


Abstract
Background: For about 25 000 Ontarians living in remote northern First Nations communities, seeing a doctor in an emergency department requires flying in an airplane or helicopter. This study describes the demographic and epidemiologic characteristics of patients transported from these communities to access hospital-based emergency medical care.
Methods: In this cross-sectional descriptive study, we examined primary medical data on patient transportation from Ornge, the provincial medical air ambulance service provider, for 26 remote Nishnawbe Aski Nation communities in northern Ontario from 2012 to 2016. We described these transports using univariate descriptive statistics.
Results: Over the 5-year study period, 10 538 patients (mean 2107.6 per year) were transported by Ornge from the 26 communities. Transport incidence ranged from 9.2 to 9.5 per 100 on-reserve population per year. Women aged 65 years or more had the highest transport incidence (25.9 per 100). Girls aged 5–9 years had the lowest mean incidence (2.1 per 100). Gastrointestinal issues accounted for 13.3% of transfers. Neurologic issues, respiratory issues and trauma each accounted for about 11% of transfers, and cardiac issues for 9.6%. Patients with obstetric issues accounted for 7.6% of transfers per year, and toxicologic emergencies for 7.5%.
Interpretation: This study provides the epidemiologic foundation to improve emergency care and emergency transport from remote First Nation communities in Ontario.
Almost all residents of Ontario, Canada live within 30 minutes of an emergency department.1 However, for about 25 000 Ontarians living in remote communities, accessing a doctor in an emergency department requires flying in a plane or helicopter.1 Patients in these northern communities access medical care through a local nursing station, with intermittent in-community physician coverage. Patients with high-acuity conditions are transported from remote communities to hospital by Ornge, the provincial medical air ambulance service provider.2,3 Even under ideal conditions, these transfers take several hours. Air transports from these communities can face delays due to weather, visibility, mechanical issues and personnel issues. More than half of the associated remote airports do not have key visual aids that pilots use to land aircraft during periods of reduced visibility, which makes medical transports dependent on weather conditions.4
First Nations populations living in remote communities are known to face challenging social determinants of health: isolated geography, insufficient housing, unemployment, and the cultural impact of colonialism and residential schools.5 Access to potable water is an issue in many communities, with 188 boil water advisories in First Nations in the Sioux Lookout area between 2007 and 2016.6 These populations face trauma at rates 2.5–8 times greater than the Canadian average.7–10 People living in these communities face elevated rates of chronic disease, which manifest as critical health emergencies including mental health, infectious disease, diabetic and cardiovascular emergencies.11–14
The characteristics of patients requiring air medical transport in this region have not been well described, with only a handful of published papers describing medical emergencies in these remote communities over the last 35 years.2,6,7,15,16 We aimed to describe who is transported from 26 remote Nishnawbe Aski Nation communities in northern Ontario to access hospital-based emergency medical care and to describe the primary clinical reason for their transport as stated in the patient record. This study adds accessible information in a geographic region where health data are not readily available.
Methods
The objectives and methods of this cross-sectional descriptive study were developed in consultation and collaboration with the Nishnawbe Aski Nation, Sioux Lookout First Nations Health Authority and Weeneebayko Area Health Authority.
Setting
Nishnawbe Aski Nation represents 49 First Nations communities in northern Ontario,17 of which 26 are remote communities with no permanent, 4-season road access. This paper focuses on these 26 remote communities, with a total on-reserve population of about 22 400. Cat Lake is the closest of these communities to Sioux Lookout, about 180 km away by air; Fort Severn is the farthest, more than 700 km north of Sioux Lookout. Sioux Lookout is the location of the closest hospital for most of these remote communities.
Inclusion criteria and definitions
We examined all medical patient transports from remote Nishnawbe Aski Nation communities from Jan. 1, 2012, to Dec. 31, 2016. A patient transport was eligible for inclusion in the study if the community in question met all the following criteria: is part of Nishnawbe Aski Nation, is remote, has a landing strip or helicopter pad, has a nursing station or health centre, and does not have access to full-time, in-community physician services.
