


Abstract
Background South Asians represent about 3% of the Canadian population and have a higher burden of certain cardiovascular risk factors and cardiovascular disease (CVD) compared with white people. The objective of this study was to review the literature to compare cardiovascular risk factors and disease management practices among adult South Asian and white Canadians.
Methods We searched MEDLINE, Embase, Cochrane and Cumulative Index to Nursing and Allied Health Literature databases from their inception through Feb. 17, 2014 and the reference lists of the selected articles. English-language studies of interventions and observational studies of biological mechanisms underlying CVD risk in South Asians conducted in Canada were eligible for inclusion. Where appropriate, we used random-effects meta-analyses to integrate results comparing the CVD risk profiles of South Asian and white Canadians.
Results We included 50 articles (n = 5 805 313 individuals) in this review. Compared with white Canadians, South Asian Canadians had a higher prevalence and incidence of CVD, an increased prevalence of diabetes (odds ratio [OR] 2.25, 95% confidence interval [CI] 1.81 to 2.80, p < 0.001) and hypertension (OR 1.11, 95% CI 1.02 to 1.22, p = 0.02), lower high-density lipoprotein cholesterol levels (mean difference –0.19 mmol/L, 95% CI –0.25 to –0.13 mmol/L, p < 0.001) and a higher percentage of body fat (men: absolute mean difference 3.23%, 95% CI 0.83% to 5.62%, p = 0.008; women: absolute mean difference 4.09%, 95% CI 3.46% to 4.72%, p < 0.001). South Asian people are also more sedentary, consume higher levels of carbohydrates and are less likely to smoke tobacco (OR 0.38, 95% CI 0.24 to 0.60, p < 0.001]) than white Canadians. No differences in access to diagnostic tests, outcomes following cardiovascular surgery or use of cardiac rehabilitation programs were apparent.
Interpretation Compared with white people, South Asian people living in Canada have a higher prevalence and incidence of CVD and possess a unique cardiovascular risk profile.
Almost 1 million South Asian people live in Canada (3% of the Canadian population) and represent one of the country’s fastest growing ethnic groups.1 Of the approximately 70% born outside Canada, 75% immigrated to Canada in the last 20 years.1
Evidence collected over the last 20 years suggests that rates of cardiovascular disease (CVD) and health behaviours vary among ethnic groups in Canada and that adoption of health behaviours typical of Western countries may promote the development of cardiometabolic risk factors among various ethnic groups.2 Initial research suggests that one group in particular, South Asians (i.e., people originating from India, Pakistan, Sri Lanka, Nepal and Bangladesh) have higher CVD rates than other groups,2–5 and these differences persist in their offspring.6 South Asian people also have more severe CVD, present with the disease at younger ages and, in some contexts, have differential access to diagnostic and treatment services compared with non–South Asian people.7–9
The health of the South Asian population is of great importance to Canadian society, and it is important to quantify their risk of CVD to inform health promotion strategies. We systematically reviewed the literature comparing South Asian people with white people living in Canada with respect to CVD risk factors, management, access to diagnostic testing and adherence to cardiac rehabilitation programs.
Methods
Search strategy and selection
In consultation with an information specialist, we developed search terms for MEDLINE, Embase, the Cumulative Index to Nursing and Allied Health Literature and the Cochrane Registry databases to identify human studies reporting associations among South Asian ethnicity, CVD risk factors and CVD. The initial search (conducted May 21, 2013) captured articles from database inception through May 2013; at the request of the CMAJ Open editors, the search was updated through to Feb. 17, 2014 (Appendix 1). Three investigators (A.R., R.dS. and S.S.A.) each screened a third of the titles and abstracts of the studies identified in the electronic search to arrive at a list of articles for full-text review. The same 3 reviewers assessed the eligibility of these full-text articles. Disagreements were resolved by discussion and consensus. Studies that were not published as full reports, such as conference abstracts and letters to the editor, were excluded.
Pairs of reviewers independently extracted study design characteristics and main results from each study. Missing variance measures were imputed using published formulae.10
Quality assessment and meta-analysis
Three reviewers independently assessed the risk of bias of each of the included studies on a scale from 1 (high risk) to 7 (low risk) and discussed their assessments to achieve consensus. A score for quality, modified from the Newcastle-Ottawa scale,11 was used to assess appropriateness of research design, recruitment strategy, response rate, representativeness of sample, objectivity/reliability of outcome determination, power calculation provided, and appropriate statistical analyses. Inverse variance random-effects weighted meta-analysis was done for both continuous and dichotomous outcomes (Review Manager, v. 5.2). The summary effect measures were the mean difference (MD) and 95% confidence interval (CI) for continuous outcomes: systolic blood pressure, diastolic blood pressure, total cholesterol, low density lipoprotein (LDL) cholesterol, high density lipoprotein (HDL) cholesterol, triglycerides, fasting blood levels of insulin and glucose, homeostasis model assessment of insulin resistance, body mass index (BMI), percentage body fat, waist-to-hip ratio and C-reactive protein. For dichotomous outcomes — smoking, diabetes mellitus, hypertension and obesity — the summary effect measures were the prevalence odds ratio (OR) and 95% CIs. Age- and sex-adjusted estimates were preferred. The presence of heterogeneity was assessed using Cochran’s Q test (considered significant at the p < 0.1 level) and quantified using the I2 statistic (ranging from 0% to 100%) using the cut-off points for important heterogeneity described by Higgins and colleagues.12 Because of the small number of studies, the prevalence and incidence of CVD, the prevalence of impaired fasting glucose and impaired glucose tolerance and summaries of differences in lipoprotein(a), the ratio of apolipoprotein B to apolipoprotein A-1, plasminogen activator inhibitor-1, physical inactivity, dietary intake and management of CVD were reviewed but not meta-analyzed.
