


Abstract
Background: Black medical students have been consistently underrepresented in Canadian medical schools, and data on the impact of discrimination on their medical education remain limited. In this cross-sectional study, we aimed to investigate the experiences of Black medical students through the Black Medical Students’ Association of Canada (BMSAC).
Methods: We developed a 63-item instrument around the domains of inclusion and diversity, wellness, discrimination, career advancement and diversity in medical education. The anonymous web-based questionnaire was sent to 128 medical students and first-year residents from all 17 Canadian medical schools via the BMSAC listserv. We obtained frequencies for demographic data and self-reported experiences.
Results: We received 52 responses. Of respondents, 59% had at least 1 personal encounter with discrimination in medical school. Discrimination was experienced in both clinical and academic contexts, notably from patients, peers and hospital staff. Students further along in their medical training were more likely to endorse having experienced discrimination in medical school. Most respondents had positive experiences with academic and clinical inclusion, as well as resiliency in the face of discrimination. However, most respondents had negative experiences relating to reporting discrimination, their well-being, career advancement, sentiments of minority tax and low diversity in medical education.
Interpretation: We found that discrimination has important implications on the learning experiences of Black medical students surveyed from the BMSAC. This directly challenges the notion that Canadian medical schools are impervious to racism and highlights the need for advocacy and systemic changes to eliminate institutional racism.
Data about the compositional diversity of Canadian medical schools are limited. However, the few studies available report a common observation: Black medical students are disproportionately underrepresented compared with other minority groups.1,2 In 2018, Khan and colleagues surveyed medical students at 14 English-speaking Canadian medical schools.1 Among the 1388 students who responded (response rate of 16.6%), only 1.7% self-identified as Black in contrast to 6.4% of the Canadian Census population.2,3 In their qualitative study on under-represented Black, Hispanic and Native American residents from 21 residency programs, Osseo-Asare and colleagues describe that minority trainees face pervasive discrimination, experience feelings of “otherness” and lack in mentors.4 Participants also describe being burdened with promoting diversity in their institutions, often at the expense of traditional scholarly work more highly esteemed in academia — a phenomenon coined the “minority tax” in prior literature.5,6 In 1 longitudinal study on discrimination set in an undisclosed Canadian medical faculty, Black and other ethnic minority medical students facing daily microaggressions from peers often did not report instances of discrimination owing to fears of having their claims dismissed or lacking access to appropriate institutional support.7 The limited data on Black students’ experiences do not mean that disparities, discrimination and systemic exclusion are absent from Canadian medical faculties.8,9 Henry and colleagues’ landmark study on the experiences of racialized faculty in Canadian academia highlighted that universities reproduce the accepted social hierarchy in which nonwhite minorities are excluded and marginalized.10
Canadian universities and The Association of Faculties of Medicine of Canada have not consistently documented the ethnocultural background of medical school applicants and matriculants,2 perpetuating challenges with identifying the systemic and intersecting factors that interplay with the underrepresentation of Black students in medical education as well as understanding their experiences and differential outcomes.2,3 Developing institutional frameworks that address racism tailored to the Canadian context requires filling the knowledge gaps about discrimination among racialized medical students. The first Black Medical Students’ Association (BMSA) was formed by Dr. Sean Wharton in 1999 at the University of Toronto.11 Over the years, few local BMSAs were spearheaded in efforts of unifying Black minorities in medical education. In 2019, the first student-led pan-Canadian network called the Black Medical Students’ Association of Canada (BMSAC) was created to unify, support and foster equitable representation of Black students in all 17 Canadian medical schools.12
In this study, we sought to answer the following research questions: Do Black medical students registered with the BMSAC face discrimination in medical education? If so, what are these experiences? As Canadian medical schools devise strategies to diversify their student body, understanding the experiences of Black students in medical education is paramount to fostering a culture of inclusion and equity.
Methods
There are 17 Canadian faculties of medicine usually divided into 4 geographic regions: Ontario, Quebec, Atlantic and Western. Together, these faculties train about 10 000 medical students, all years combined.13 The number of self-identifying Black medical students and trainees across Canadian medical schools is currently unknown. Given the absence of institutional race-based data, our sample population is recruited from BMSAC. All self-identifying Black medical students studying in Canada are granted membership to the BMSAC.12 Membership is voluntary through registration on the website or social media. At the time of our study, the BMSAC had 128 active members.
Study procedure
This is a cross-sectional, descriptive study using an online, anonymous, voluntary and self-administered questionnaire. The recruitment material and SurveyMonkey link were sent to the BMSAC for dissemination through its listserv. The questionnaire was sent to all 128 members. Data collection occurred from Jan. 12, 2021, to Mar. 11, 2021. A snowball sampling method through the BMSAC regional directors was used to further optimize recruitment. The eligibility criteria included self-identifying as Black, and being a medical student enrolled at a Canadian faculty of medicine or a first-year resident who completed medical school at a Canadian faculty in 2020. First-year residents, alumni of BMSAC, were included in the cohort of participants given their recent completion of all 3 or 4 years of medical school and given that most of their experience in medicine could still be attributed to their undergraduate medical studies at the time of questionnaire dissemination.
Instrument design
The content of the questionnaire was adapted from validated questionnaires exploring minority students’ and faculty members’ perceptions of the medical school environment in the United States and United Kingdom.4,14,15 Our questionnaire was reviewed by a multidisciplinary group of professionals, including a social scientist (A.G.). It included 63 questions that began with exploring sociodemographic data and then 5 domains of interest, which are outlined below. Participants were asked to select in multiple choice or declare in free text their ethnocultural origin; “race” and “ethnocultural identity” were used interchangeably in our study. Other demographic data included respondents’ gender identity, native language, year of study and the geographic region of their medical school. We used household income during the second decade of life as a direct indicator of socioeconomic status. The quantitative online questionnaire included dichotomic closed-ended questions (yes or no) and closed-ended questions with 6-point Likert scales. The survey was offered in French and English (Appendix 1, available at www.cmajopen.ca/content/10/4/E937/suppl/DC1). Before dissemination, we piloted the questionnaire with 5 nonparticipants who were either non-Black minority medical students or Black professionals to assess the survey response process. Through their feedback, questions were reworded for clarity.
The work presented in this article forms the quantitative part of our mixed-methods study on the experiences of Black medical students in Canada. The qualitative phase of the study will be presented at a later date and will provide further information on the lived experiences of survey participants.
Data analysis
Guided by our literature review, we regrouped items of our questionnaire in distinct semantic dimensions designed to reliably assess various components of minority experience in medicine and guide our final data analysis. We ran an exploratory factor assay and Cronbach α reliability analysis to redefine our survey domains. We kept only dimensions or grouped questions that demonstrated good reliability with a Cronbach α coefficient higher than 0.7 (Table 1). Questions were measured by 6-point Likert scales. Scores were grouped as negative if coded from 4 (somewhat agree) to 6 (strongly agree). Descriptive data analysis consisted of frequencies for each reliable dimension or independent item responses. Missing data were omitted for the analyses. Analyses were performed in collaboration with an independent biostatistician using SPSS software version 25 (IBM SPSS Statistics).
Statistical characteristics of the survey domains’ assessment of minority experience among Black medical students
Ethics approval
Ethics approval was granted by the Health Sciences and Sciences Research Ethics Board of the University of Ottawa on Jan. 2, 2021 (ID no. H-08-20-5969).
Results
The survey was completed by respondents representing all 4 geographic regions (Ontario, Quebec, Atlantic and Western), including 13 of all 17 (76%) Canadian medical schools. According to the Accredited Canadian Faculties of Medicine, the 2019 incoming classes of the 13 programs represented in our survey included 2465 medical students; 83% of the total incoming medical student population in the country (2969).13 We received a total of 52 responses from the 128 active BMSAC members (41% response rate) (Table 2). Surveys were completed in 13.1 minutes on average. Our response sample had representation across all eligible years of study. Of respondents, 75% self-identified as women, and 25% self-identified as men. Owing to the small sample of MD and PhD students, their data were analyzed only in aggregate to maintain confidentiality.
Sociodemographic and professional characteristics of surveyed Black medical students in Canadian medical institutions
Most (94%) respondents reported that while growing up, their parents’ gross income was middle to high (above poverty line of $37 542 per year) (Figure 1).

Parental income distribution of surveyed Canadian Black medical students (n = 52). The threshold for “low income” was approximated to $40 000 and for “high income” to $125 000 annual gross salary of the respondents’ household during youth. As shown by the graph, most Black medical students came from middle to high socioeconomic class.
Academic and clinical inclusion
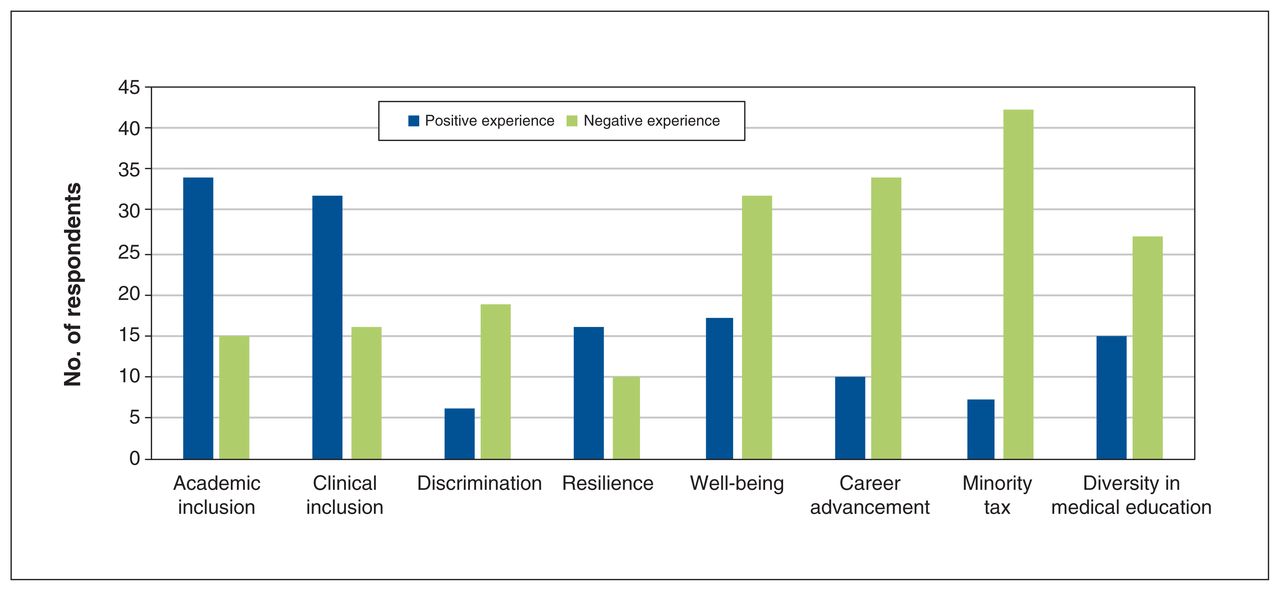
Sixty-nine percent (34/49) of participants responded positively to survey questions and statements ascertaining their perception of medical school belonging — agreeing that they belonged in their medical school community (Figure 2). Similarly, 67% (32/48) of the respondents indicated that they felt included or integrated in the medical team of their clinical settings.
