


- © 2004 Canadian Medical Association or its licensors
Between February and September 2003 Health Canada reported 438 probable or suspect cases of severe acute respiratory syndrome (SARS) resulting in 43 deaths1 primarily in the Greater Toronto Area (GTA). The basic reproductive number of 2–4 suggested a primary mode of transmission through contact of mucous membrane with infectious respiratory droplets or fomites,2,3,4 although airborne transmission was also suggested.5 In Toronto, there were several “super-spreading” events, instances when a few individuals were responsible for infecting a large number of others. At least 1 of these events occurred in an emergency department,6 where overcrowding, open observation “wards” for patients with respiratory complaints, aerosol treatments, poor compliance with hand-washing procedures among health care workers and largely unrestricted access by visitors may have contributed to disease transmission.
We outline the process successfully followed by 4 Toronto emergency departments (at Mount Sinai Hospital, North York General Hospital, Sunnybrook and Women's College Health Sciences Centre and the Hospital for Sick Children) involved in the assessment and treatment of 276 suspect and probable SARS cases between Mar. 13 and June 13, 2003, with no transmission to emergency department staff.
Modifications in operations
During the SARS outbreak the 3 emergency departments with respiratory isolation rooms initially assessed patients within existing facilities, and the 1 without such rooms triaged suspect cases to negative air pressure wards until a temporary isolation room in the emergency department was completed. One site subsequently constructed a large outdoor SARS assessment unit. Advance notification of the arrival of suspect cases allowed efficient use of isolation facilities.
General procedures for triage and management of patients in the emergency department during the SARS outbreak are outlined in Fig. 1 and Box 1. Patients who failed SARS screening were placed in respiratory isolation before any further assessment, including assessment of remaining vital signs. Suspect SARS cases sent to hospital by infection control were processed and often sent to the SARS ward immediately with no further interventions.


Fig. 1: Emergency department triage for SARS during an outbreak
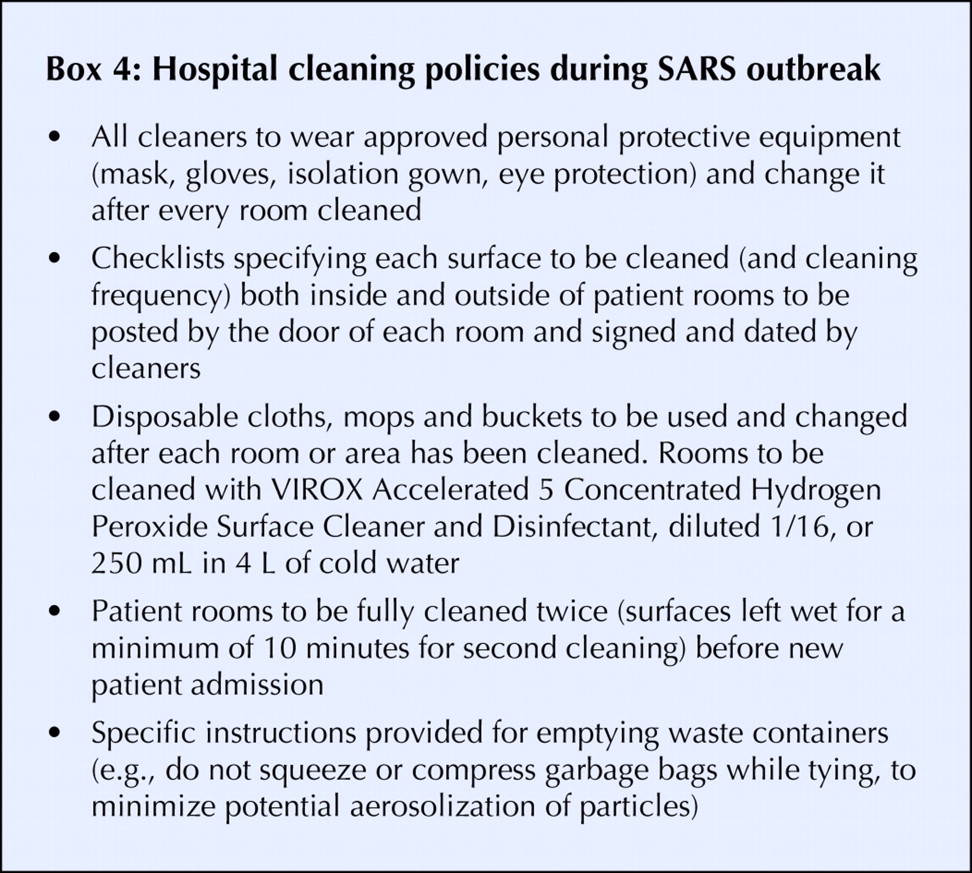
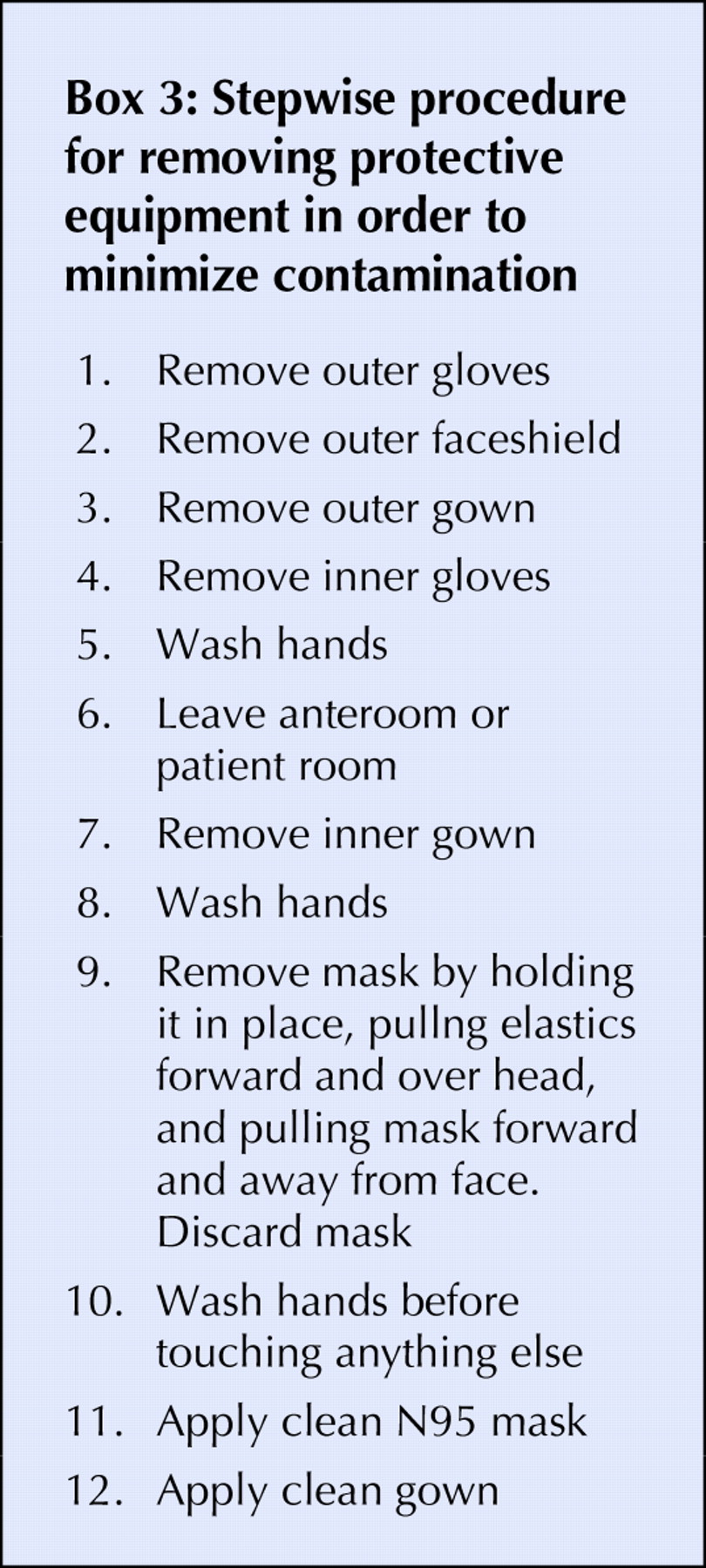
Modifications to daily operations were updated daily and notices posted by email and on bulletin boards. Procedure lists and protocols for donning and removing protective gear (Boxes 2 and 3) were posted, and equipment and garbage containers were arranged to facilitate compliance with SARS precautions. Non-essential equipment and furniture were removed from rooms to minimize contamination. Stethoscopes and other frequently used equipment were provided by the hospital and left in the rooms, whereas charts, pens and wireless phones were prohibited in rooms. Any equipment removed from rooms was disinfected using a hospital-approved disinfectant, and special policies were developed for cleaning patient rooms (Box 4).

Guards at entrances to the emergency departments restricted access to staff and emergency department patients only (no visitors or family), ensured compliance with protective measures and recorded names for contact tracing. A standardized hospital SARS classification governing patient transfers between institutions was developed by the SARS Provincial Operations Centre (www.oma.org/phealth/SARsCategories.htm) and significantly affected patient flow. Individual emergency departments were at times strained by large and unpredictable changes in patient volume when neighbouring institutions were closed because of uncontrolled exposure to or spread of SARS.