Heterogeneity was explored through preplanned sensitivity analyses limited to high-quality studies (quality score ≥ 5) and by stratifying analyses by study type (administrative database v. cross-sectional) and sampling mechanism (random v. convenience). Heterogeneity is reported in Appendix 2, eTable 1. Secondary analyses examining heterogeneity are reported in Appendix 2, eTable 2 and Appendix 3.
Results
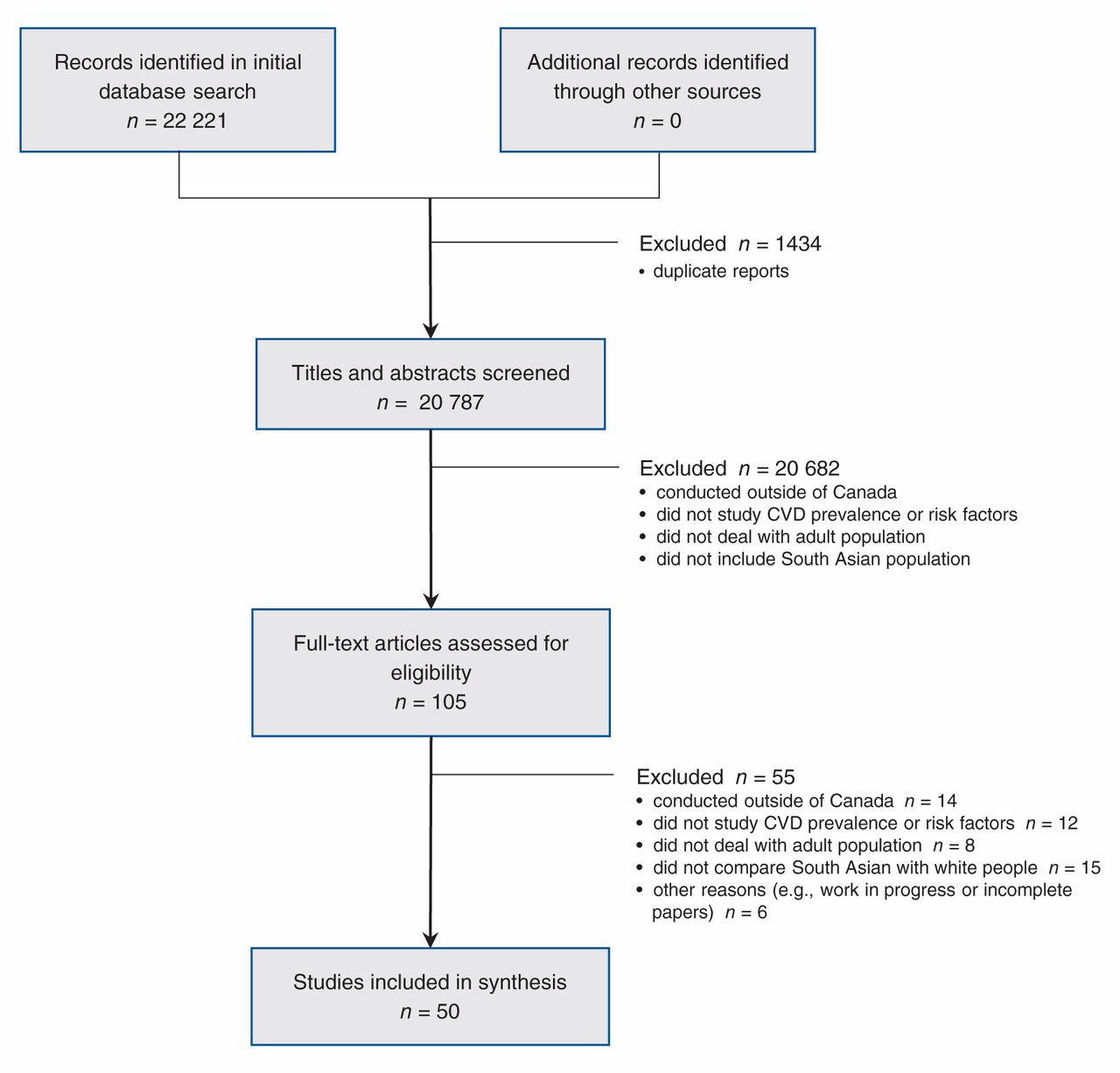
The search identified 22 221 potentially relevant articles, 22 116 of which were excluded after abstract review, leaving 105 for full-text review. Of these, 55 articles were excluded (Figure 1). The 50 included studies (n = 5 805 313 individuals) (Appendix 4) covered a long period, 1979 to 2007. Of these studies, 21 (42%) were cross-sectional, 24 (48%) were retrospective chart or database reviews, 2 (4%) were prospective cohort studies, 2 (4%) were descriptive studies and 1 (2%) was a case–control study.
