


Abstract
Background: As women with HIV live longer, the need for age-appropriate breast cancer screening will increase. We compared rates of screening mammography among women with and without HIV.
Methods: We used administrative health databases to identify all women in Ontario, Canada, who were eligible for screening mammography (aged 50 to 74 yr and no history of breast cancer) as of Apr. 1, 2011. We used multivariable log-binomial regression to compare the 2-year period prevalence of screening mammography in 2011 to 2013 among women with and without HIV and to examine the correlates of screening among women with HIV.
Results: We identified 1 447 015 screen-eligible women, among whom 623 (0.04%) were women with HIV. Women with HIV were less likely to undergo screening than women without HIV (50.1% v. 63.4%, p < 0.001). Following multivariable adjustment, HIV-positive status was associated with significantly lower odds of undergoing mammography (adjusted prevalence ratio [PR] 0.83, 95% confidence interval [CI] 0.77-0.89). Compared with women with HIV receiving regular care from both a family physician and an HIV specialist, women with HIV receiving neither kind of care (adjusted PR 0.64, 95% CI 0.50-0.83) or predominantly specialist care (adjusted PR 0.77; 95% CI 0.60 to 0.97) were less likely to undergo screening mammography.
Interpretation: Women with HIV are less likely to undergo breast cancer screening mammography than women without HIV. Addressing this disparity requires optimizing care delivery to ensure adequate provision of comprehensive primary care to people with HIV.
Breast cancer is the most common malignancy and second leading cause of cancer-related death among women in North America, causing an estimated 5000 deaths among Canadian women in 2015.1 Although breast cancer incidence among women with HIV is similar to that in the general population, some studies report that women with HIV have more advanced disease at initial diagnosis and greater risk for breast cancer-related death than those without HIV.2 HIV imparts a greater risk of myelosuppression during chemotherapy, resulting in treatment interruption, early cessation of therapy and adverse outcomes.3,4
Screening mammography allows for earlier detection of breast cancer and has been shown to reduce mortality in women aged 50 to 69 years.1 Because women with HIV are living longer, the need for age-appropriate breast cancer screening will increase.5,6 However, use of mammography by women with HIV in developed settings has been poorly characterized. Past studies have been limited by samples that were small, not population based, or lacking in comparison groups without HIV.7-12 Such data are important because women with HIV may possess numerous intersecting vulnerabilities associated with inadequate screening, including low socioeconomic status, immigration and mental illness.13-16Moreover, the complexity of managing HIV and associated comorbid conditions means that preventive care may get less attention than it otherwise would.10,12 We aimed to compare the use of breast cancer screening mammography among women with and without in HIV in Ontario, Canada, and identify correlates of screening using large provincial administrative databases.
Methods
Setting
We conducted a population-based study comparing receipt of mammography among screen-eligible women living with and without HIV infection in Ontario from Apr. 1, 2011, to Mar. 31, 2013. Ontario has single-payer, universal coverage for physician services, including screening mammography. Women can receive screening either through the Ontario Breast Screening Program (OBSP), an organized province-wide network of screening sites, or through non-OBSP- affiliated centres funded by the Ontario Health Insurance Plan (OHIP). Provincial guidelines recommend screening at 2-year intervals for women aged 50 to 74 years who are at average risk for breast cancer, irrespective of HIV status.17
Data sources
We used Ontario's administrative health databases, which are held securely in linkable files without any direct personal identifiers at the Institute for Clinical Evaluative Sciences (ICES). We identified individual demographic information such as age, sex and residential postal code using the Registered Persons Database (RPDB), which serves as the base population file of the majority of Ontario's 13.5 million residents who are eligible for provincial health care coverage. We used the Ontario Cancer Registry (OCR), which records all cancer diagnoses and deaths among Ontario residents, to exclude women with a prior diagnosis of breast cancer; the OCR has an estimated 95% capture across cancer diagnoses.18,19 We used the Immigration, Refugees and Citizenship Canada database to identify immigrants to Ontario and their country of origin; this database has a linkage rate of 86.4% to the RPDB.20 We obtained data regarding patient enrollment with family physicians and physician demographics and training through the Client Agency Program Enrolment registry (for which the Ontario Ministry of Health and Long-Term Care updates rostering of individuals to family physicians on a monthly basis) and the ICES Physician Database (which comprises information from the OHIP Corporate Provider Database [CPDB], the Ontario Physician Human Resources Data Centre [OPHRDC] database and the OHIP database of physician billings). We used the OHIP database, which captures almost all physician billing, to identify number of primary care visits. We determined receipt of mammography using data from the OBSP, provided by Cancer Care Ontario, and from the OHIP database using fee codes X185, X171 and X178.
Study population
We used the RPDB to identify all women between 50 and 74 years of age living in Ontario who were eligible for screening and eligible for health insurance as of the index date, Apr. 1, 2011. Next we identified women with HIV using a validated case-finding algorithm,21 with the remaining women without HIV serving as the comparison population. From both groups, we excluded women with a history of breast cancer or mastectomy and women who died during the study period to ensure all had 2 years of follow-up.
Outcomes
Our primary outcome was the receipt of a screening mammogram during the 2-year period following the index date, Apr. 1, 2011.
Statistical analysis
We compared the baseline distribution of characteristics between women with and without HIV using standardized differences, with less than 0.1 indicating good balance between groups.
For the primary analysis, we compared the receipt of mammography between women with and without HIV using multivariable log-binomial regression models. We used a non-parsimonious model, adjusting for clinical and health service covariates associated with screening mammography, including age, urban versus rural residence,22 socioeconomic status, immigration status (non-immigrant, recent [< 5 years from index date] immigrant from HIV-endemic country, recent [< 5 years from index date] immigrant from non-HIV endemic country, non-recent immigrant from HIV-endemic country, non-recent immigrant from non-HIV-endemic country) and comorbidity. We determined socioeconomic status at the neighbourhood level using postal code information and Statistics Canada census data. We ascertained comorbidity burden in the preceding year using the Johns Hopkins Adjusted Clinical Groups case-mix assignment software (Sun Microsystems Inc.).23 We used Aggregated Diagnosis Groups (ADGs), which are clusters of diagnostic codes that are similar in terms of severity and expected persistence. The number of ADGs ranges from 0 to 32, with a higher number reflecting a higher level of diagnosed comorbidity.
We also adjusted models by physician characteristics, including age, sex and practice model. We identified women's family physician enrollment using the Client Agency Program Enrolment registry; those who were not enrolled were assigned to the family physician who provided the majority of their primary care during the study period. Almost three-quarters of Ontario's population are enrolled with physicians practising in one of several types of reimbursement and organizational practice models, which differ in characteristics such as the presence of interprofessional teams. The categories of these models were as follows: capitation - team based (e.g., Family Health Teams with allied health support); capitation - non-team based (e.g., Family Health Networks, Family Health Organizations); enhanced fee for service (e.g., Family Health Groups); traditional fee for service; and other.24 We counted women's number of primary care visits in the year before the study period. We classified women's patterns of care on the basis of whether they had at least 3 visits to their family physician, at least 3 HIV-specific visits to an infectious disease or internal medicine physician (International Classification of Diseases, 10th revision [ICD-10] billing code 042, 043 or 044), both kinds of care, or neither kind of care during the 2-year period. Unlike other jurisdictions in which internal medicine may include physicians in generalist practice, in Canada, physicians who practise internal medicine act as consultant physicians.
In secondary analyses, we determined predictors for screening in women with HIV only. We adjusted models for all patient, provider and practice characteristics listed above.
We used SAS version 9.3 statistical software (SAS Institute Inc.) for all analyses.
Ethics approval
Ethics approval was obtained from the Sunnybrook Health Sciences Centre Research Ethics Board on Aug. 12, 2015. This research ethics board has an agreement with ICES that allows it to conduct research using the anonymized administrative databases held at ICESwithout need for independent research ethics board review; thus, no approval number or ID is given. ICES is named as a prescribed entity under Section 45 of the Personal Health Information Protection Act (Ontario Regulation 329/04, Section 18). Under this designation, ICES can receive and use health information without consent for the purposes of analysis and compiling statistical information about the health care system of Ontario.
Results
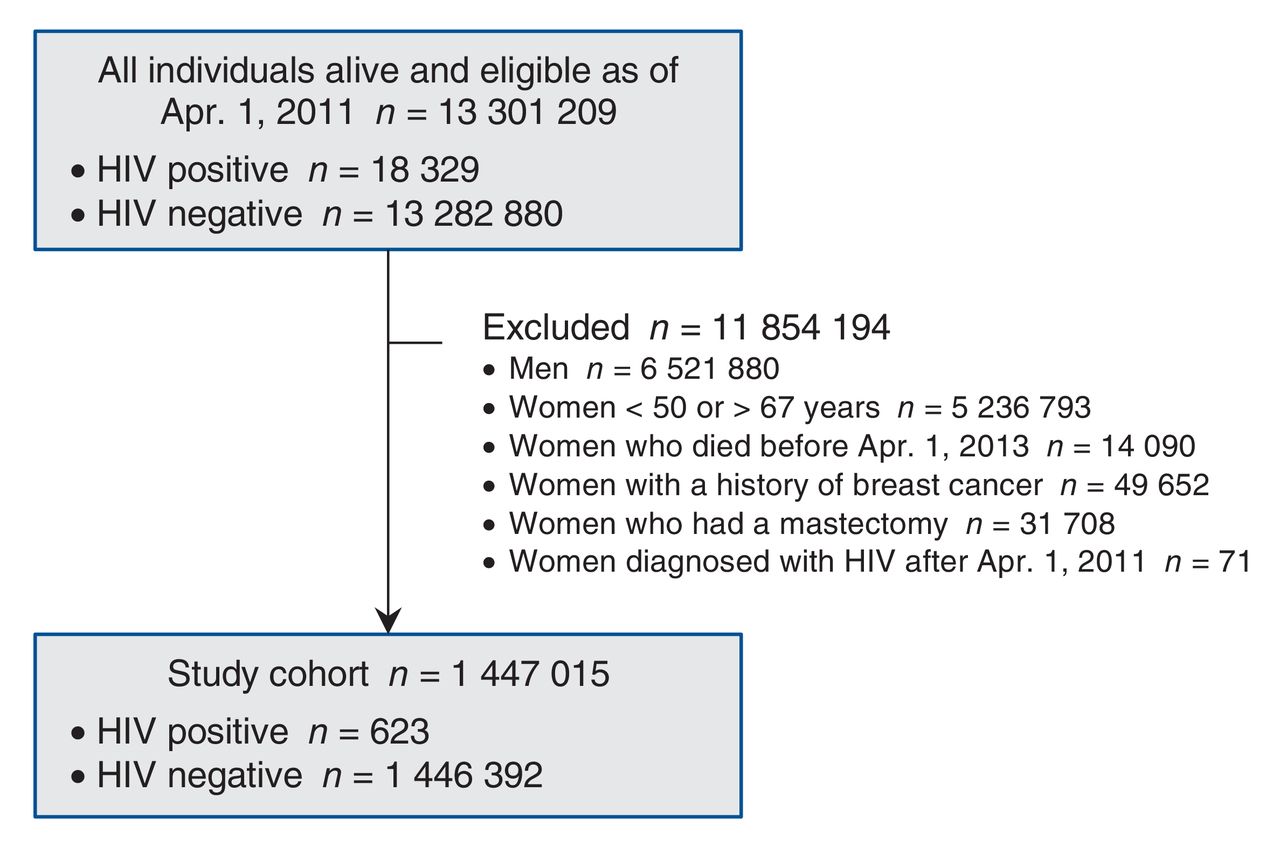
We identified 1 447 015 women eligible for mammography screening during our study period, of whom 623 (0.04%) were living with HIV (Figure 1).
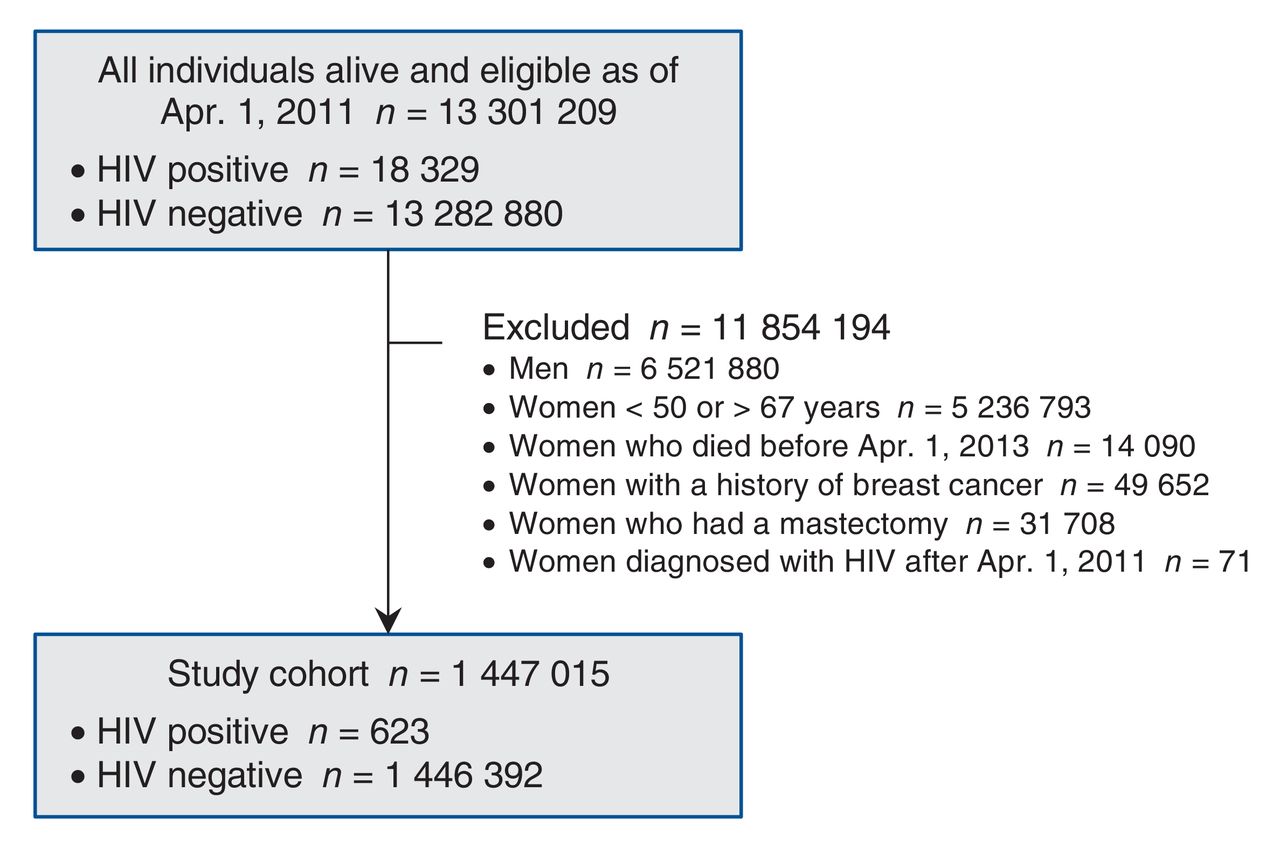
Figure 1: Study flow diagram.
Analyses of women with HIV compared with women without HIV
Women with HIV were younger, disproportionately represented in low-income neighbourhoods and more likely to be immigrants (Table 1) than women without HIV. The family physicians caring for women with HIV were younger and less likely to be female than were those caring for women without HIV. Women with HIV were less likely to be receiving primary care in any of the enrollment models and had more primary care visits than women without HIV.
Our first multivariable analysis considered the complete cohort of women (Table 2). Three hundred and twelve (50.1%) women with HIV underwent screening mammography during the 2-year follow-up period, compared with 916 775 (63.4%) women without HIV (Table 1). Following multivariable adjustment, women with HIV were less likely to undergo screening mammography than women without HIV (adjusted prevalence ratio [adjusted PR] 0.83, 95% confidence interval [CI] 0.77-0.89). Having a female primary care physician (adjusted PR 1.09, 95% CI 1.09-1.09) and having had a minimum of 3 visits to a primary care physician in the preceding year (adjusted PR 1.43, 95% CI 1.42-1.43)were also associated with undergoing mammography.
Analyses restricted to women with HIV
Women with HIV who underwent mammography were more likely to live in high-income neighbourhoods (27.3% v. 21.5%; p < 0.001), have a high comorbidity burden (30.4% v. 24.4%; p = 0.002) and have a female primary care physician (36.9% v. 25.7%; p < 0.001) (Table 3) than those who did not undergo mammography. Women with HIV who underwent mammography were more likely to be enrolled in capitation models other than Family Health Teams, have more primary care visits and receive regular care from their family physician either alone or in conjunction with an HIV specialist.
Among women with HIV, before adjustment, higher comorbidity was associated with increased prevalence of screening, as was type of physician care received; compared with women receiving both regular family physician care and regular HIV specialist care, women who saw only a specialist or who had neither kind of care were less likely to undergo screening. Following multivariable adjustment, only type of physician care received was associated with mammography receipt; compared with women receiving both regular family physician care and regular HIV specialist care, women who saw only a specialist (adjusted PR 0.77, 95% CI 0.60-0.97) or who had neither kind of care (adjusted PR 0.64, 95% CI 0.50-0.83) were less likely to undergo screening (Table 4).
Interpretation
In this population-based study, women with HIV in Ontario were less likely to receive breast cancer screening than women without HIV. Furthermore, only half of all screen-eligible women with HIV received a mammogram during the 2-year study period. Among women with HIV, receipt of regular primary care either alone or in conjunction with care by an HIV specialist was associated with more screening.
Despite the fact that women in our cohort had access to mammography without cost, the percentage of those with HIV who underwent screening was lower in our population, at 50.1%, than that reported in many studies among women with HIV,7,9,11 but it was similar to25 or higher than that reported in others, where the prevalence of completed screening was as low as 31% among some cohorts.10 After adjustment, we found no patient characteristics were associated with breast screening uptake among women with HIV. Ours is not the first study to report this finding.11 Previous studies in women with HIV have found that, compared with screening rates in Latina women, rates are lower among women of black and white ethnicity7 but higher among immigrants than among non-immigrants and higher among women who have not completed high school than among those who have.25 Our findings highlight the role of model of care delivery in screening mammography. Women who had regular primary care, either with or without regular HIV specialist care, were more likely to receive mammograms compared with those without regular care or those with only HIV specialist care. A previous comparison of generalists versus specialist physicians did not find a difference in mammography screening between specialty groups.9 However, our finding is consistent with our earlier work indicating that cancer screening was more common among people with HIV who had a usual family physician12 and studies among women in the general population, which support the view that continuity of care with a usual family physician is critical to meeting breast screening recommendations.25,26
Limitations
Our study is strengthened by its population-based nature, which allowed us to comprehensively evaluate breast cancer screening in Ontario. Furthermore, physician care and mammography are universally covered for Ontario residents, mitigating the potential effect of disparities in health insurance.27 However, our study has limitations. First, we did not have access to laboratory data, such as CD4 cell count and viral load, although immune status has not been found to be associated with breast cancer screening in other studies.7,28 Second, characteristics such as socioeconomic status were assigned at the neighbourhood rather than at the individual level. Third, we did not have information about HIV transmission group, such as heterosexual or injection drug use transmission, which may influence access to and engagement with preventive care. Fourth, we could not identify women with HIV who were unaware of their status or who had not linked to care; we hypothesize that mammography screening would be even lower among these populations. Fifth, we lacked data on organizational features that may influence screening, including electronic decision support tools,28,29 practice size28 and co-location of screening services.22 Finally, with only 623 screen-eligible women with HIV, our study may have been under-powered to detect associations in the secondary analysis.
Conclusion
Our study builds upon previous findings of lower prevalence of breast cancer screening among women with HIV. We have also demonstrated that regular care, especially care provided by a usual family physician, is associated with improved uptake of mammography among these women. Strategies such as co-location of preventive services,10 patient letters, reminder phone calls and educational materials have been shown in studies of women without HIV to improve screening uptake, and they warrant evaluation in women with HIV.26,29,30 Reminder letters for breast cancer screening are sent to patients in Ontario, and it is unclear why there is differential uptake among women with and without HIV. Physician-directed interventions may be required, as physicians may emphasize the provision of HIV-specific primary care services to the detriment of routine, non-HIV-specific health screening, such as mammography.12,31,32 This phenomenon may be related in part to the time constraints associated with the management of HIV and associated comorbidities.33,34 These findings have implications for HIV care practice and policy, which must increasingly encompass the prevention and management of comorbidities across the lifespan and requires communication and integration across primary and specialist care.33,35
Supplemental information
For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/5/3/E673/suppl/DC1.
Footnotes
Competing interests: None declared.
Contributors: All authors contributed substantially to the conception and design of the study, or the acquisition of the data, or the analysis and interpretation of the data. All authors drafted the article or revised it critically for important intellectual content, and gave final approval of the version to be published. All authors agree to act as guarantors of the work.
Funding: This study was funded by the Canadian Institutes of Health Research (CIHR). Claire Kendall and Tony Antoniou are supported by New Investigator Awards from CIHR - Ontario HIV Treatment Network (OHTN). Janet Raboud is supported by an Ontario HIV Treatment Network Chair in Biostatistics. Sharon Walmsley is supported by a research chair from the Ontario HIV Treatment Network. Ann Burchell is supported by a CIHR New Investigator Award.
Disclaimer: This study was supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred. Parts of this material are based on data and information compiled and provided by Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions and statements expressed herein are those of the authors and not necessarily those of CIHI.
References
- Copyright 2017, Joule Inc. or its licensors
In this issue

{kind=link}
Article tools





