burden estimates over a 10-year period that account for the natural annual fluctuation in pertussis incidence. Our analysis highlights that cost-effectiveness is somewhat dependent on annual disease incidence, with the threshold of $50 000 per QALY gained being reached in 6 of the 10 years. This cost-effectiveness modelling is comprehensive, as it considered the age-specific burden of disease, temporal changes in disease incidence, severe outcomes, vaccine effectiveness, adverse events following vaccination, and costs of both the vaccine program and health care treatment related to pertussis.
Our results are similar to those found in the US, Brazil and the Netherlands, although any comparisons with other settings should be interpreted with caution, as results of cost-effectiveness analyses are highly context dependent.33–35 Based on our base-case scenario, vaccination with Tdap in pregnancy in Canada would lead to an incremental cost of $44 301 per QALY gained and would have been cost-effective in 6 of the 10 years studied. Similarly, the incidence of pertussis influenced cost-effectiveness estimates in England, where the strategy of pertussis vaccination in pregnancy was estimated to achieve an incremental cost of £16 856–£42 070 per QALY gained.36 The highest gain was predicted to be achieved at £16 856 in the year with the highest incidence.
The results of cost-effectiveness analyses are affected by the cost per vaccination, which directly affects costs per QALY gained. Lower-cost pertussis vaccines may be cost-effective even in years with lower rates of pertussis incidence if they can display similar efficacy. In our study, the vaccination cost was $17, which gave an incremental cost of $44 301 per QALY gained. In a US study with a high vaccine cost (US$57.60), the incremental cost per QALY gained was much higher, US$414 523.37 Other investigators have estimated the cost of vaccine to be in the range of US$14.6–US$57.60 (Can$19.60–$77.20),33–39 with cost-effectiveness ranging depending on disease incidence.
Because pertussis vaccination is recommended during each pregnancy,12,13 our cost-effectiveness analysis would still be valid for subsequent pregnancies. If this recommendation changes in the future, the cost-effectiveness analysis should be modified accordingly. If modulation of infants’ immune responses is found to be clinically significant, this effect should be modelled in future cost-effectiveness analyses, as it may decrease the cost-effectiveness of a maternal vaccination strategy if additional infant booster doses are required. Finally, our cost-effectiveness analysis is based on data published between 2006 and 2015; thus, this analysis should be updated as more data are collected and published.
Limitations
Our study has several limitations. Our search for model parameters was limited to the English-language literature; thus, our results should be interpreted with caution in provinces and territories where data are published in languages other than English.
Although the costs and benefits to pregnant women arising from a vaccination program for the prevention of pertussis in the initial year were included, direct protection of the woman against pertussis disease may last for several years, and this might affect the cost-effectiveness of the program. Mothers play a central role in transmission of pertussis to infants and other household members.40 Thus, vaccination might prevent transmission within household contacts for several years after vaccination in pregnancy and potentially increase the cost-effectiveness of this strategy.
Underreporting of pertussis cases may have affected the estimation of the true incidence and burden of pertussis disease, especially in older adults, and thus our model may have underestimated the cost-effectiveness of a program of vaccination during pregnancy. However, the effect of this underreporting is expected to be minimal, as pertussis in early infancy leads to severe disease that is recognized and reported in young infants, who are the primary target of protection following Tdap vaccination during pregnancy.
Our paper focuses on the effect of pertussis vaccination during pregnancy on the burden of pertussis disease in infants. Although the vaccine contains diphtheria and tetanus components, vaccination during pregnancy is not expected to have substantial beneficial or detrimental effects against tetanus and diphtheria diseases owing to the extremely low rates of disease in infants in Canada. In addition, higher antibody levels transferred to the infant after maternal Tdap vaccination may inhibit the infant’s response to subsequent vaccination to pertussis vaccines and other vaccines.41 Our model did not take into account the potential effect of this modulation of the infant’s immune response, as its clinical significance is unclear.
Our model assumed that the average program costs would be $2.50. Higher costs would have the incremental effect of reducing the threshold for the cost of the vaccine to be considered cost-effective. In addition, given that the acquisition cost of the vaccine is regarded as confidential information and is not publicly available in Canada, we adopted a price of $12.50, plus $4.50 in administrative costs. This value is similar to that used in published cost-effectiveness analyses from other countries.36,39 Other associated costs were not included.
We recognize that, within Canada, the decision as to whether and how to implement a vaccination program is made at the provincial and territorial level, and such provincial-and territorial-specific analyses should be done to inform local decision-making.
Conclusion
Based on a threshold of $50 000 per QALY gained, pertussis vaccination in pregnancy would be cost-effective if the acquisition cost per vaccine were $14.03 or less. However, the applicability of our results for current and future policy decisions depends on the incidence of pertussis disease, especially among infants less than 3 months of age, which is difficult to predict and can be province-specific.
Acknowledgements
The authors gratefully acknowledge the expert assistance provided by the Canadian Immunization Monitoring Program, ACTive (IMPACT) Monitor Liaisons Heather Samson and Annick Audet, IMPACT Surveillance Manager Melanie Laffin, and the IMPACT nurse monitors and staff of the IMPACT data centre (Kim Marty, Shuzhen Liu and Jennifer Mark).
Footnotes
↵* Canadian Immunization Monitoring Program, ACTive (IMPACT): IMPACT is a national surveillance initiative managed by the Canadian Paediatric Society and conducted by the IMPACT network of pediatric investigators. Members: C. Foo and N. Bridger, Eastern Health Janeway Children’s Health and Rehabilitation Centre, St. John’s, NL; K. Top and S. Halperin, IWK Health Centre, Halifax, NS; R. Thibeault, Centre Mère-Enfant Soleil, Québec, Que.; J. Papenburg and D. Moore, Montreal Children’s Hospital of the McGill University Health Centre, Montréal, Que.; M. Lebel, CHU Sainte-Justine, Montréal, Que.; N. Le Saux, Children’s Hospital of Eastern Ontario, Ottawa, Ont.; D. Tran and S. Morris, The Hospital for Sick Children, Toronto, Ont.; J. Embree, Winnipeg Children’s Hospital, Winnipeg, Man.; B. Tan, Royal University Hospital, Saskatoon, Sask.; T. Jadavji, C. Constantinescu, O. Vanderkooi and J. Kellner, Alberta Children’s Hospital, Calgary, Alta.; W. Vaudry and C. Burton, Stollery Children’s Hospital, Edmonton, Alta.; D. Scheifele, J. Bettinger, M. Sadarangani and L. Sauvé, BC Children’s Hospital, Vancouver, BC
Competing interests: Manish Sadarangani is supported via salary awards from the BC Children’s Hospital Foundation, the Canadian Child Health Clinician Scientist Program and the Michael Smith Foundation for Health Research. He has been an investigator on projects funded by Merck, VBI Vaccines, Pfizer, Seqirus, Sanofi Pasteur and GlaxoSmithKline; all funds have been paid to his institute, and he has not received any personal payments. Scott Halperin has been an investigator on projects funded by Merck, VBI Vaccines, Pfizer, Seqirus, Sanofi Pasteur and GlaxoSmithKline, and has served on ad hoc advisory boards for Merck, Sanofi Pasteur, GlaxoSmithKline and Pfizer; all funds have been paid to his university, and he has not received any personal payments. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Manish Sadarangani and Doug Coyle obtained the data. Doug Coyle analyzed the data. Bahaa Abu-Raya and Manish Sadarangani drafted the manuscript. All of the authors conceived and designed the study, interpreted the data, revised the manuscript critically for important intellectual content, approved the final version to be published and agreed to be accountable for all aspects of the work.
Funding: Bahaa Abu-Raya is supported by a Canadian Institutes of Health Research Vanier Canada Graduate Scholarship.
Data sharing: Our analysis used published and available data (detailed in the accompanying appendix).
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/8/4/E651/suppl/DC1.
References
- Copyright 2020, Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools