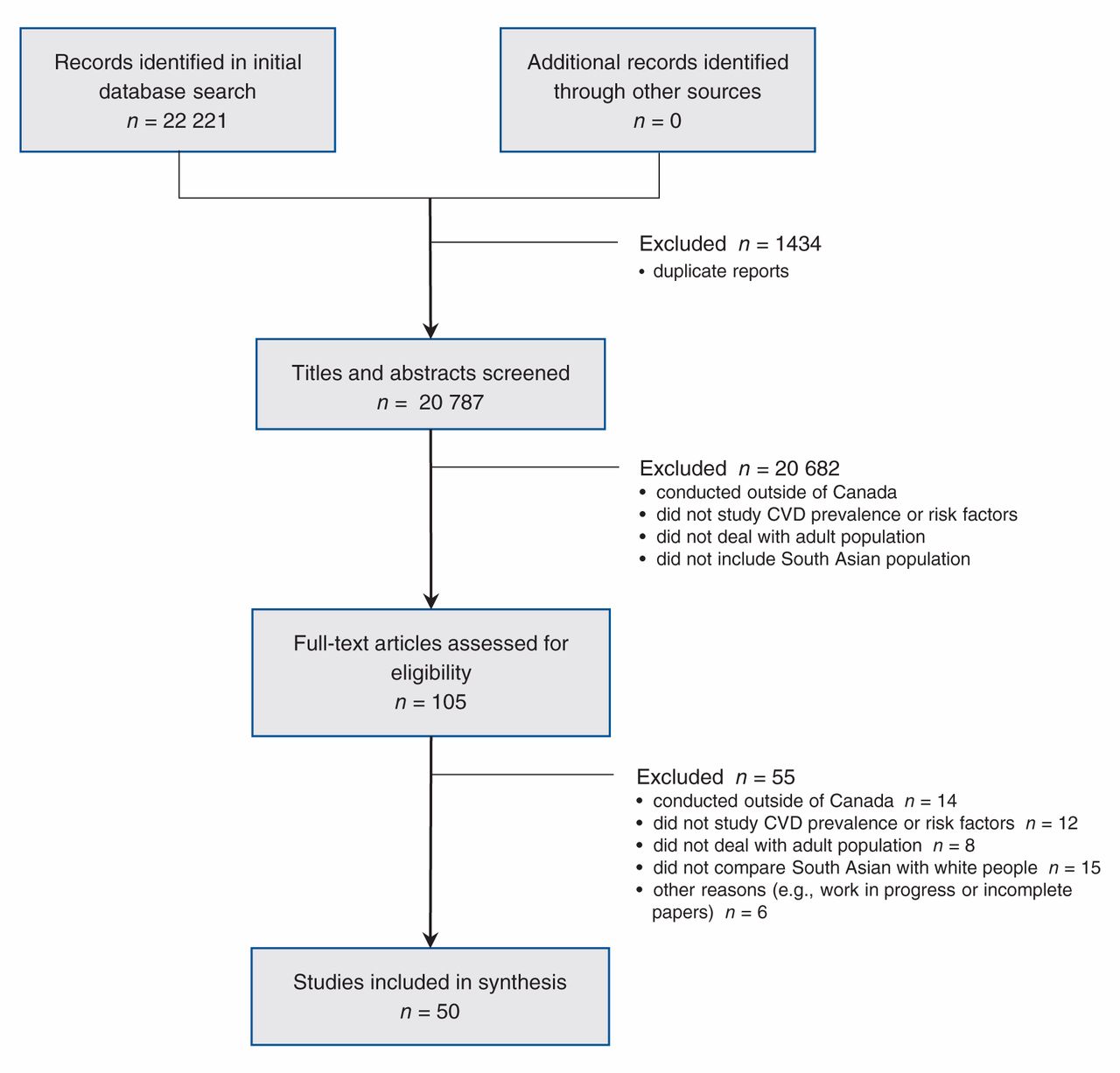
Selection of studies comparing cardiovascular risk factor and disease management practices among adult South Asian and white Canadians. CVD = cardiovascular disease.
Prevalence and incidence of heart disease
Compared with white people, South Asian people in Canada had a higher age-standardized incidence of acute myocardial infarction (MI): 4.97 events per 1000 population per year among South Asian men versus 3.29 among white men (p < 0.001); 2.35 events per 1000 population per year among South Asian women versus 1.53 among white women (p = 0.01).13 The prevalence of CVD (defined as a history of MI, angina, silent MI, percutaneous transluminal coronary angioplasty, coronary artery bypass grafting or stroke) was also higher among South Asian people: 5.7% to 10.0% versus 5.4% to 5.7% among white people (p < 0.05)3,4,14 (see Appendix 3 for details). Furthermore, from 1979 to 1993, sex-standardized rates of mortality from coronary disease were higher among South Asian people compared with white people: men, 42% versus 29% (p < 0.001); women, 29% versus 19% (p < 0.001).15
Risk factors
BMI and abdominal obesity
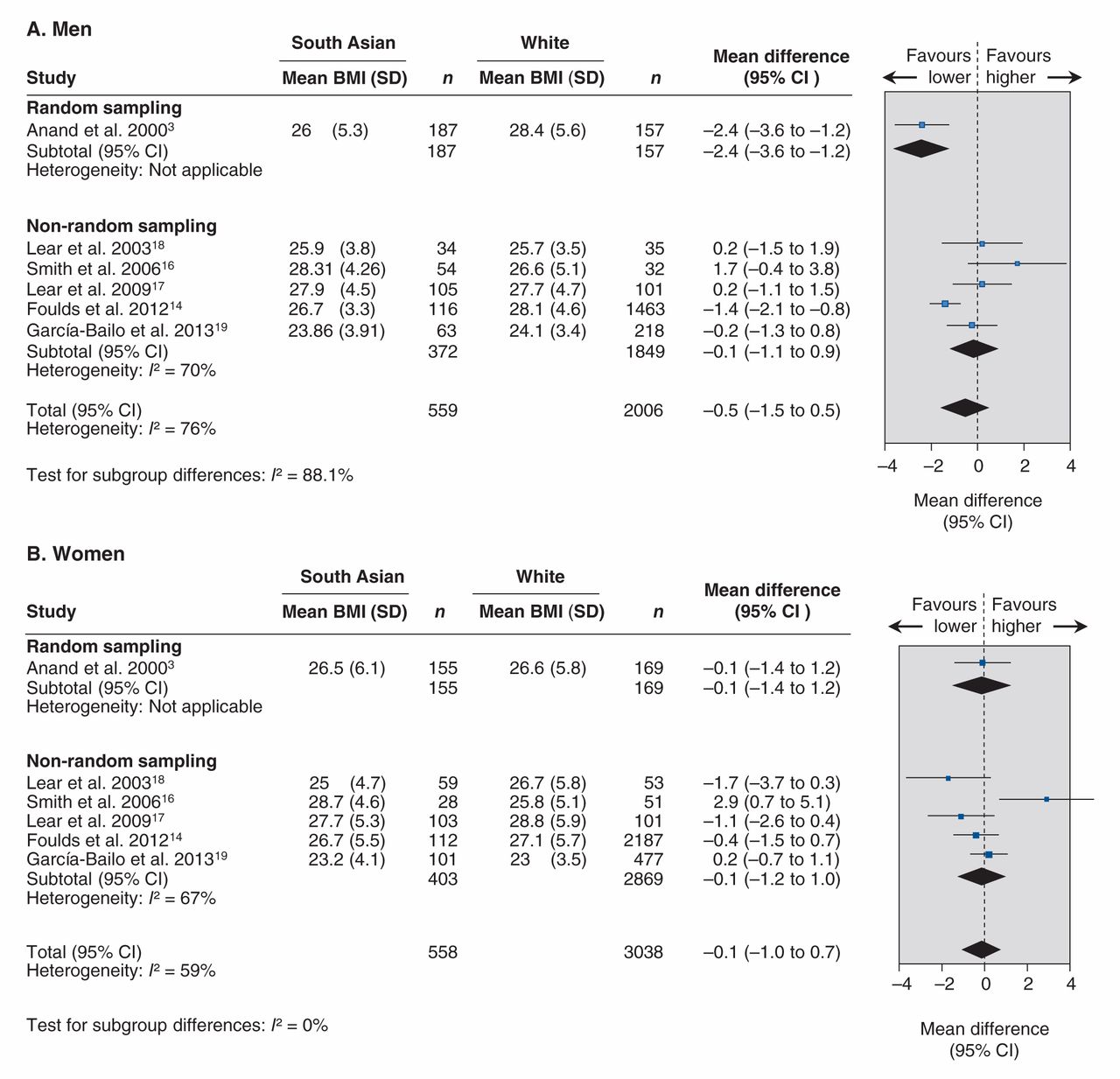
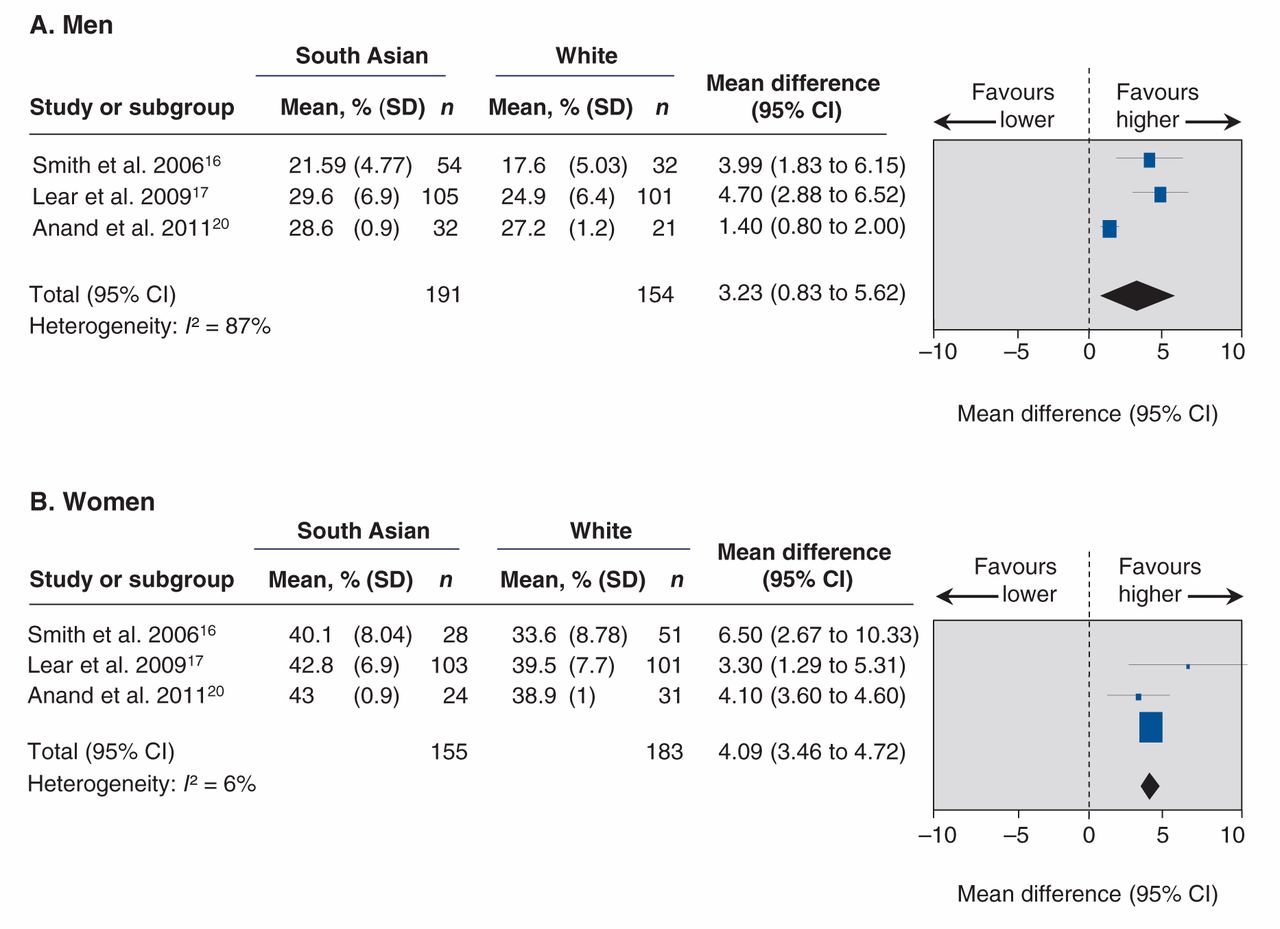
Although the BMIs of South Asian Canadians were similar to those of white Canadians (men: MD –0.52, 95% CI –1.51 to 0.47, p = 0.31; women: MD –0.14, 95% CI –0.99 to 0.74, p = 0.77) (Figure 2),3,14,16–19 South Asian people had a higher percentage body fat compared with white people (Figure 3)16,17,20(men: absolute MD 3.23%, 95% CI 0.83% to 5.62%, p = 0.008; women: absolute MD 4.09%, 95% CI 3.46% to 4.72%, p < 0.001) and South Asian women had a higher waist-to-hip ratio3,16–18,20(MD 0.02, 95% CI 0.01 to 0.04, p = 0.005). The prevalence of obesity (BMI ≥ 30)4,8,21was lower among South Asian people (OR 0.62, 95% CI 0.40 to 0.96, p = 0.03). No significant differences were found in waist-to-hip ratio3,16–18,20 between South Asian and white men or in sex-specific waist circumference14,17–20,22,23 (Appendix 2, eTable 1).

Meta-analysis of studies evaluating differences in body mass index between South Asian and white Canadian men (A) and women (B). A mean difference greater than zero indicates higher BMI among South Asian people. BMI = body mass index, CI = confidence interval, SD = standard deviation.
