


Abstract
Background: The prevalence of metabolic syndrome is growing worldwide, yet remains underinvestigated in Canadian young adults. We sought to explore the use of a harmonized case definition specific to early-onset metabolic syndrome and determine its feasibility in assessing the prevalence of metabolic syndrome among electronic medical record (EMR) data of young adults in Northern Alberta.
Methods: We conducted a cross-sectional study using a sample of EMR data from young adult patients aged 18–40 years and residing in Northern Alberta, who had an encounter with a participating primary care clinic between June 29, 2015, and June 29, 2018. Physical examination, laboratory investigation and disease diagnosis data were collected. A case definition and algorithm were developed to assess the feasibility of identifying metabolic syndrome, including measures for body mass index (BMI), blood pressure (BP), dysglycemia, hypertriglyceridemia, high-density lipoprotein cholesterol, diabetes and hypertension.
Results: Among 15 766 young adults, the case definition suggested the prevalence of metabolic syndrome was 4.4%, 95% confidence interval (CI) 4.1%–4.7%. The most frequent 3-factor combination (41.6%, 95% CI 37.9%–45.3%) of metabolic syndrome criteria consisted of being overweight or obese, having elevated BP and hypertriglyceridemia. Half of metabolic syndrome cases (51.3%, 95% CI 47.6%–55.0%) were missing measures for fasting blood glucose, and one-fifth were missing a hemoglobin A1c (HbA1c) level. Notably, most young adults with a BMI of 25 or greater were missing HbA1c (68.7%, 95% CI 67.6%–69.8%), fasting blood glucose (84.0%, 95% CI 83.2%–84.8%) and triglyceride testing (79.0%, 95% CI 78.1%–79.9%).
Interpretation: We have shown that our case definition is feasible in identifying early-onset metabolic syndrome using EMR data; however, the degree of missing data limits the feasibility in assessing prevalence. Further investigation is required to validate this case definition for metabolic syndrome in the EMR data, which may involve comparing this definition to other validated metabolic syndrome case definitions.
Metabolic syndrome is a constellation of interconnected metabolic factors that contribute to the development of obesity, cardiovascular disease, type 2 diabetes and other related chronic conditions.1–3 The main components of metabolic syndrome are widely considered to be elevated blood pressure (BP), low high-density lipoprotein (HDL) cholesterol, hypertriglyceridemia, dysglycemia and excess visceral adiposity measured either by body mass index (BMI) or waist circumference.4 The pathogenic mechanisms of metabolic syndrome are thought to be driven by the presence of chronic low-grade inflammation associated with the development of insulin resistance and excess adiposity.5 The causes of metabolic syndrome are still under investigation and reviews have been published elsewhere.4,6,7
Since metabolic syndrome is typically more prevalent in older populations, its characterization in younger adult populations is less studied. Existing reports are either based on smaller cohorts of older adults, minority ethnic groups or overall population estimates based on self-reported data.8–10 Two Canadian-based studies using data from 2007 to 2009 showed that in populations aged 18–40 years, the prevalence estimates for early-onset metabolic syndrome were 6.5% and 7.8%, respectively.8,11 The lack of data on metabolic syndrome in younger populations is worrying, given that obesity and diabetes are rising in this population, with the highest growth of diabetes in Canada being in the gestational diabetes population.12 Furthermore, earlier identification and implementation of evidence-based interventions provide important opportunities to reduce the end-organ complications of metabolic syndrome, particularly in primary care. 13,14
Guidelines, such as those produced by Diabetes Canada and the Canadian Cardiovascular Society, encourage use of statins in individuals with diabetes who are older than 40, or in individuals with 15-year duration of disease who are older than 30.15,16 Understanding the burden of metabolic syndrome is important in preventing early-onset type 2 diabetes, given that an earlier diagnosis of type 2 diabetes has been shown to increase all-cause mortality.17
Challenges in consistently reporting estimates of metabolic syndrome prevalence are driven by the ambiguity of multiple validated case definitions created by different organizations.1,18–22 The most widely used criteria for identifying individuals with metabolic syndrome were published in the US National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP III) guideline.18 Moreover, the use of multiple definitions has created confusion for clinicians tasked with identifying and treating metabolic syndrome. Without clear definitions on who has metabolic syndrome, clinicians are not able to bring guidelines into action.
The main objectives of this study were to explore the use of a harmonized case definition for metabolic syndrome specific to early-onset metabolic syndrome and determine the feasibility of using such a definition in young adult patients in Northern Alberta who were included within the Northern Alberta Primary Care Research Network (NAPCReN) primary care electronic medical record (EMR) data.
Methods
Design
This was a cross-sectional study evaluating the most recent encounter for BMI, BP, laboratory investigations and disease diagnosis data to ascertain the feasibility of assessing prevalence of metabolic syndrome in a sample of primary care practices.
Setting and data source
The data provided for this research are NAPCReN regional data, a Northern Alberta subset of the Alberta primary care practice population, which contributes data to the Canadian Primary Care Sentinel Surveillance Network (CPCSSN).23 The EMR data are representative of 18 active clinics including 77 participating primary care clinicians across Northern Alberta representing 91 525 patients.24 The data do not include those seeking care from a clinic outside of NAPCReN, such as non-NAPCReN primary care, and secondary, tertiary and hospital care settings. Consenting family physicians and primary care clinicians provide NAPCReN with access to their EMR data.
We collected information on patient demographic characteristics, physical examination and laboratory investigations, as well as data for CPCSSN case definitions for diagnosis of disease. Physical examination data included BMI, systolic BP and diastolic BP. The laboratory data included HDL cholesterol, hemoglobin A1c (HbA1c), fasting blood glucose (FBG) and triglycerides.
Participants
The population denominator included all living people between the ages of 18 and 40 years, who had an encounter with a participating NAPCReN primary care clinic between June 29, 2015, and June 29, 2018, with an entry for sex and a valid Alberta postal code.
Measures
We developed a harmonized case definition using criteria based on the National Cholesterol Education Program Adult Treatment Panel III,18 the World Health Organization, 25 Diabetes Canada,21 Canadian Cardiovascular Harmonized National Guidelines Endeavour (C-CHANGE)15 and validated CPCSSN disease definitions.26 As outlined in Table 1, a patient was classified as having metabolic syndrome if they met a minimum of 3 out of 5 criteria. We used BMI given that 98.5% of individuals included in these data did not have measures for waist circumference and there is reasonable evidence to consider BMI where waist circumference data are unavailable.27 We used a BMI value of 25 or greater and did not distinguish between those in overweight or obese categories.18 Exclusion of outliers was based on expert clinical judgment (R.O.Y. and D.P.M) for BMI less than 15 and greater than 55.
Harmonized criteria for defining metabolic syndrome: 3 or more factors to make a diagnosis
Dysglycemia was present if a patient had a validated CPCSSN diagnosis of diabetes26 or an HbA1c level of 6.0% or greater or an FBG value of 5.6 mmol/L or greater.21 A diagnosis of diabetes was identified through an International Classification of Diseases, 9th Revision (ICD-9) code of 250 in the billing or problem list, antidiabetic medications or a previous laboratory value of elevated HbA1c or FBG; the CPCSSN case definition has a sensitivity of 95.6% (95% confidence interval [CI] 93.4%–97.9%) and specificity of 97.1% (95% CI 96.3–97.9).26
We used the validated CPCSSN case definition for diagnosis of hypertension, which has a sensitivity of 84.9% (95% CI 82.6%–87.1%) and a specificity of 93.5% (95% CI 92.0%–95.1%),26 or an office systolic BP or diastolic BP measurement to establish the presence of elevated BP. Based on clinical judgment (R.O.Y. and D.P.M.), we removed outliers for office BP measurements outside the range of 60–300 mm Hg for systolic BP and 30–200 mm Hg for diastolic BP. We used medical billings, medications and the problem list from the EMR data to identify hypertension-related ICD-9 codes, in order to make the diagnosis of hypertension.26 Individuals with a BMI or BP outside the prespecified range were still included in the cohort for all other clinical measures.
To assess the presence of dyslipidemia, women were identified as having a low HDL cholesterol level at less than 1.3 mmol/L and men at less than 1.0 mmol/L. Hypertriglyceridemia was determined using a triglycerides cut-off point of 1.7 mmol/L or greater. Notably, our data did not distinguish whether measurement of triglycerides was fasting or random, but there is evidence that the use of nonfasting triglyceride measurement is acceptable for the purposes of identifying metabolic syndrome.28
Case-finding algorithm for metabolic syndrome
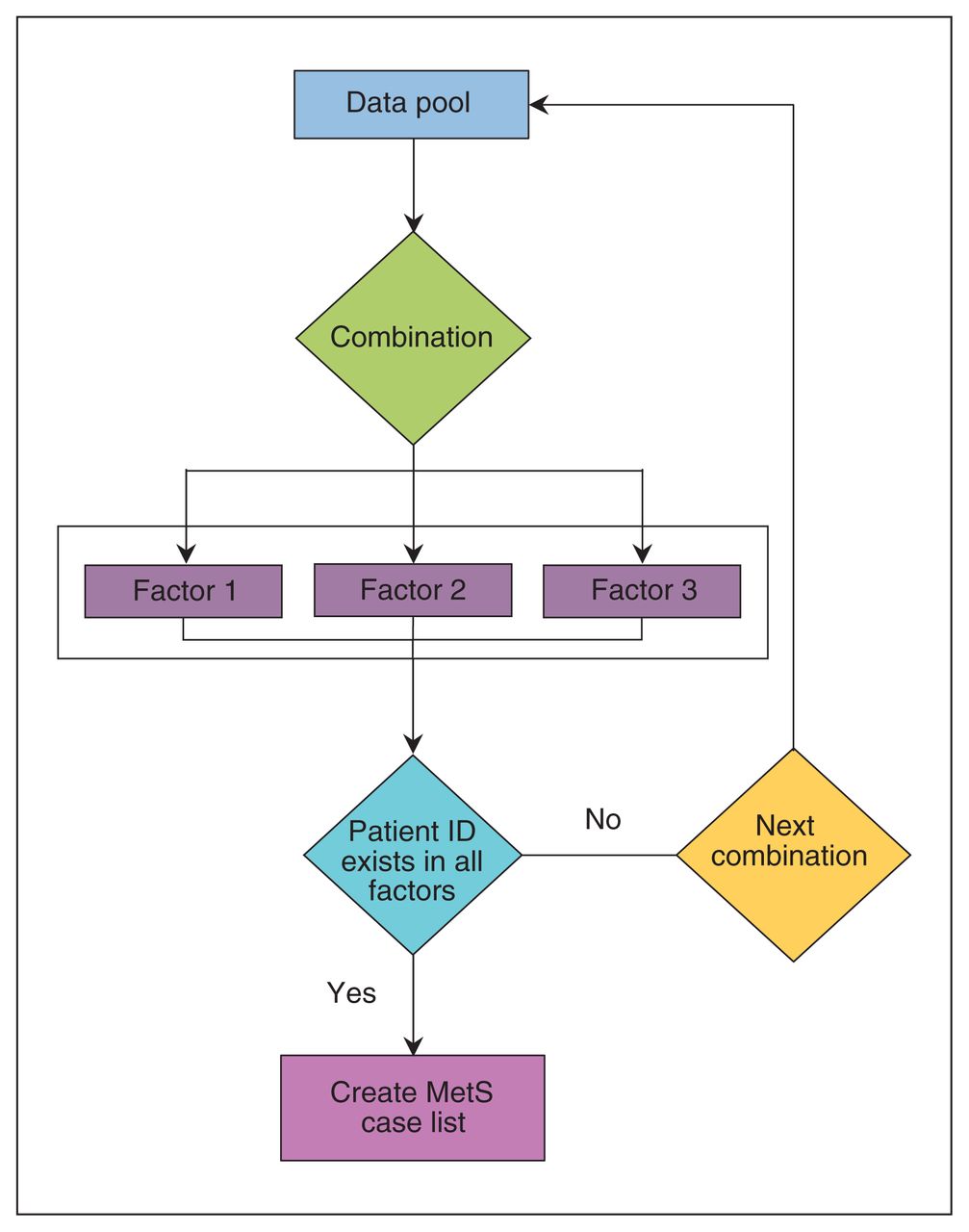
A case-finding algorithm was developed to ascertain prevalent cases of metabolic syndrome in patients who met a minimum of 3 of the 5 criteria listed in Table 1. The process of identifying metabolic syndrome cases in the algorithm (Figure 1) began with the first of 10 possible combinations. Each eligible patient within the sample was assessed for each combination. If a patient met the criteria for 3 factors for a given combination, they were identified as having metabolic syndrome. It is important to note that it was possible for a patient to have metabolic syndrome based on more than 1 combination, and that a patient was counted only once in establishing the prevalence, regardless of the number of combinations met.

Case-finding algorithm for detecting cases of metabolic syndrome (MetS). All patients within this data set are assessed using the 10 possible combinations based on the case definition outlined in Table 1. Each combination consists of 3 factors. An individual is counted as having MetS only once despite the possibility for meeting the criteria in multiple combinations.
Statistical analysis
Statistical analysis was conducted using R language for data manipulation, univariate and bivariate analysis, and case-finding algorithm development with RStudio version 1.1.453. A descriptive analysis was performed to describe the baseline sample characteristics on all variables, including age (calculated from year of birth), sex, disease status, BMI, BP, FBG, HbA1c, HDL and triglycerides measures. Continuous variables were reported as mean ± standard deviation (SD) or median and interquartile range (IQR). Categorical variables were expressed as counts with percentages. The prevalence of metabolic syndrome was defined as the ratio between those having metabolic syndrome and the total number of patients included in the denominator.
Ethics approval
This study was approved by the Health Research Ethics Board, University of Alberta (Pro. 00073600).
Results
A total of 15 766 individual records of patients aged 18 to 40 years were evaluated for the presence of metabolic syndrome. Of these, 260 were excluded because the records were missing an Alberta postal code or patient sex, or because the patient had died, and 6660 records were excluded because of duplicate and missing data (Figure 2). Baseline characteristics of the patients are shown in Table 2. Using our case-finding algorithm, we identified 700 participants with metabolic syndrome, corresponding to a prevalence of 4.4% (95% CI 4.1%–4.7%). The most common combination of 3 factors for diagnosing metabolic syndrome, representing 41.6% (95% CI 37.9%–45.3%) of those diagnosed, included measures of BMI, elevated BP and hypertriglyceridemia (Table 3).
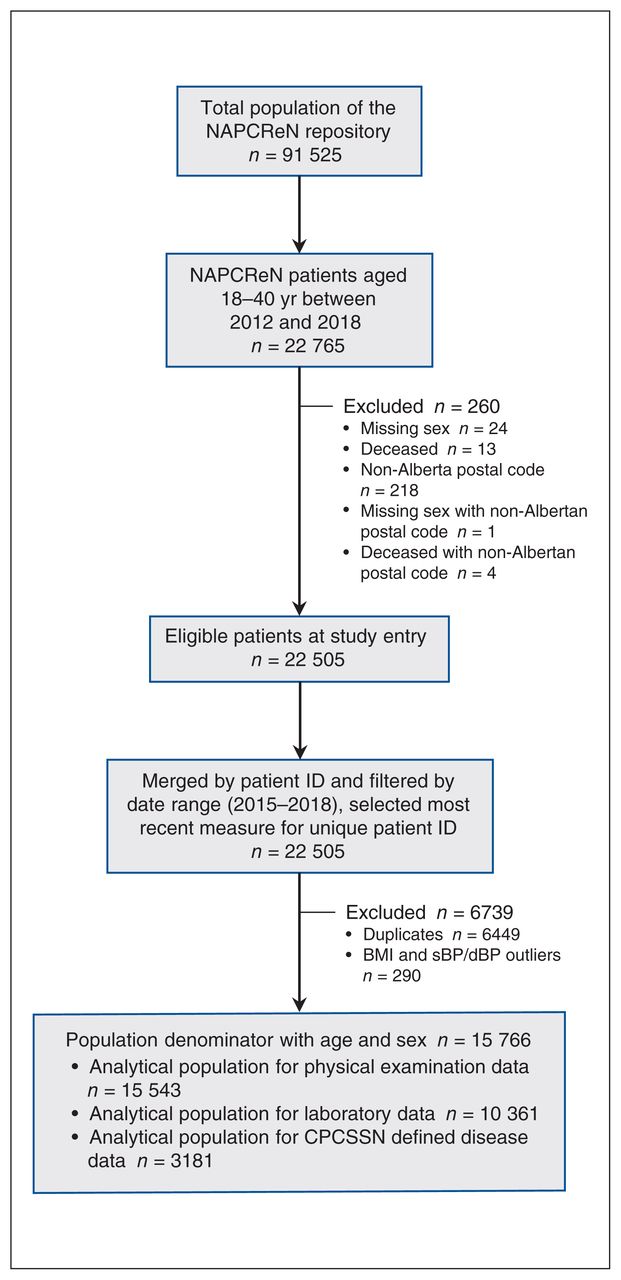
Flow of data extraction and cleaning from the NAPCReN-CPCSSN data repository. Note: BMI = body mass index, CPCSSN = Canadian Primary Care Sentinel Surveillance Network, dBP = diastolic blood pressure, NAPCReN = Northern Alberta Primary Care Research Network, sBP = systolic blood pressure.
Baseline characteristics of study sample stratified by presence of metabolic syndrome*
Prevalence of combinations meeting the minimum 3 factors for metabolic syndrome
Among physical examination measures, 90.6% (95% CI 88.4%–92.8%) of individuals in the metabolic syndrome group had a BMI of 25 or greater (Figure 3) and 71.3% (95% CI 67.9%–74.7%) had elevated office systolic BP and diastolic BP measurements. Dyslipidemia was more prominent in the metabolic syndrome group than in the non–metabolic syndrome group, with a greater presence of hypertriglyceridemia (70.1%, 95% CI 66.7%–73.5% v. 2.2%, 95% CI 2.0%–2.4%) and low HDL cholesterol (59.1%, 95% CI 55.5%–62.7% v. 2.3%, 95% CI 2.1%–2.5%). Of patients with metabolic syndrome, 45.9% (95% CI 42.2%–49.6%) had dysglycemia. Diabetes was higher in the metabolic syndrome group (15.1%, 95% CI 12.4%–17.8%) than in the non–metabolic syndrome group (0.8%, 95% CI 0.7%–0.9%), and hypertension was more prevalent among patients with metabolic syndrome than among patients in the non–metabolic syndrome group (14.1%, 95% CI 11.5%–16.7% v. 1.6%, 95% CI 1.4%–1.8%).

Percentages of participants with and without metabolic syndrome (MetS) who have specific risk factors and diseases. The proportion of participants achieving MetS component cut-off points with and without MetS is numerically represented in parenthesis. Error bars indicate 95% confidence interval. Note: BP = blood pressure, HDL-C = high-density lipoprotein cholesterol.
Overall, individuals within the metabolic syndrome group had higher mean values for BMI, FBG, HbA1C, triglycerides and lower HDL cholesterol than the non–metabolic syndrome group (Table 2). Regarding outliers in this data, including values beyond cut-off points for outliers yielded little effect on the mean values and interpretation for BMI and BP and, therefore, remained excluded from the data.
Missing data
In those with metabolic syndrome, 51.3% (95% CI 47.6%–55.0%) were missing an FBG measurement and 22.4% (95% CI 19.3%–25.5%) were missing measurements for HbA1c. Regarding measures of dyslipidemia and hypertriglyceridemia, 13.9% (95% CI 11.3%–16.5%) were missing laboratory investigations for HDL cholesterol and 10.3% (95% CI 8%–12.6%) were missing investigations for triglycerides. Physical examination data were measured more frequently in this group, as only 7.9% (95% CI 5.9%–9.9%) were missing BMI and 3.9% (95% CI 2.5%–5.3%) were missing an office BP reading (Figure 4A).

Distributions of missing data in (A) those with metabolic syndrome and (B) those with a BMI ≥ 25. Panel A shows the percent missing of MetS factors among those with MetS. Panel B shows the percent missing of MetS factors among those who are overweight or obese (BMI ≥ 25) regardless of MetS status. The proportion of missing data among those with MetS (panel A) or those who are overweight or obese (panel B) is numerically presented in parentheses. Error bars indicate 95% confidence interval. Note: BMI = body mass index, FBG = fasting blood glucose, HbA1c = hemoglobin A1c, HDL = high-density lipoprotein, MetS = metabolic syndrome, sBP/dBP = systolic/diastolic blood pressure, TG = triglycerides.
Within the overall sample of young adults aged 18–40 years, 24.9% (95% CI 24.2%–25.6%) were missing a BMI measurement. Moreover, among those who were missing a BMI measurement, 67.5% (95% CI 66.0%–69.0%) met 2 factors for metabolic syndrome and, therefore, would have been considered as having metabolic syndrome if they had a BMI over the 25 cut-off point. Notably, among all with a recorded BMI of 25 or greater (n = 7193), most were missing measures for FBG (84.0%, 95% CI 83.2%–84.8%), HDL cholesterol (80.3%, 95% CI 79.4%–81.2%), triglycerides (79.0%, 95% CI 78.1%–79.9%) and HbA1c (68.7%, 95% CI 67.6%–69.8%; Figure 4B). Lastly, the degree of missing data appeared to be attenuated among individuals as the number of metabolic syndrome factors increased (Figure 5).

Degree of missing data on physical examination and laboratory investigations among 0–5 factors for metabolic syndrome. Participants are numerically represented in parenthesis on the x-axis. Error bars indicate 95% confidence intervals. Note: BMI = body mass index, BP = blood pressure, FBG = fasting blood glucose, HbA1c = hemoglobin A1c, HDL = high-density lipoprotein, TG = triglycerides.
Interpretation
Using a case definition and case-finding algorithm for metabolic syndrome within the age group of 18–40 years, we found a potential prevalence of 4.4% of early-onset metabolic syndrome in Northern Alberta primary care EMR data. Importantly, we found a large proportion of missing data in this young adult sample, and we therefore suspect that our findings underestimate the true prevalence of metabolic syndrome. Young adult patients show lower rates of health care use and are more likely to forgo follow-up or not have a family physician, which could reduce the precision of our prevalence estimate.12,29 It is also difficult to know how missing data would potentially bias the true clinical prevalence given that in patients who underwent a physical examination or laboratory investigation, there was likely clinical suspicion to prompt these actions, and therefore, these patients may represent an enriched sample.30
Physical examination measures for BMI and BP were better recorded than laboratory measures for FBG, HbA1C and lipids, which may reflect clinical guidelines like the Alberta Screening and Prevention Program.31 Though BMI is readily captured in this EMR data, studies have shown the benefit of assessing central adiposity using waist circumference in definitions of metabolic syndrome.32,33
Given the feasibility of algorithmic identification of metabolic syndrome using our EMR data, this sparks the possibility of having point of care identification of these higher risk individuals during family practice visits, though the operationalization of such would require substantial consultation with primary care colleagues to avoid alert fatigue and to ensure appropriate steps for further screening and management.
The missing data among FBG, HbA1C and lipid measures illustrate current challenges in performing surveillance of young adult populations at risk for metabolic syndrome and chronic disease using routinely collected EMR data. The feasibility of the harmonized case definition developed illustrates metabolic syndrome in the young-adult sample; however, the degree of missing data affects the overall interpretation and findings of this study.
Despite the limitations to the feasibility of the case definition with this study’s EMR data, our findings suggest that the patterns of early-onset metabolic syndrome were similar to those of other studies evaluating older populations.10,34 Although there may be an age-dependent increase in the prevalence of metabolic syndrome, the distribution of metabolic syndrome features remains relatively the same, despite previous evidence of the physiologic differences in metabolic syndrome by age.35 The similarities in comparing the combinations from our study with another family practice–based study using a similar case definition for metabolic syndrome suggest that the patterns of metabolic syndrome manifestation remains similar irrespective of age (Table 3 and Appendix 1, available at www.cmajopen.ca/content/8/4/E779/suppl/DC1).
Canadian epidemiological investigations vary greatly in prevalence estimates for metabolic syndrome, with the estimates being between 2% and 13% in most studies and the most reliable estimates being 6.5% and 7.8% based on Canadian Health Measures Survey (CHMS) data.8,11 These findings reinforce the likelihood that our data underestimate the true prevalence of metabolic syndrome in the primary care setting, particularly given that the prevalence of obesity has only increased since those studies were conducted,36 and that the metabolic health of those seeking primary care are possibly worse than the population not seeking any medical care.30,37 It is also unsurprising that those meeting the definition for metabolic syndrome had elevated clinical physical examination and laboratory measurements; however, these measurements were important when comparing the data from this group to the data of those without metabolic syndrome.
Our data might suggest that the lack of clinical investigation for risk markers in young adults with metabolic syndrome or elevated BMI represents a lost opportunity for chronic disease prevention. This lack of investigation likely represents a combination of both patient and clinical inertia where patients may be less inclined to obtain laboratory testing while young and asymptomatic, and physicians might be less likely to order laboratory tests for the same reasons. There may also be considerable resource constraints given that 45% of young adults in this practice population had a BMI in the overweight or obese category. Physicians also report difficulties addressing metabolic syndrome among multiple definitions and recognize that identification of individual clinical risk factors is insufficient to address metabolic syndrome appropriately. 38 The causes of metabolic syndrome often involve broad social challenges requiring substantial resources that may lie outside the scope of conventional medicine or pose a challenge because of other conflicting clinical priorities in a patient’s care.39,40
The NAPCReN data are point-of-care EMR data allowing for a pragmatic understanding of the patterns of disease and the diagnostic gaps in the primary care setting. Using validated CPCSSN definitions for hypertension and diabetes in the case-finding for metabolic syndrome strengthens this study beyond the conventional measures for elevated BP and dysglycemia. Our harmonized case-finding algorithm for metabolic syndrome will further assist the CPCSSN network in validating a case definition for use in future surveillance, research and quality improvement projects.
Limitations
Major limitations of real-world data are insufficient clinical documentation and imperfect EMR data. In many instances, fields are missing information, data are incorrectly entered into the EMR, and patient demographic characteristics, such as home address and death, are not always reported if patients have moved out of province.41 We recognize that recording complete health information requires sufficient clinical reasoning and human resources and that measurements are affected by factors such as clinic workflow, professional judgment, recording behaviours of the provider, monetary incentives and design of the EMR. Moreover, negative findings are less likely to be reported, resulting in a selective nonreporting bias.42 We were also not able to assess health outcomes based on Indigenous status within these data. These limitations should be carefully considered when interpreting this study.
Conclusion
This cross-sectional study of real-world family practice data suggests that 1 out of every 25 people aged 18–40 years has metabolic syndrome. However, this is likely an underestimate because of the large proportions of missing data, driven by the subclinical nature of metabolic syndrome, the high prevalence of overweight and obese patients and the competing priorities of both patients and physicians. Further work is required to assess the feasibility of this case definition and to understand better whether missing data are clinically informed, rather than an omission because of lack of time or resources. These observations provide a basis for engaging primary care clinicians in considering the current recommendations for screening of young adults at higher risk of metabolic disease, and actions to earlier detection and management of metabolic syndrome and its associated morbidity.
Acknowledgements
The authors acknowledge the support of the Northern Alberta Primary Care Research Network, Mr. Brian Forst, Mrs. Allison Boileau and Mrs. Kimberly Derksen for their assistance with data access.
Footnotes
Competing interests: Jamie Boisvenue received studentship funding from the Alberta Diabetes Institute for the duration of this project. Roseanne Yeung reports grants from AstraZeneca, personal fees from Merck, personal fees from Novo Nordisk and personal fees from Sanofi, outside the submitted work. Carlo Oliva, Donna Manca and Jeffrey Johnson have no disclosures. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Jamie Boisvenue, Jeffrey Johnson, Donna Manca and Roseanne Yeung conceived and designed the study. Donna Manca provided the data. Jamie Boisvenue analyzed the data. Carlo Oliva provided programming and support of algorithm development. Jamie Boisvenue drafted the manuscript. All authors contributed to the revised manuscript for intellectual content. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Data sharing: The data from this study are held securely by the Northern Alberta Primary Care Research Network/Canadian Primary Care Sentinel Surveillance Network. A de-identified analysis data set from the study may be made available to other researchers who provide a detailed study proposal clearly describing the use of the data. The study proposal must also obtain approval from a research ethics board for this purpose. Proposals may be submitted up to 5 years after the date of publication of this paper. Researchers who wish to access the study data may contact the corresponding author, Jamie Boisvenue (boisvenu{at}ualberta.ca).
Funding: This study was supported by the Alberta Diabetes Institute and the Northern Alberta Primary Care Research Network.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/8/4/E779/suppl/DC1.
References
- Copyright 2020, Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools