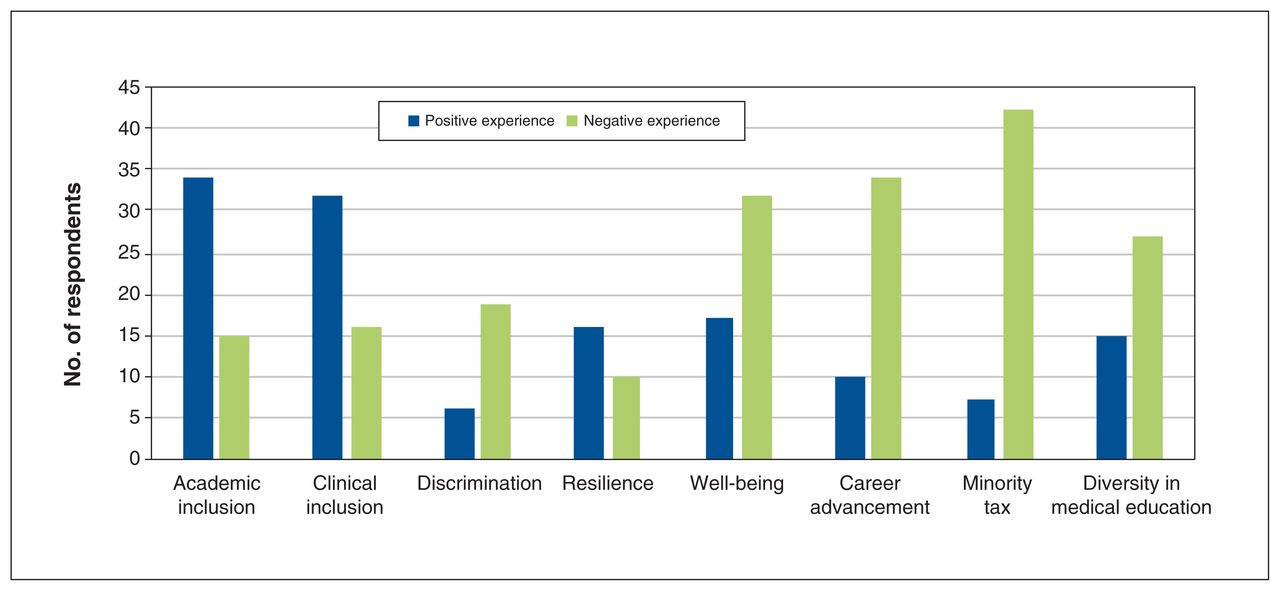
Frequency distribution of Black medical students’ perceptions and experiences in Canadian medical schools by survey dimensions (n = 51). Answers were graphed by frequency of positive (blue) or negative (green) responses. Six-point Likert scale responses were grouped as negative if coded from 1 (strongly disagree) to 3 (disagree), and as positive if coded from 4 (agree) to 6 (strongly agree). The resilience and discrimination survey domains had a smaller sample (n = 26) because experience with discrimination was a prerequisite to respondents answering these specific questions. Overall, we can visualize academic inclusion, clinical inclusion and resilience to have positive responses while all other domains were reported to be experienced as negative by survey participants.
Discrimination
Fifty-nine percent (30/51) of participants responded “Yes” to having experienced discrimination in medical school (Table 3). The sources of mistreatment were mostly from a “patient” or “student/resident or peer,” followed by “hospital staff physician, nurses or preceptors.” Most students shared these experiences with their student peers (81%, 21/26). Moreover, most students did not report these incidents: 31% (8/26) reported seeking institutional support and 27% (6/22) reported receiving institutional support (Table 3). A total of 76% (19/25) of respondents who experienced discrimination in medical school had negative experiences with reporting incidents (Figure 2). Whereas 20% (2/10) of first-year students responded “Yes” to experiencing discrimination in medical school, 100% of students in fourth year (6/6) or postgraduate year 1 (7/7) reported having experienced discrimination during their medical career (Appendix 2, available at www.cmajopen.ca/content/10/4/E937/suppl/DC1).
Surveyed Black medical students’ experiences with discrimination in Canadian medical school
Resilience
Sixty-two percent (16/26) of the respondents endorsed resilience statements when describing how they dealt with racial discrimination (Figure 2). In other words, most respondents agreed that their confidence or career advancement as a medical student were not negatively affected, despite experiences of discrimination.
Wellness
Of respondents, 65% (32/49) indicated that their well-being was poor in medical school, agreeing with statements indicating symptoms of burn-out in themselves (Figure 2).
Career advancement
Most respondents (80%, 35/44) agreed with statements that reported race or ethnicity negatively affecting their career advancement (Figure 2). The proportion of Black medical students reporting that being Black had a negative impact on their career advancement decreased from first year (90%, 9/10) to fourth year (33%, 2/6) (Appendix 2).
Minority tax
Most (86%, 42/49) participants agreed with statements that the phenomenon of the minority tax was regarded as a negative experience (Figure 2). Also, a higher proportion of female respondents (95%, 35/37) compared with males (42%, 5/12) agreed that being tasked as a “race ambassador” was viewed as a negative experience (Appendix 2).
Diversity in medical education
Of respondents, 64% (27/42) endorsed negative responses for questions asking whether they found their medical school faculty or medical curricula to be diverse in its representation (Figure 2).
Interpretation
Our findings show that Black medical students surveyed from the BMSAC are substantially affected by discrimination while training in Canadian medical schools. To date, little is known about the experiences of racism among Black medical students in Canada, and our study contributes to addressing this knowledge gap.
In our survey, most reported personal encounters with discrimination were experienced in both clinical and academic contexts, most notably from patients, peers and hospital staff. Students further along in their medical training were more likely to endorse having experienced discrimination in medical school. Respondents were more likely to report these negative experiences to peers rather than reporting to faculty or seeking institutional support. Only 1 in 3 respondents who experienced interpersonal discrimination reported incidents to their medical school, and even fewer sought out and received requested support. Although most respondents reported feeling included in their social interactions within clinical and academic settings and being resilient in the face of discrimination, our study results highlight that most Black medical students had negative experiences regarding reporting discrimination, their own wellness, their career advancement, feelings of being “taxed” as a minority and a lack of diverse representation in faculty and in curricula. These marginalized experiences of Black medical students as well as the pedagogical practices and perpetuation of inequity through inconsistent support are suggestive of institutional racism. As defined in Sir William Macpherson’s inquiry into the death of Stephen Lawrence, “[Institutional racism is] the collective failure of an organization to provide an appropriate and professional service [and it is] detected in processes, attitudes and behaviour which amount to discrimination through unwitting prejudice, ignorance, thoughtlessness, and racist stereotyping which disadvantage minority ethnic people.”16
Many of our findings are consistent with those of prior studies about systemically excluded minority groups in medical education. In the University of Toronto’s Temerty Medicine Voice of the MD Student 2021 survey report, 56% of current Black medical students said that they had experienced discrimination at least once in the past academic year.11 Mpalirwa and colleagues’ 2020 qualitative study about Ontarian Black residents and physicians found that more than 70% of respondents experienced mistreatment from patients, peers and preceptors,9 and this is consistent with our finding that exposure to racism begins early in medical training and persists throughout training. Other studies outside of Canada similarly indicate that Black and minority ethnic medical students are unlikely to report discrimination, as reporting is perceived to be ineffective and victimizing.17 This suggests that medical school administrators may be unaware of interpersonal racism experienced by their students and, paradoxically, the denial of these negative experiences renders them ill-equipped to properly support affected students. Moreover, in their review of 28 studies on under-represented minorities in medicine, Orom and colleagues describe that minority students were more likely to experience discrimination, have poorer self-esteem, have a smaller social network and have more difficulties finding mentors than their white counterparts.18 If left unaddressed, this adverse learning climate will continue to entrench attainment gaps in medical education and advancement among underrepresented minorities.
Traditionally, excellence has been a unifying framework in academic and medical communities; now more than ever, it becomes important to integrate social accountability within the narratives of excellence, with the goal of ultimately aligning excellence with societal outcomes.19,20 As faculties continue to expand their equity practices beyond anti-discrimination policies, mitigating the occurrence and impact of discrimination requires a comprehensive antiracism plan involving all key actors.10 This could include antiracism training for faculty, nonstereotypical diversity representation in the curriculum and the creation of an institutional service dedicated to addressing inequity complaints while promoting equity. Finally, disrupting inequities also requires a review of inaccurate use of “race” as a biological entity in medicine and academia.21 The consistent use of “race” as a social construct would allow a better understanding of racism as a risk factor stemming from the individual’s relation to societal norms and not from within the individual themselves.22
Limitations
Our study population is drawn from BMSAC members. Since membership to the BMSAC is voluntary, this sample remains a proxy to the nominal demography of Canadian Black medical students. Also, there were no respondents from 4 institutions (Table 2). This could indicate low regional engagement of self-identifying Black individuals with BMSAC or, more systemically, disproportionately low numbers of Black individuals in these 4 medical schools or rural regions.23 Black individuals remain historically under-represented in research studies owing to mistrust, cultural barriers, racial stigma and discomfort disclosing sensitive information.24,25 Despite this limitation, our response rate is in keeping with that of similar surveys on underrepresented Canadian and American medical students in literature, namely those with self-reported 2SLGBTQIA+ identity and disability status.26,27
Conclusion
Our study highlights the experiences of discrimination faced by Black medical students registered with BMSAC, and our findings directly challenge the conception that Canadian medical schools are impervious to racism. Future qualitative studies could provide more in-depth understanding to further inform medical faculties’ strategic policy changes. There also remains a pressing need for systematic race-based data collection to identify and address inequities in medical education. As we move toward enhancing equity and inclusivity in Canadian medical education, academic institutions must commit to bringing awareness and creating sustainable systemic changes through multidimensional and interdisciplinary antiracist approaches.
Acknowledgements
The authors extend their thanks to Joseph Abdulnour, biostatistician at the Institut du Savoir Montfort, for his dedicated work in analyzing the data for this project. The authors also thank Sara N. Mwamba for the expert contribution provided throughout this project, including in the manuscript review. Sara N. Mwamba is a sociologist who has offered her expertise in interethnic relations to a wide range of Canadian organizations. Her research interests centre on the African, Caribbean and Black experience in Canadian medical and health systems as it relates to blood donation. The authors also thank the Black Medical Students’ Association of Canada for collaborating in the dissemination of the questionnaire and the Association Médicale Universitaire de l’Hôpital Montfort for financing the research project. Finally, the authors thank the Office of Francophone Affairs at the Faculty of Medicine of the University of Ottawa for its continued support throughout this project.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Johanne Mathieu, Kien Crosse and Lolade Shipeolu conceived of the presented idea. Gaelle Bekolo and Salomon Fotsing were involved in planning and supervising the work. Abdoulaye Gueye reviewed the instrument. Johanne Mathieu, Kikelomo Akinbobola, Salomon Fotsing and Gaelle Bekolo processed the experimental data and performed the analysis. Johanne Mathieu and Gaelle Bekolo drafted the manuscript. Johanne Mathieu designed the figures. Johanne Mathieu, Kikelomo Akinbobola, Kimberley Thomas, Manon Denis-LeBlanc, Salomon Fotsing and Gaelle Bekolo aided in interpreting the results and worked the subsequent versions of the manuscript. All authors discussed the results and commented on the final manuscript. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: The authors Johanne Mathieu, Lolade Shipeolu, Kien Crosse, Salomon Fotsing and Gaelle Bekolo received funding from the Association des Médecins Universitaires de l’Hôpital Montfort.
Data sharing: The data that support the findings of this study are available on request from the corresponding author, Johanne Mathieu. The data are not publicly available owing to information that could compromise the privacy of research participants.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/10/4/E937/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2022 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
Article tools