We defined a remote community as having no permanent, 4-season road access. These remote communities have access to an emergency department only by air or by winter road; people are unable to get in a vehicle and drive to access physician services. Twenty-six communities met the inclusion criteria (Figure 1).

Included remote Nishnawbe Aski Nation communities. Source: Indian Reserve (Shapefile). Peterborough (Ont.): Ontario Geospatial Data Exchange, Ministry of Natural Resources, 2008. Reproduced with permission.
Ornge patient transports from remote Ontario communities not associated with Nishnawbe Aski Nation were excluded, as were nonemergency, non-paramedic–supported medical transports on scheduled flights with commercial carriers. Patients who accessed care by driving on a winter ice road to access a hospital were excluded from the study. All emergent, paramedic-supported transfers were captured in the study.
Data sources
We accessed Ornge data through data-sharing agreements with all partner organizations and investigators. This database is owned and maintained by Ornge. For the purpose of this study, Patient Call Reports from Ornge were used. The Patient Call Report is a record of events relevant to a patient transfer request, including demographic characteristics, clinical information, physical examination findings, clinical treatments and procedures, and general administration sections. A Patient Call Report was completed for each patient by paramedics. The database was missing data for less than 1% of cells analyzed. It does not capture flight delay information.
For population data during the study period, we used on-reserve population from Indigenous and Northern Affairs Canada (Tim Leonard, Indigenous and Northern Affairs Canada, Ottawa, Ont.: personal communication, 2018). We grouped communities into 3 on-reserve population groupings (1–499, 500–1000 and > 1000) to assess whether community size was associated with the rate of emergency transfer. There were about an equal number of communities per grouping.
Statistical analysis
We examined the patient transport data through univariate descriptive statistics. We calculated the mean annual emergency transport incidence per 100 people on reserve, total transports by year, sex and age group, and incidence of transports by year, sex and age group. We also compared transport incidence stratified by community population. We computed mean annual transport rate ratios for each age group by sex using the 40- to 44-year-old group as the reference.
We analyzed the reason for transport as stated in the patient record. As patients were transferred from nursing stations, where minimal testing is available, they did not have a diagnosis but, rather, chief presenting problem. Ornge paramedics assigned patients a primary reason for transportation, and we grouped these into clinical subheadings according to their clinical domain. Transfers for primary mental health concerns were not identified or labelled as “mental health” in this data set. We captured patients who were transferred for a mental health crisis under another clinical subheading, such as neurologic, toxicologic or trauma. This issue is discussed further in the Limitations section of the paper.
Ethics approval
This project received research ethics board approval from the Sioux Lookout Meno Ya Win Health Centre, Weeneebayko Area Health Authority, Lakehead University, Laurentian University and the Sinai Health System.
Results
Between 2012 and 2016, the total on-reserve population of the 26 included communities increased from 21 488 to 23 257, with a mean of 22 389.0. During the same period, total emergency medical transports by Ornge from the communities increased from 2051 to 2145 (mean 2107.6 per year), for a total of 10 538 transports (Appendix 1, Supplemental Tables S1 and S2, available at www.cmajopen.ca/content/8/2/E400/suppl/DC1). Although the on-reserve population increased by 8.2% over the study period, the number of emergency medical transports increased by 4.6%, corresponding with a decreasing incidence of emergency transfer, from 9.5 to 9.2 per 100 on-reserve population.
Each year, 44.1% of people receiving emergency transportation were male, and 55.3% were female (Table 1). Among males, those aged 4 years or less, and those aged 65 years or more had the highest mean number of transports per year over the study period (164.8 and 140.8, respectively) (Table 1, Figure 2A). Similar peaks of mean total number of transports per year were observed for females (119.4 among those aged ≥ 4 yr, 159.0 among those aged ≥ 65 yr); however, the mean number of transports was also high for females aged 15–19 years (126.4) and 20–24 years (140.8).
Sex and age for on-reserve population and medical transports, 2012–2016
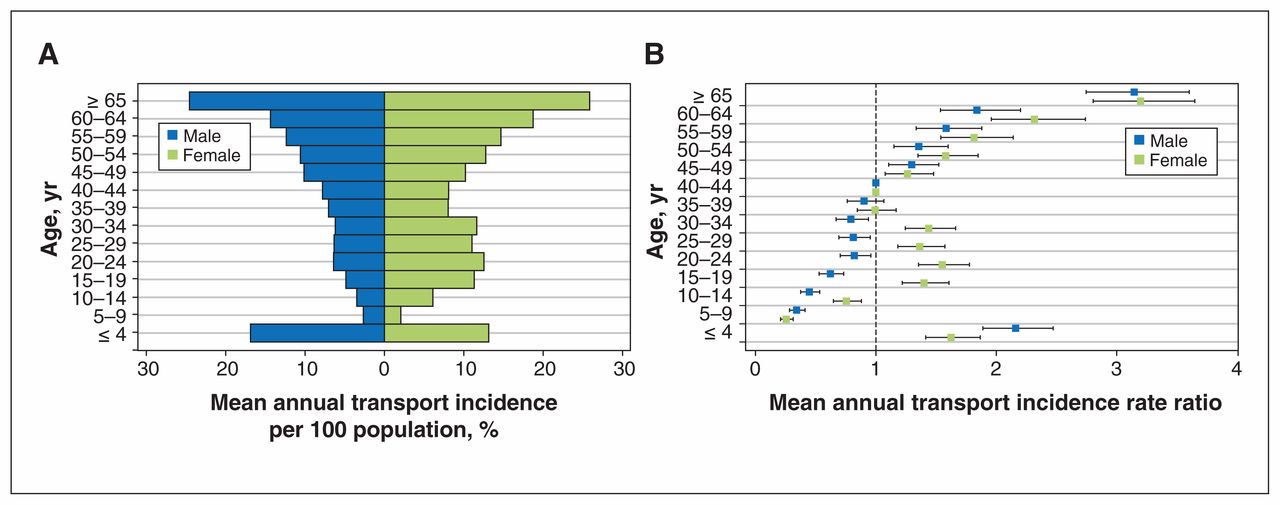
Mean annual transport incidence per 100 on-reserve population in the 26 communities (A) and mean annual transport incidence rate ratios (reference group age 40–44) (B). Error bars represent 95% confidence intervals.
There were 776 transports of children less than age 1 year, (mean 155.2 per year) (Appendix 1, Supplemental Table S3). Of the 776, 133 (mean 26.6 per year) involved babies less than 28 days of age. A total of 804 people aged 75 or more were transported (mean 160.8 transports per year); of the 804, 162 were older than 85 (mean 32.4 per year) (Appendix 1, Supplemental Table S3). Women more than 65 years had the highest incidence of emergency medical transport, with a mean annual rate of 25.9 transports per 100 on-reserve population (Figure 2A). Girls aged 5–9 years had the lowest rate of emergency transport, with a mean annual incidence of 2.1 per 100 on-reserve population.
Compared to the reference age group (40–44 yr), patients aged 65 or more had the highest mean annual transport incidence rate ratio (Figure 2B).
