


Abstract
Background: Indigenous people are disproportionately affected by mental health issues in Canada. We investigated factors underlying the difference in psychological distress and suicidal behaviours between non-Indigenous and Indigenous populations living off-reserve in Canada.
Methods: We conducted a cross-sectional study using data from the 2012 Canadian Community Health Survey — Mental Health. Respondents were aged 18 years and older. We measured the variation in psychological distress (10-item Kessler Psychological Distress Scale scores, ranging from 10 [no distress] to 50 [severe distress]) and the prevalence of lifetime suicidal ideation and suicide plan between the Indigenous and non-Indigenous populations and explained these differences using the Blinder–Oaxaca approach.
Results: The overall response rate for the survey was 68.9%, comprising 18 300 respondents (933 Indigenous and 17 367 non-Indigenous adults). We found lower mean psychological distress scores among non-Indigenous people than among Indigenous people (15.1 v. 16.1, p < 0.001) and a lower prevalence of lifetime suicidal ideation (9.2% v. 16.8%, p < 0.001) and plan (2.3% v. 6.8%, p < 0.001). We found that if socioeconomic status among Indigenous people were made to be similar to that of the non-Indigenous population, the differences in mean psychological distress scores and prevalence of lifetime suicidal ideation and suicide plan would have been reduced by 25.7% (women 20.8%, men 36.9%), 10.2% (women 11.2%, men 11.9%) and 5.8% (women 7.8%, men 8.1%), respectively.
Interpretation: Socioeconomic factors account for a considerable proportion of the variation in mental health outcomes between non-Indigenous and Indigenous populations in Canada. Improving socioeconomic status among Indigenous people through plans like income equalization may reduce the gap in mental health outcomes between the 2 populations in Canada.
Indigenous people around the globe have suffered from the impacts of colonization to various extents and often share similar historical and ongoing collective adversities that negatively affect well-being.1,2 Of particular concern is the disproportionate burden of mental health issues among Indigenous people.3–5 A growing number of studies demonstrate the extent of inequality in physical health and mental health between non-Indigenous and Indigenous populations. 6–10 For example, just under one-quarter of Inuit (23.5%) and First Nations adults living off-reserve (24.0%) and 1 in 5 Métis (19.6%) reported lifetime suicidal ideation, compared with just over 1 in 10 non-Indigenous adults.11 Furthermore, a recent study12 shows inequalities in mental health outcomes within Indigenous populations in Canada.
To assist effective policy-making based on the emerging evidence of the extent of inequalities, it is critical to understand what explains these inequalities. Recent studies12,13 highlighted the importance of social determinants of health in inequalities in health and mental health outcomes within Indigenous populations in Canada. These studies show, for example, that policies designed to address food insecurity may help reduce mental health issues among Indigenous people living off-reserve in Canada. Our study objective was to quantify the extent of, and explain various demographic, socioeconomic and geographical factors that account for, inequalities in psychological distress, suicidal ideation and suicide plans between non-Indigenous and Indigenous populations living off-reserve in Canada.
Methods
Data source, design and study population
This is a cross-sectional analysis using the most recent Canadian Community Health Survey–Mental Health (2012 CCHS–MH).15 This survey was designed to collect information on mental health and health care services, lifestyle and social conditions, and prevention and detection of disease from both non-Indigenous and Indigenous populations living off-reserve (79.7% of the total Indigenous population14) in Canada.
The survey is a large nationally representative survey of individuals aged 15 years and older living in the 10 provinces in Canada, except those living on reserves and other Indigenous settlements, full-time members of the Canadian Armed Forces and the population living in institutions. These exclusions represent approximately 3% of the Canadian population aged 15 years and older. We restricted the study sample to nonimmigrant respondents aged 18 years and older.
Data were collected by trained interviewers using computer assisted personal interviewing and telephone interviewing. The majority of interviews (87%) were conducted in person. The questionnaire collected information on a range of topics such as demographics, socioeconomic status, medical conditions, well-being and functioning, and mental health status. Further information about questionnaire and sampling methods can be found elsewhere.15
Variables
The outcome variables included psychological distress, lifetime suicidal ideation and lifetime suicide plan. The 10-item Kessler Psychological Distress Scale (K10; Appendix 1, available at www.cmajopen.ca/content/9/1/E215/suppl/DC1)16 was used to identify psychological distress of individuals. The K10 comprises items evaluating psychological and physiologic symptoms of depression and anxiety. The overall K10 scores range from 10 (no distress) to 50 (severe distress). The K10 is shown to be appropriate and valid for use in Indigenous populations living on- and off-reserve in Canada.16–19 Based on the information available in the CCHS–MH, we constructed 2 binary variables (yes or no) assessing lifetime suicidal ideation and suicide plan. Indigenous populations in this study refers to Inuit, Métis and First Nations people living off-reserve in Canada.
As per the existing literature12,13,20–28 and availability of questions assessed in the CCHS–MH, we considered a variety of demographic variables (sex, age and marital status), socioeconomic variables (equivalized household income, education, employment status, household arrangement and homeownership status) and geographic variables (urbanicity and region) known to be associated with mental health outcomes. We equivalized annual household income by dividing it by the square root of household size.29 Appendix 2 (available at www.cmajopen.ca/content/9/1/E215/suppl/DC1) presents the definitions and descriptive statistics of all the variables used in the study.
Statistical analysis
We first performed the ordinary least squares and logistic regressions to investigate the effect of determinants on the continuous psychological distress and 2 binary suicidal behaviours, respectively. Subsequently, we used the Blinder–Oaxaca decomposition method30,31 to understand the contribution of each factor to the overall differences in the 3 mental health outcomes between non-Indigenous and Indigenous populations.
The Blinder–Oaxaca technique enabled us to decompose the observed gaps between the 2 populations into explained and unexplained components. The explained (endowment) component captures the part of the difference in a given outcome explained by differences between groups in the level of observed characteristics that were assessed (i.e., demographic, socioeconomic and geographic variables). The unexplained component captures the portion attributable to differences in the effects of these characteristics and unobserved determinants on the outcome of interest in non-Indigenous and Indigenous populations. The absolute value of the explained component for income factor, for example, can determine how much the gap in the mean of psychological distress levels between non-Indigenous and Indigenous populations would have been reduced if the income of Indigenous people were set to be at the similar level of non-Indigenous Canadians, all other things being equal.30–32
We used the Blinder–Oaxaca decomposition for a linear model to assess the differences in the mean scores of psychological distress. An extended version of the Blinder–Oaxaca technique for a logistic model32 was used to evaluate the difference in the prevalence of suicidal ideation and suicide plans. Appendix 3 (available at www.cmajopen.ca/content/9/1/E215/suppl/DC1) provides a detailed description of our regression and decomposition analyses.
To acknowledge potential differential results by sex, we stratified all analyses by sex. The t test and χ2 statistics were used to test the differences in continuous (i.e., psychological distress) and categorical (i.e., lifetime suicidal ideation and lifetime suicide plan) variables between non-Indigenous and Indigenous populations, respectively. We considered p < 0.05 as statistically significant. As per Statistics Canada’s Research Data Centre guidelines, all analyses were weighted to represent all adults living off-reserve in Canada. Observations with missing information on any of the variables were excluded from the analyses. We performed all the analyses in Stata 14.
Ethics approval
We accessed the 2012 CCHS–MH through Statistics Canada’s Atlantic Research Data Centre. Data accessed through the Research Data Centres, which follow strict disclosure protocols according to the Statistics Act, are exempt from research ethics board review based on the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans — TCPS2 article 2.2 (a).
Results
Sample characteristics
The CCHS–MH contains information on 25 113 participants. The response rate of the survey was 68.9%. After we excluded 4166 immigrant individuals, 1156 individuals aged 15–17 years and 1491 individuals with missing values in outcomes or explanatory variables, our final sample consisted of 18 300 adults. There were 933 Indigenous (55.1% women) and 17 367 non-Indigenous (54.9% women) individuals, representing 18 573 280 (754 982 Indigenous and 17 818 298 non-Indigenous) individuals in Canada.
The mean scores of psychological distress were lower among non-Indigenous than Indigenous populations (total: 15.05 v. 16.05, p < 0.001; women: 15.32 v. 16.53, p = 0.007; men: 14.78 v. 15.59, p = 0.03) respectively. The prevalence of lifetime suicidal ideation (total: 9.20% v. 16.80%, p < 0.001; women: 9.69% v. 19.10%, p < 0.001; men: 8.70% v. 14.60%, p = 0.005) and lifetime suicide plan (total: 2.23% v. 6.81%, p < 0.001; women: 2.66% v. 7.73%, p = 0.008; men: 1.98% v. 5.94%, p = 0.006) was lower among non-Indigenous than Indigenous populations, respectively (Table 1).
Summary statistics of variables used in the study
The non-Indigenous population in Canada was older than the Indigenous population. Equivalized household annual income of the non-Indigenous population (total: $54 426; women: $52 076; men: $56 846) was higher than that of the Indigenous population (total: $46 550; women: $44 482; men: $48 488). The non-Indigenous population had higher educational attainment than the Indigenous population. While 61.9% (women 55.9%; men 68.2%) of the non-Indigenous population was employed in Canada, employment was 57.6% (women 56.1%; men 58.9%) in the Indigenous population. The proportion of home ownership was higher in the non-Indigenous than in the Indigenous population in Canada (Table 1).
Determinants of psychological distress and suicidal behaviours
There were negative associations between age and mental health outcomes among both women and men. A 1-year increase in age was associated with a decrease of 0.054 (women 0.068, men 0.043) points in distress score and 0.11 (women 0.12, men 0.09) percentage points in the probability of having lifetime suicidal ideation. The probability of lifetime suicide plan also decreased by age among men.
Income was negatively associated with all the 3 mental health outcomes among women and men. Psychological distress among employed individuals was lower compared with those unemployed and those with other employment status. Home ownership was associated negatively with distress levels and lifetime suicidal ideation.
Compared with women in Ontario, distress was lower among women in Quebec. Individuals residing in Prairie provinces had higher probabilities of reporting lifetime suicidal ideation. The probability of lifetime suicide plan was higher among men living in Quebec and Prairie provinces.
After controlling for the difference in the observable factors, there was no significant difference in distress level between the non-Indigenous and Indigenous populations. However, the non-Indigenous population had lower probability of reporting lifetime suicidal ideation and lifetime suicide plan than the Indigenous population after adjusting for the observable characteristics (Table 2).
The coefficients and marginal effects obtained from the ordinary least squares and logistic models for psychological distress scale, lifetime suicidal ideation and lifetime suicide plan*
Explaining differences in psychological distress and suicidal behaviours
The mean score of psychological distress for the non-Indigenous population in Canada was 0.992 (women 1.208, men 0.814) points lower than for the Indigenous population. The Blinder–Oaxaca decomposition results suggested that the difference in the characteristics between the 2 groups explains 60% (women 51.2%, men 78.3%) of the absolute difference in the mean score of psychological distress. Differential distribution of factors, including age, household income and home ownership between non-Indigenous and Indigenous populations, accounted for the higher mean score of psychological distress among the Indigenous population. For example, if the Indigenous population had the same equivalized household income as the non-Indigenous population, the difference in the mean score of psychological distress could potentially decrease by 0.132 (women 0.132, men 0.133) points, all things being equal (Table 3, Figure 1).
Decomposition of the differences in psychological distress scale and the prevalence of lifetime suicidal ideation and suicide plan between non-Indigenous and Indigenous adults living off-reserve in Canada*
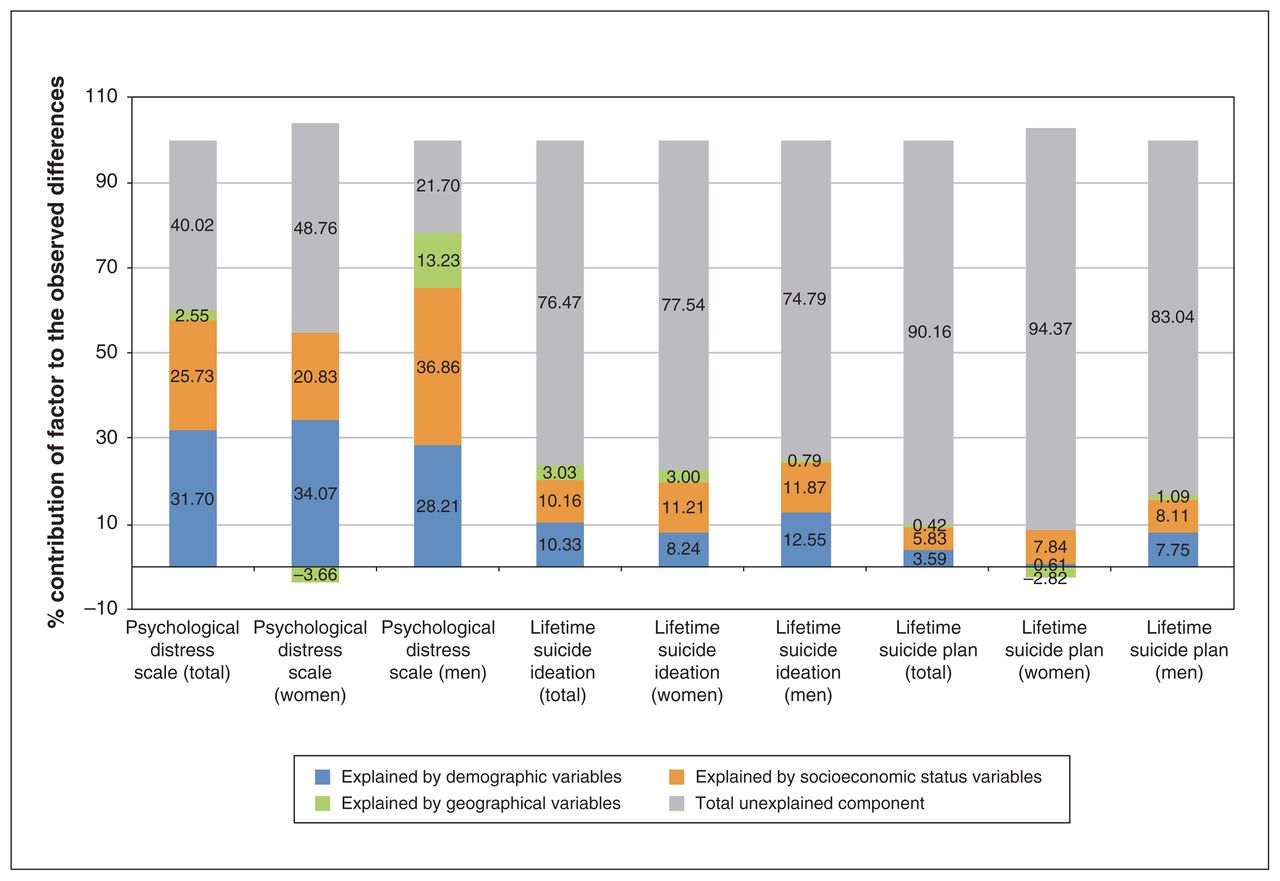
Percentage point contribution of explained and unexplained components to the differences in psychological distress scale and the prevalence of lifetime suicidal ideation and suicide plan between non-Indigenous and Indigenous adults living off-reserve in Canada. Percentage point contributions of explained component were calculated by dividing the sum of the contribution of all variables in each category by the total difference in the corresponding mental health outcome. Some percentages do not add up to 100 as a result of rounding.
The prevalence of lifetime suicidal ideation for the non-Indigenous population in Canada was 7.57 (women 9.39, men 5.90) percentage points lower than that of the Indigenous population. The decomposition results suggested that difference in the characteristics explained 23.5% (women 22.5%, men 25.2%) of the absolute difference in the prevalence of lifetime suicidal ideation. The differential distribution of factors, such as age, income and home ownership between the 2 groups, contributed significantly to the difference in the prevalence of lifetime suicidal ideation between non-Indigenous and Indigenous populations. The difference in income and home ownership between the 2 groups explained 0.36 (women 0.56, men 0.22) and 0.25 (women 0.27, men 0.26) percentage points of the difference in the prevalence of lifetime suicidal ideation, respectively (Table 2, Figure 1).
The prevalence of lifetime suicide plan for the non-Indigenous population in Canada was 4.48 (women 5.07, men 3.96) percentage points lower than that of the Indigenous population in Canada. The decomposition results suggested that difference in the characteristics explained 9.8% (women 5.6%, men 17.0%) of the absolute difference in the prevalence of lifetime suicide plan. If the Indigenous population had the same observed characteristics as the non-Indigenous population in Canada, the difference in the prevalence of lifetime suicide plan would have been reduced by 0.42 (men 0.68; the value for women was not statistically significant) percentage points. The differential distribution of income between non-Indigenous and Indigenous populations also contributed to the overall difference in the prevalence of lifetime suicide plan between the 2 groups (Table 3, Figure 1).
Interpretation
Health inequalities between non-Indigenous and Indigenous populations continue to exist in Canada, despite calls to action to address these gaps.33 One particularly concerning issue is the substantial differences in key mental health outcomes between the 2 populations in Canada,34,35 which were observed in the current analyses of the 2012 CCHS–MH. Similar to a recent study using data from the 2012 Aboriginal Peoples Survey,12 we showed a high prevalence of psychological distress and suicidal behaviours among Indigenous people living off-reserve in Canada. We found that mean psychological distress scores among the non-Indigenous population was 6.59% lower than that of the Indigenous population. The prevalence of lifetime suicidal ideation and suicide plan among the non-Indigenous population was also l.61 and 3 times lower, respectively, than that of the Indigenous population.
Our results indicated that the difference in the mean levels of psychological distress between non-Indigenous and Indigenous populations was mostly explained by the differences in levels of the explanatory variables between these groups, particularly for men. The differences in demographic factors accounted for a significant proportion of the differences in distress between the 2 groups. In particular, age differences between non-Indigenous and Indigenous adults accounted for one-third of the overall gap in distress between the 2 groups. Age contributed to the differences in distress levels between the 2 groups because distress decreased with increasing age and non-Indigenous adults are older than Indigenous adults; thus, distress levels of the Indigenous population would be less if the Indigenous population had the same age characteristics as the non-Indigenous population. Socioeconomic factors also accounted for a quarter of the difference in distress levels between the 2 groups. Improving socioeconomic status of Indigenous people through plans like income equalization may decrease the gap in psychological distress between non-Indigenous and Indigenous populations in Canada, particularly for men.
Unlike results for psychological distress, results for suicidal behaviours showed that the gaps in suicidal behaviours between non-Indigenous and Indigenous populations largely come from differences in the effects of the characteristics and unobserved determinants. This indicates that there are characteristics other than the variables in our model that affect suicidal behaviours that we are unable to observe or control. Nonetheless, our findings underscore the importance of the role of socioeconomic factors in accounting for differences in the prevalence of lifetime suicidal ideation and suicide plan. For example, improving the income of Indigenous people to the level of the non-Indigenous population could potentially reduce the prevalence of suicidal ideation by 0.25 percentage points (i.e., 1887 cases in our sample of 754 982) and suicide plan by 0.11 percentage points (i.e., 830 cases in our sample of 754 982) among Indigenous people.
Limitations
Our study is subject to several limitations. The CCHS–MH restricts survey respondents to people living in private dwellings and, thus, omits many Indigenous people with high risk of mental health issues, who might live in institutions (e.g., hospitals and prisons) and other collective dwellings (e.g., shelters and group homes).36,37 Because of the unavailability in the CCHS–MH, we could not assess the impact of some determinants of mental health outcomes such as food insecurity, the long-term effects of residential schools and the child welfare system, and numerous additional cultural, historical and contemporary factors that are known to be important specifically among Indigenous people. Some of the explanatory factors included in the analysis are likely to be endogenous, and together with the cross-sectional design, the reported associations do not necessarily imply causality. We could not consider those who have died by suicide in our study, also disproportionately represented among Indigenous populations.7
For the sample size consideration, we combined the 3 Indigenous populations for the analyses. Since differences in mental health outcomes exist among and within the 3 Indigenous groups in Canada,12 further studies need to evaluate specific Indigenous populations separately. Although we used the most recent available survey on mental health issues in Canada for the analyses, the survey was conducted in 2012. Updates by use of new surveys as they become available are needed. Although the number of dropout (missing) observations was very small in our analyses, there may be potential differences in missing observations between non-Indigenous and Indigenous populations. Finally, further studies are needed to evaluate Indigenous populations living on-reserve in Canada.
Conclusion
The differential distribution of socioeconomic factors between non-Indigenous and Indigenous populations explains a considerable proportion of inequalities in mental health outcomes between non-Indigenous and Indigenous populations living off-reserve in Canada. Thus, policies designed to improve major contributing socioeconomic determinants of health such as income may help reduce inequalities in mental health outcomes between the 2 populations. Interventions designed to address social determinants of health should fit the particular situational and cultural context of Indigenous people living off-reserve across Canada.
Acknowledgements
The analyses presented in this paper were conducted at Statistics Canada’s Atlantic Research Data Centre (RDC) at Dalhousie University, which is part of the Canadian Research Data Centre Network (CRDCN). The authors thank the CRDCN for facilitating the access to the CCHS–MH and the RDC analyst Heather Hobson for her support and assistance. The authors also thank Carol Hopkins and Thunderbird Partnership Foundation for reviewing the manuscript, and participants of the 53rd Annual Conference of the Canadian Economics Association, the 2019 Canadian Association for Health Services and Policy Research conference and the Community Health & Epidemiology Seminar Series at Dalhousie University for their comments and suggestions.
Footnotes
Competing interests: Mohammad Hajizadeh, Min Hu, Yukiko Asada and Amy Bombay report grants from Research Nova Scotia during the conduct of the study.
This article has been peer reviewed.
Contributors: All authors contributed to the conception and design of the study. Mohammad Hajizadeh and Min Hu performed the statistical analysis and all authors interpreted the results. Mohammad Hajizadeh drafted the manuscript, and Min Hu, Yukiko Asada and Amy Bombay helped with drafting and revisions. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: The authors acknowledge funding for this research provided by the Research Nova Scotia Establishment Grant program (Grant No. 1017).
Data sharing: The 2012 Canadian Community Health Survey — Mental Health (CCHS–MH) can be accessed by the researchers for approved projects at the Statistics Canada Research Data Centres.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/9/1/E215/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2021 Joule Inc. or its licensors
In this issue

{kind=link}
Article tools