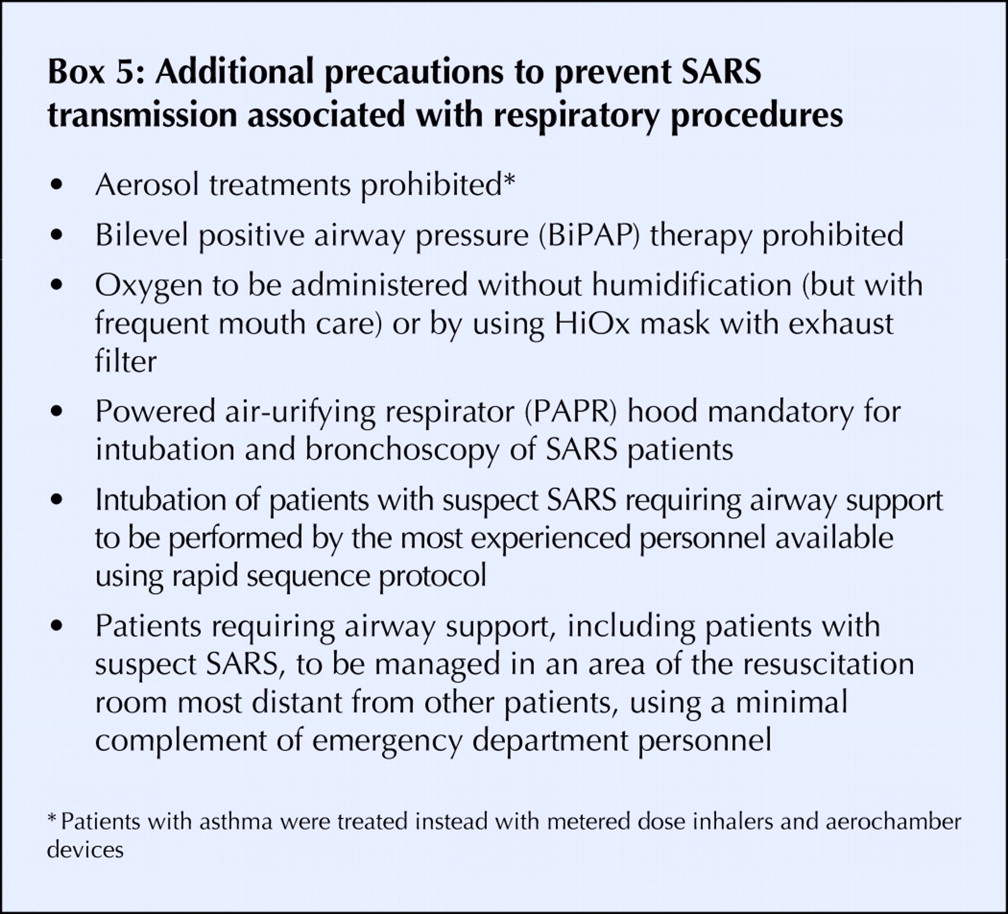
To accommodate increasing numbers of patients under investigation, some sites adjusted ventilation systems to create negative air pressure rooms (checked daily). All hallway stretchers were removed, and only 1 stretcher was permitted per room that had had multiple stretchers, which resulted in reduced emergency department capacity. As the outbreak came under control, a protocol was developed governing which patients could be separated only by a drape (i.e., those who were afebrile, passed SARS screening, were compliant with wearing approved masks and could be kept at least 1 m apart from each other). Protocols were developed to control patient movement (e.g., to radiology, wards, bathrooms), dispose of human waste and minimize the risk of SARS transmission associated with respiratory droplet aerosolization (e.g., through intubation with powered air-purifying respirator hoods, use of aerosolized therapies and pulmonary function testing) (Box 5).
Although some emergency departments in SARS-affected areas modified operations even more dramatically than the measures we describe,7 our experience suggests that the extra measures may not be required. The procedures we followed were protective against spread by respiratory droplets and fomites and were effective during several intubations and high-risk procedures.
Despite precautions, there were nonemergency department cases of SARS transmission in health care settings in Toronto,8 and these prompted control measures such as detailed guidelines for the management of high-risk airway procedures (www.health.gov.on.ca/english/providers/program/pubhealth/sars/sars_mn.html#1). The impact of these measures on emergency department practice is difficult to evaluate, and some measures remain controversial.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- Assessing the efficacy and safety of hydroxychloroquine as outpatient treatment of COVID-19: a randomized controlled trial
- Wanted: better public health training for family physicians
- Recherchee : une meilleure formation en sante publique pour les medecins de famille
- RNA Interference against Animal Viruses: How Morbilliviruses Generate Extended Diversity To Escape Small Interfering RNA Control
More in this TOC Section
Similar Articles
Collections