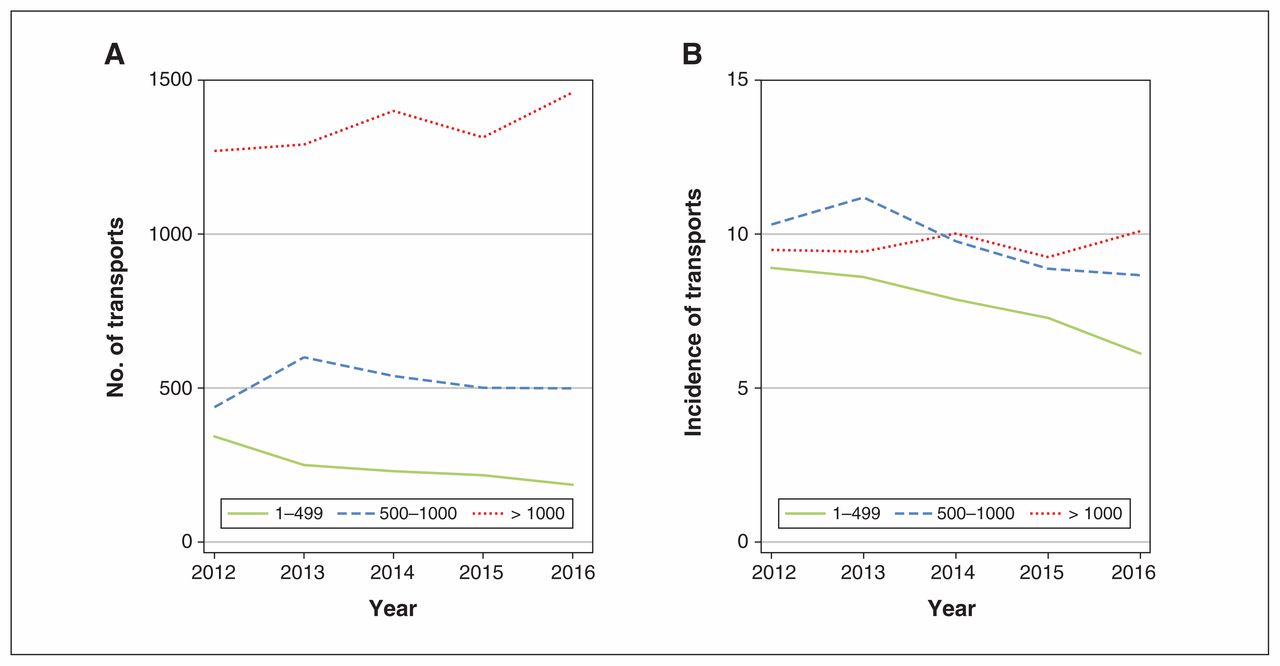
Across each of the 5 study years, the highest number of transfers came from the larger communities, with 60.3%–68.1% of all transfers initiated in communities with more than 1000 people (Table 2; Appendix 1, Supplemental Table S4). Although the total number of transfers was higher in the larger communities, the incidence was more stable across community population sizes (Figure 3). Over the study period, the lowest incidence of transfer was 6.1 per 100 on-reserve population, from communities with fewer than 500 people in 2016. The highest incidence of transfer was 11.2 per 100 on-reserve population, from communities with a population of 500–1000 in 2013. Although there was year-to-year variability in the incidence of transfer between medium-size and large communities, the incidence of transfer from communities with fewer than 500 people was consistently lower than that of other population strata.
Number of transports and incidence per 100 people, by community size and year
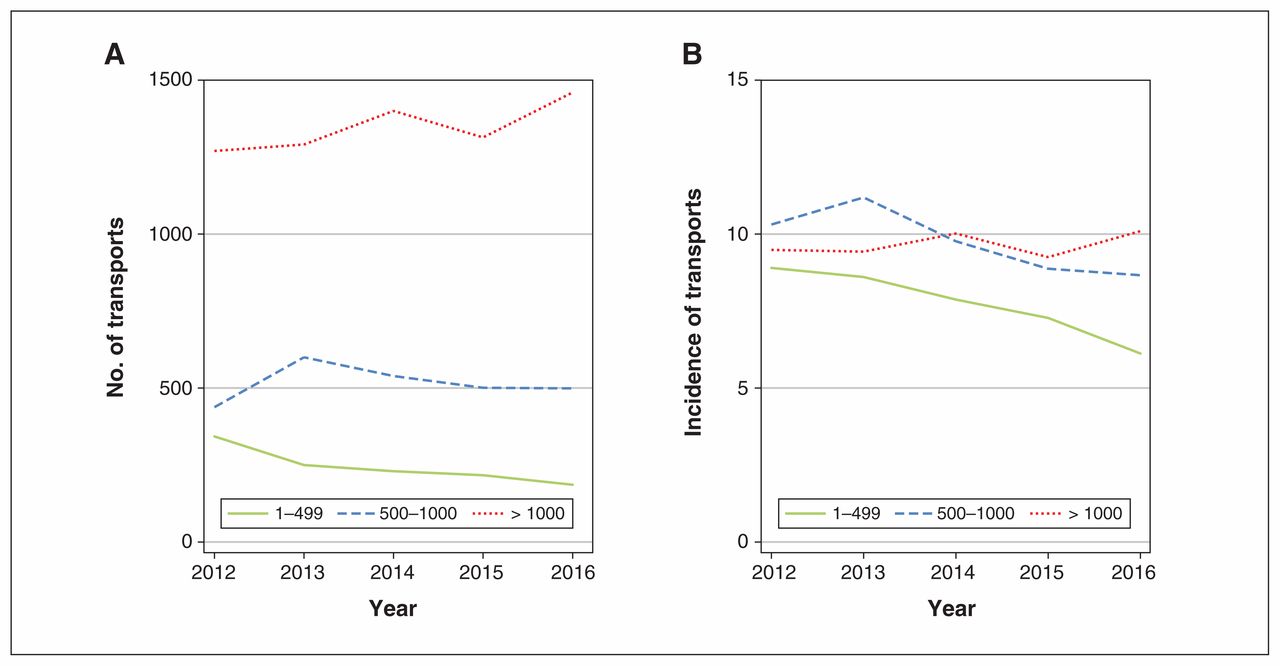
Number of patient transports by community size and year (A) and incidence of transports per 100 on-reserve population by community size and year (B).
The presenting reason for transport was left blank in 184 records (1.7%). The most common reasons for medical transport were consistent from year to year (Table 3). Gastrointestinal issues accounted for 13.3% of the total emergency transports, and cardiac issues for 9.6%. Patients with obstetric issues were transported on average 161.0 times per year and accounted for 7.6% of all transports. Toxicologic emergencies accounted for 7.5% of transports per year, and accidental and nonaccidental trauma accounted for 237.4 transports per year, or 11.3% of all transports. About 27% of transports were for presenting problems that individually accounted for less than 5% of all transports per year.
Number of transports by presenting problem, 2012–1016
The majority of patients were transported to the Sioux Lookout Meno Ya Win Health Centre (mean annual number of transports 1145.6, or 54.4% of all transports each year) (Appendix 1, Supplemental Table S5). Patients were flown to Moose Factory in 15.7% of cases, Thunder Bay in 12.9%, Winnipeg in 6.3% and to another accepting hospital in 10.7%.
Interpretation
This study provides an understanding of the burden of emergency medical problems in remote First Nations communities in northern Ontario and the volume of emergency air transports to access physician services. Our data suggest that First Nations people in these communities accessed physician services through Ornge at a rate of about 9 per 100 on-reserve population. There were 3 age peaks of total transports — less than 4 years, 65 years or more, and females aged 15–34 years — and the incidence of transport began to increase after age 50 years. Communities with an on-reserve population of fewer than 500 people had a lower incidence of transport for emergency medical care.
In 2014, about 1 028 000 patients in Ontario were transported by land ambulance, a rate of 7.5 per 100 population.18 Studies of interfacility transfer suggest that Ontario rural hospitals transfer patients to larger referral centres at a rate of about 1–3 per 100 population.19,20 Although one might interpret the Ornge transport rate as similar to provincial land ambulance or interfacility transfer numbers, these services are not comparable. In remote First Nations communities in northern Ontario, there is no 911 emergency telephone number or ambulance service. There is no option for people to self-present to an emergency department without boarding an aircraft. Patients who are transported by Ornge have been assessed by a nurse, who has discussed the case with a physician. When patients are transferred between facilities elsewhere in Canada, it is often for reasons such as computed tomography imaging, critical care, orthopedic care or pediatric care.19–21 For patients in this study, emergency air transfer was for their initial hospital assessment. Our data therefore underscore severe disparities in health care services and a high burden of emergency health conditions in remote First Nations.
The increased incidence of transport among young women may have been due to obstetric concerns. In 2016, First Nations in the Sioux Lookout area had a birth rate of 19.5 per 1000 population, compared to the provincial rate of 10.4 per 1000.6
The reason for the lower incidence of transport for emergency medical care from communities with an on-reserve population of fewer than 500 people is unclear and is most likely multifactorial. Paradoxically, larger communities often have more in-community physician coverage but also higher rates of transport, which suggests that local access to physician services may not independently reduce emergency patient transfers. Further study is needed to determine whether the presence of a local physician reduces emergency transfers in remote communities.
Canada-wide, the top 3 reasons for an emergency department visit are abdominal or pelvic pain, chest or throat pain, and respiratory problems.22 In the Sioux Lookout Meno Ya Win Health Centre emergency department, the centre that evaluated 54.4% of the patients transferred in this study, the top 4 reasons for emergency department visits are follow-up examination, respiratory problems, mental health and addiction issues, and abdominal and pelvic problems.2 In comparison, the top 3 chief reasons for air transport from remote communities in northern Ontario in our study were gastrointestinal issues, trauma and neurologic issues.
On average, 202.4 people per year were transported from First Nation communities for cardiac reasons. Could point-of-care testing in nursing stations reduce transfers for chest pain? Similar questions can be raised for each category of transport, leading to further areas of inquiry or innovation.
Future studies should target hospital-linked data to further understand these patients’ course to discharge and patient outcomes as these data sources become accessible. Prospective studies could examine changes in transport after implementation of interventions such as point-of-care testing, increased use of telemedicine and increased in-community imaging. Studies could also complete a cost analysis of Ornge patient transport. In addition, studies could examine remote Indigenous communities that have autonomous control over health care administration in their territory to learn whether administration differences affect emergency transfer patterns.
Limitations
We were unable to quantify the burden of emergency transports for mental health issues as these patients are categorized under another chief problem. Between 2012 and 2016, the rate of emergency department visits for mental health problems among First Nations youth in the Sioux Lookout area increased by 123%.6 In 2017, the region experienced a youth suicide rate of 2.7 per 1000, far higher than the provincial average.6 Data may be improved by developing methods to more clearly capture mental health cases.
Our data set does not follow patients as they move through the health care system; rather, it summarizes their transfer. Being able to connect this data set with hospital-linked data from ICES would be helpful to gain further details about the patient’s care and diagnoses on discharge from hospital. At the time of data analysis, this was not yet possible.
A further limitation in this study is balancing the data versus privacy. The research ethics board approvals outlined that this study can report only on collated data, not on any specific community-level data. Furthermore, when we accessed population data from Indigenous and Northern Affairs Canada, data for smaller age brackets were suppressed. Consequently, we used 65 years or more as an age category, as, in general, the community-level population data did not permit more specificity. Although the best population data available were accessed, there are limitations with these data. On-reserve population data are reliant on community reporting, which may lag behind true changes to population numbers as people move to and from remote reserves. In addition, with a quickly growing population, there may be delays in including births in the data set.
Conclusion
This study provides the epidemiologic foundation to enhance emergency care services in remote Indigenous communities in Ontario. There are limited publicly available data on the epidemiologic features of disease in remote First Nations in Ontario. The absence of data creates a compound marginalization: not only do communities face elevated health risks and decreased access to health care, they also lack the epidemiologic infrastructure to describe and address these issues. This study aims to aid in closing that gap. Understanding health emergencies in this region should improve the ability to plan services in these remote communities, which experience a disproportionate burden of disease and inequitable access to hospital-based emergency care.
Acknowledgements
The authors thank Julia Russell for support with administration, Mahvareh Ahghar for assistance with Ornge data, Jackson Beardy for support with community engagement and Adrien Marcotte for assistance with population data.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: David VanderBurgh, David Savage, Sacha Dubois, Homer Tien and Aaron Orkin acquired the data. David VanderBurgh, David Savage, Sacha Dubois and Aaron Orkin analyzed and interpreted the data and drafted the manuscript. All of the authors contributed to the study conception and design, revised the manuscript critically for important intellectual content, approved the final version to be published and agreed to be accountable for all aspects of the work.
Funding: This research was funded in part by a grant from the Northern Ontario Academic Medical Association.
Data sharing: Under the data-sharing agreement involving Ornge and Lakehead University, the data are not accessible to others.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/8/2/E400/suppl/DC1.
References
- Copyright 2020, Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools