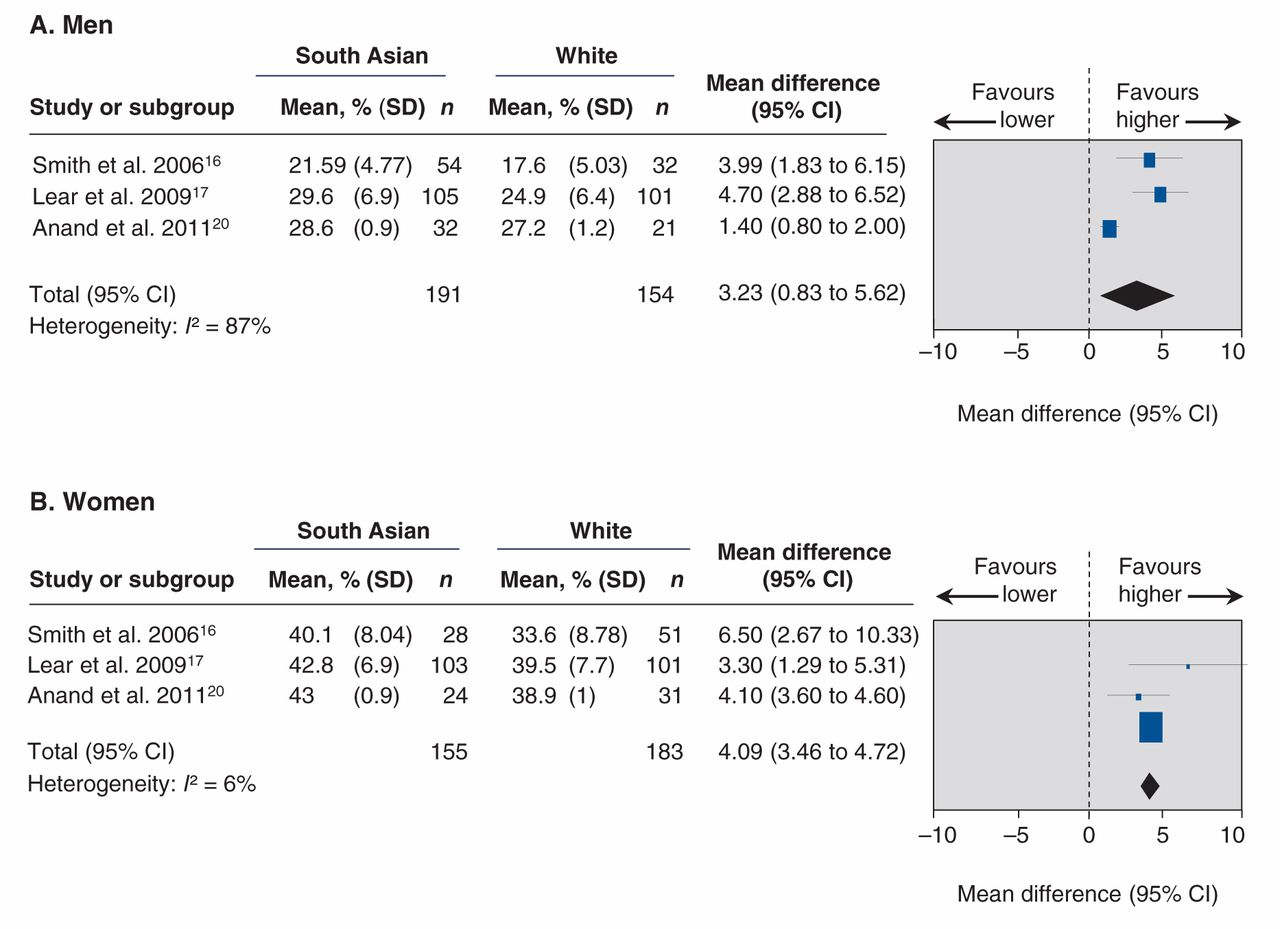
Meta-analysis of studies evaluating differences in percentage body fat between South Asian and white Canadian men (A) and women (B). A mean difference greater than zero indicates higher percentage body fat among South Asian people. CI = confidence interval, SD = standard deviation.
Fat distribution
South Asian men had a higher mean total abdominal adipose tissue than white men (439.7 cm2, standard deviation [SD] 169.5 cm2 v. 369.1 cm2, SD 164.0 cm2, p = 0.003), although there was no difference between South Asian and white women.24,25 Furthermore, South Asian people had less subcutaneous adipose tissue (as a percentage of total abdominal adipose tissue) than white people (MD –2.94%, 95% CI –5.56% to –0.32%, p < 0.05) and 17% more deep subcutaneous and visceral fat relative to superficial subcutaneous fat20,26(Appendix 3).
Type 2 diabetes and impaired glucose tolerance
Compared with white people, South Asian people had a 2-fold increase in point prevalence of diabetes3,4,9,14,23,27–36 (OR 2.25, 95% CI 1.81 to 2.80, p < 0.001) (Figure 4), an increased incidence of diabetes (new cases between 1993 and 2007),4,22,37–40 a greater prevalence of impaired glucose tolerance3,36 (Appendix 3), higher fasting insulin levels3,18–20,24,41 (MD 19.16 pmol/L, 95% CI 13.86 to 24.46 pmol/L, p < 0.001) and increased insulin resistance by homeostasis model assessment19,20,41–43 (MD 0.75, 95% CI 0.33 to 1.17, p < 0.001). No differences in fasting glucose levels3,18–20,24,41 were observed (Appendix 2, eTables 1 and 2).

Meta-analysis of studies evaluating the prevalence of diabetes among South Asian versus white Canadian men (A) and women (B). An odds ratio greater than 1.0 indicates an increased risk of diabetes among South Asian people. CI = confidence interval.
Blood pressure, hypertension
South Asian people had a lower systolic blood pressure than white people (MD –1.96 mm Hg, 95% CI –3.76 to –0.16 mm Hg, p = 0.03) but similar diastolic blood pressure3,18–20,24,41 (Appendix 2, eTables 1 and 2). However, South Asian people were more likely to have hypertension compared with white people3,4,9,14,27,28,31,32,34–36,41,44 (OR 1.11, 95% CI 1.02 to 1.22, p = 0.02).
Lipid levels
South Asian people had lower HDL cholesterol3,16,18–20,24,41 (MD –0.19 mmol/L, 95% CI –0.25 to –0.13 mmol/L, p < 0.001) and apolipoprotein A-1 levels,3,45 and a higher total cholesterol to HDL cholesterol ratio16,18–20,22,24 (MD 0.65, 95% CI 0.28 to 1.01, p = 0.0006), triglyceride levels3,18–20,24,41 (MD 0.20 mmol/L, 95% CI 0.02 to 0.37 mmol/L, p = 0.03), lipoprotein(a)3 and a ratio of apolipoprotein B to apolipoprotein A-116 than white people (Appendix 3). There were no significant differences in total cholesterol3,16,18,19,24,41 or LDL cholesterol3,18–19,24,41 (Appendix 2, eTables 1 and 2).
Diagnosis, management and outcomes
South Asian people appeared to delay presentation to hospital with symptoms of acute MI. The median time from symptom onset to presentation to a hospital in a southern Ontario sample9 was about 1 hour longer for South Asian people than white people (3.92 h v. 3.08 h, p = 0.04). Once in hospital, however, South Asian people and white people had similar access to diagnostic procedures and interventions2,7,8,27 for CVD, although there was some practice and outcome variation between provinces (Appendix 3). Following hospital admission for acute coronary syndrome, South Asians had higher short-term (< 1 yr) recurrent event rates, including readmission to hospital and recurrent angina, compared with white people.7,27,55–57 However, short-7–9,27,32,55,58 and long-term mortality7,27,31,32,34,51 after MI appeared to be similar among South Asian and white people (Appendix 3).
Interpretation
This review shows that South Asian people living in Canada have a higher prevalence and incidence of CVD compared with white people2,15 and possess a unique CVD risk profile. However, some inter-study variation exists in these results; we attribute this to differences in classification of ethnicity (i.e., self-report v. direct assessment v. surname classification), heterogeneity of South Asian populations (i.e., Pakistani v. Indian v. Bangladeshi) and differences in classification of outcomes (self-report v. health administrative data). This variation emphasizes the need to develop a standardized surveillance system for non-communicable diseases, such as CVD, cancer and lung diseases, by ethnic group in Canada.59 Such a system would generate information that would help shape health services, policies and programs aimed at particularly high-risk ethnic groups.
Explanation and comparison with other studies
Compared with white people, South Asian people living in Canada have a higher prevalence of hypertension; twice the prevalence of type 2 diabetes; greater insulin resistance; a higher percentage of body fat; higher visceral adiposity; a higher ratio of apolipoprotein B to apolipoprotein A-1; higher carbohydrate intake; lower HDL cholesterol levels; and lower levels of physical activity, all of which contribute to the etiology of CVD in this ethnic group. However, South Asian people in Canada are less likely than white people to smoke cigarettes. The sparse data available do not support differences in total cholesterol or LDL cholesterol levels between South Asian and white Canadians.
Although South Asian Canadians have conventionally “normal” BMI ranges, they have a higher percentage of body fat, increased visceral abdominal fat and greater insulin resistance4,60 compared with white people; these findings are consistent with those of US61,62 and British63 studies of immigrant South Asian populations. Greater insulin resistance in South Asian people may result from altered levels and actions of adipokines.64 The predisposition of South Asian people to this cardiometabolic risk profile may be a result of complex biological interactions between genetic and environmental factors. A comparative study showed that a greater proportion of newborns in South India have excessive body fat and higher umbilical cord blood insulin compared with white babies born in the United Kingdom,65 which suggests that insulin resistance develops in South Asian people in early infancy and portends increased risk of diabetes and CVD.66 Despite lower BMI, waist circumference and body weight, Canadian South Asian adolescents have higher triglyceride and lower HDL cholesterol levels than white adolescents, which shows that the adverse risk factor profile develops early among South Asians.6 The South Asian Birth Cohort (START) study67 is enrolling and prospectively following 1000 South Asian babies born in southern Ontario and will provide insight into the developmental origins of CVD risk factors in this ethnic group.
Health care access, including diagnostic cardiac tests and interventions, is similar among South Asian and white people, although there are interprovincial and contextual variations. For example, South Asian people living in Alberta and British Columbia are less likely than white people to undergo angiography in under 3 hours7 following an acute MI but are more likely to undergo angiography or cardiac catheterization at 30 days and 1 year after acute MI.8 However, a study in the greater Toronto area9 showed that South Asian and white people were equally likely to undergo angiography. We found no differences in short- or long-term mortality after MI; however, more data are required to understand the short-term clinical patterns after MI among South Asian people in Canada, as this may reflect variations in health systems. UK studies68–70 are conflicting: some show higher postoperative mortality among South Asian patients,70 whereas others show similar mortality rates between Asian and white patients.69
UK studies71 suggest that South Asian people are less adherent to cardiac rehabilitation programs than white people. Moreover, South Asian people with established CVD report worse health-related quality-of-life outcomes 1 year after angiography than white people with CVD.56 Lack of knowledge of the severity of CVD, differences in illness perception, lack of social support and stress associated with migration to Canada53,72–74 may contribute to this poor adherence.
Strengths and limitations
In this review, we pooled data from the largest studies of CVD risk in South Asian Canadians and examined sources of clinical and methodological heterogeneity. Our findings are generally consistent with UK68–71 and US61 studies. Limitations of this review include the low number of large studies of South Asian people living in Canada, the diversity of study designs and sampling schema and the lack of standardized measures of race or ethnicity (some studies based ethnicity on self-reporting, while others used an algorithm taking into account surnames and birthplace).
Substantial heterogeneity existed for most outcomes. The body of evidence posed particular problems with respect to methodologic and clinical heterogeneity because of differences in study design, sampling mechanisms and patient characteristics. The values for the I2 statistic were frequently in the 75% to 90% range, which signifies considerable unexplained heterogeneity. To maximize our ability to synthesize the data quantitatively, we combined cross-sectional, database, prospective and case–control studies. To accommodate this, we meta-analyzed the cross-sectional (i.e., single time point) associations between ethnicity and the risk factors.
We acknowledge that the populations in the individual studies may differ with respect to clinical characteristics, including age (45 to 60 yr), BMI range (24 to 28) and waist circumference (80 to 100 cm for men and 72 to 94 cm for women). Heterogeneity was explored through sensitivity analyses by study quality, and subgroup analyses by study types and sampling mechanisms (Appendix 2).
Despite the high level of heterogeneity, some important consistencies were found. First, in most individual studies, the point estimates were consistent with higher insulin, triglyceride and HDL cholesterol levels and a higher ratio of total cholesterol to HDL cholesterol in South Asian people than in white people. Second, when the analyses were stratified by sampling mechanism, the unexplained heterogeneity in adiposity was reduced to almost 0%. Residual differences may be attributable to lack of standardized definitions of ethnicity and varying study designs.
Conclusion
Compared with white people, South Asian people living in Canada have a higher prevalence and incidence of CVD, have twice the burden of diabetes and have a different cardiovascular risk profile. Given the increased prevalence and mortality associated with CVD among South Asian people living in Canada, etiologic studies to understand the development of these risk factors among children and youth and intervention strategies to reduce risk factors and CVD among this high-risk group are needed.
Supplemental information
For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/lookup/suppl/doi/10.9778/cmajo.20130064/-/DCI
Acknowledgements
We thank Arnav Agarwal and Sonia Ruparell for their assistance with extracting data for some of the articles. We also thank Dr. Katherine Cianflone, Dr. Bibiana Garcia-Bailo and Dr. Aman Nijjar for sharing their data and additional information about the studies with us. Dr. Sonia Anand holds the Michael DeGroote Heart and Stroke Chair in Population Health, a Canada Research Chair in Ethnicity and Cardiovascular Disease and the Eli Lilly May Cohen Chair in Women’s Health. Dr. Scott Lear holds the Pfizer/Heart and Stroke Foundation Chair in Cardiovascular Prevention Research at St. Paul’s Hospital. Dr. Russell de Souza is a recipient of a Canadian Institutes of Health Research postdoctoral research fellowship.
Footnotes
-
Competing interests: None declared.
-
Contributors: Ayesha Rana, Russell de Souza and Sonia Anand were responsible for study concept and design. Ayesha Rana, Russell de Souza, Sujane Kandasamy, Scott Lear and Sonia Anand were responsible for data acquisition. Ayesha Rana, Russell de Souza, Sujane Kandasamy and Sonia Anand analyzed and interpreted the data. Ayesha Rana, Russell de Souza, Sujane Kandasamy, Sonia Anand and Scott Lear drafted the manuscript. Ayesha Rana, Russell de Souza, Sonia Anand and Scott Lear revised the manuscript critically for important intellectual content. Ayesha Rana and Russell de Souza carried out the statistical analysis. Ayesha Rana, Russell de Souza and Sujane Kandasamy provided administrative, technical and material support. Sonia Anand supervised the study. All authors approved the final version of this article for publication and are willing to act as guarantors of this work.
References
- © 2014 Canadian Medical Association or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- Effects of lifestyle interventions on cardiovascular risk factors in South Asians: a systematic review and meta-analysis
- Barriers and facilitators to healthy active living in South Asian families in Canada: a thematic analysis
- Lifestyle interventions for type 2 diabetes management among migrants and ethnic minorities living in industrialized countries: a systematic review and meta-analyses