


Abstract
Background: As in other jurisdictions, the demographics of people infected with SARS-CoV-2 changed in Quebec over the course of the first COVID-19 pandemic wave, and affected those living in residential care facilities (RCFs) disproportionately. We evaluated the association between clinical characteristics and outcomes of hospitalized patients with COVID-19, comparing those did or did not live in RCFs.
Methods: We conducted a retrospective case series of all consecutive adults (≥ 18 yr) admitted to the Jewish General Hospital in Montréal with laboratory-confirmed SARS-CoV-2 infection from Mar. 4 to June 30, 2020, with in-hospital follow-up until Aug. 6, 2020. We collected patient demographics, comorbidities and outcomes (i.e., admission to the intensive care unit, mechanical ventilation and death) from medical and laboratory records and compared patients who did or did not live in public and private RCFs. We evaluated factors associated with the risk of in-hospital death with a Cox proportional hazard model.
Results: In total, 656 patients were hospitalized between March and June 2020, including 303 patients who lived in RCFs and 353 patients who did not. The mean age was 72.9 (standard deviation 18.3) years (range 21 to 106 yr); 349 (53.2%) were female and 118 (18.0%) were admitted to the intensive care unit. The overall mortality rate was 23.8% (156/656), but was higher among patients living in RCFs (36.6% [111/303]) compared with those not living in RCFs (12.7% [45/353]). Increased risk of death was associated with age 80 years and older (hazard ratio [HR] 2.39, 95% confidence interval [CI] 1.35–4.24), male sex (HR 1.74, 95% CI 1.25–2.41), the presence of 4 or more comorbidities (HR 2.01, 95% CI 1.18–3.42) and living in an RCF (HR 1.62, 95% CI 1.09–2.39).
Interpretation: During the first wave of the COVID-19 epidemic in Montréal, more than one-third of RCF residents hospitalized with SARS-CoV-2 infection died during hospitalization. Policies and practices that prevent future outbreaks of SARS-CoV-2 infection in this setting must be implemented to prevent high mortality in this vulnerable population.
Quebec was the epicentre of the COVID-19 health crisis in Canada between March and August 2020, accounting for more than half of Canada’s cases and deaths.1 As of Feb. 9, 2021, over 271 700 cases and 10 000 deaths attributed to COVID-19 occurred in Quebec, of which more than 50% of cases and 60% of deaths occurred in Montréal.1
The first case of COVID-19 in Quebec was diagnosed on Feb. 27, 2020, in an international traveller.2 Early transmission dynamics were driven by returning international travellers, many of whom were returning from school spring break.2,3 By mid-April, however, numerous outbreaks occurred in public and private residential care facilities (RCFs). The residents of these institutions bore the greatest burden of the first wave of the pandemic, accounting for 70% of the deaths in Canada and Quebec, with a case fatality rate estimated to be 36% (range 20% to 42%).2,4,5 Of the 59 845 patients with SARS-CoV-2 infection reported in Quebec between Mar. 1 and July 27, 2020, people living in RCFs represented a disproportionate burden of COVID-19, accounting for 23.4% of all patients, 43% of hospitalizations and 84.3% of deaths attributed to COVID-19.4
During the first wave of the pandemic, the incidence and mortality rates of COVID-19 peaked in Quebec in mid-May (> 1000 cases per day). After this peak, case numbers decreased to fewer than 150 cases per day from mid-June to mid-August 2020, in part because of travel restrictions, quarantining, physical distancing and masking.
To decrease the health burden of SARS-CoV-2 infection and protect the older adult population in the future, it is imperative that we learn from the experiences of the first wave. We sought to describe and evaluate the association between clinical characteristics and in-hospital outcomes (i.e., admission to the intensive care unit [ICU], mechanical ventilation and death) of patients with COVID-19 admitted to hospital in Montréal during the first wave of the pandemic, between March and June 2020, comparing those who did and did not live in RCFs.
Methods
Study design and setting
We conducted a retrospective case series of all patients with laboratory-confirmed SARS-CoV-2 infection who were hospitalized at the Jewish General Hospital from Mar. 4 to June 30, 2020, with in-hospital follow-up until Aug. 6, 2020. The Jewish General Hospital is a tertiary care hospital, in Montréal, Quebec. It was 1 of 2 adult hospitals initially designated to receive patients with COVID-19 in Quebec, and therefore received a large number of COVID-19 admissions.
Participants
We included all adults (≥ 18 yr) hospitalized at the Jewish General Hospital with a diagnosis of SARS-CoV-2 infection confirmed by a positive polymerase chain reaction test. Specimens obtained from the nasopharynx or lower respiratory tract were assessed with a polymerase chain reaction test that was developed and validated by the Quebec provincial laboratory, targeting the envelope gene (E-gene).
Data sources
We obtained retrospective data from the hospital electronic medical record and the laboratory system. These data included demographic data, past medical history (including medical comorbidities and medications), onset of and description of presenting symptoms, initial physical examination, initial laboratory data, clinical outcomes (ICU admission, mechanical ventilation and death) and disposition (death, discharged, still admitted). We collected data until Aug. 6, 2020, for patients who were still hospitalized. Two authors (medical residents, J.M. and A.L.) and several trained medical students collected data, and 2 authors (staff physicians, C.G. and L.Y.K.) and senior medical residents performed audits of the data abstracted by medical students to ensure reliability and accuracy of the data extraction.
The level of medical intervention and goals of care were established for each patient admitted to the hospital.6 Medical interventions are classified into 4 levels. Level 1 includes provision of all interventions offered by the medical team, including admission to the ICU, intubation and cardiopulmonary resuscitation (CPR). Level 2 has specific restrictions, that may include no CPR. Level 3 aims at treating reversible conditions, with directions for no transfer to ICU and no CPR. Level 4 focuses on palliative care. We collected the last level of medical intervention for each patient.
In Quebec, RCFs are classified as long-term care facilities providing 24-hour registered nurse coverage (centres d’hébergement et de soins de longue durée), where residents require more than 3 hours of nursing care per day;7 public institutions in which residents are semiautonomous and require up to 3 hours of nursing care per day (ressources intermédiare); and private facilities (résidences privées pour aînés), where older adults require care ranging from assistance with some activities of daily living to hours of nursing care.8,9 We defined patients living in public long-term care, public intermediate care or private residential care facilities before admission as RCF patients.
We included these descriptive variables and complications as they have been reported to be either associated with poor outcomes in several cases series or are important sequelae of SARS-CoV-2 infection.10–20 We defined acute kidney injury as an increase of 50% above the patient’s baseline creatinine or an increase of more than 26.5 μmol/L of the serum creatinine. We defined elevated hepatocellular enzymes as an elevation of aspartate transaminase or alanine transaminase above the upper limit of normal, and defined lymphopenia as an absolute lymphocyte count of less than 1.0 × 109/L. We considered hypoxemia as oxygen saturation less than 88% on room air or the need for supplemental oxygen, and considered tachypnea as a respiratory rate of more than 20 breaths per minute.19,21–23 We used the Berlin criteria to identify acute respiratory distress syndrome.24
Statistical analysis
We used descriptive statistics to summarize baseline demographic characteristics, clinical characteristics, laboratory values on admission, complications during hospitalization and disposition at the end of the study period. We present continuous variables as a mean and a standard deviation (SD) or a median and an interquartile range (IQR), as appropriate, and categorical variables as a total number and percentages. We used Kaplan–Meier curves and a log-rank test to describe differences in in-hospital survival up to 60 days among RCF and non-RCF patients.
We evaluated factors associated with in-hospital mortality with a Cox proportional hazard model using the date of admission to hospital as the beginning of follow-up time and the date of in-hospital death, hospital discharge or the end of the study observation (Aug. 6, 2020, for patients who were still admitted to hospital) as the censoring date, depending on which occurred first.
We used a multivariable Cox proportional hazard model to estimate adjusted hazard ratios (HRs) of in-hospital mortality for predictors of death, including age, sex, medical comorbidities and living in an RCF. We assessed the proportional hazard assumption with log-log survival curves and estimated Schoenfeld residuals for age groups, sex, number of medical comorbidities and residence in an RCF. In a sensitivity analysis, we modelled hospital discharge as a competing risk for death using the Fine and Gray method. All analyses were done in SAS, version 9.4.
Ethics approval
This study was approved by the CIUSSS West-Central Montréal Ethics Board.
Results
Between Mar. 4, 2020, and June 30, 2020, 656 patients with a laboratory-confirmed diagnosis of SARS-CoV-2 infection were admitted to the Jewish General Hospital, including 303 (46.2%) patients who were admitted from an RCF. The mean age of patients was 72.9 (SD 18.3) years (range 21 to 106 yr); 349 (53.2%) patients were female, and the median time of symptom onset before hospitalization was 6.0 (IQR 3.0–10.0) days. Baseline demographic and clinical characteristics are shown in Table 1. A total of 433 (66.0%) patients had 2 or more comorbidities, and the most common comorbidities were hypertension (n = 399, 60.9%), dementia (n = 209, 31.9%) and diabetes (n = 183, 27.9%).
Characteristics of patients admitted to hospital with SARS-CoV-2 infection at time of admission
The level of medical intervention status was level 3 or 4 in 286 (44.3%) people. Fever, cough or upper respiratory tract symptoms were present in 422 (64.3%) patients, and 112 (17.2%) patients had diarrhea as a presenting symptom. Most patients presented with tachypnea (n = 445, 70.3%). One-third of patients (n = 240, 36.8%) were hypoxemic and required supplemental oxygen at the time of admission. Lymphopenia at the time of admission was present in 296 (45.4%) patients. A total of 238 patients (36.3%) received both hydroxychloroquine and azithromycin after admission; this was routine practice at the hospital between Mar. 22 and Apr. 24, 2020, unless there was a prolonged QTc interval or another contraindication. A total of 177 (27.0%) patients received steroids, 9 patients (1.4%) received lopinavir or ritonavir and 8 patients (1.2%) received tocilizumab. A total of 118 (18.0%) patients were admitted to the ICU, 69 of whom were intubated.
Patients admitted from residential care facilities
Through the study period, the patient population characteristics changed, with an increase in older adults living in RCFs near the middle of the study period (Figure 1). Patients living in RCFs accounted for 46 (22.2%) of 207 admissions from Mar. 2 to Apr. 6, 248 (60.5%) of 410 admissions from Apr. 13 to May 18, and 8 (22.2%) of 36 admissions from May 25 to June 29. The mean age of all patients for each of these periods was 69.5 years, 75.2 years and 70.8 years, respectively. The demographics and clinical outcomes, stratified by RCF status, are presented in Table 2.
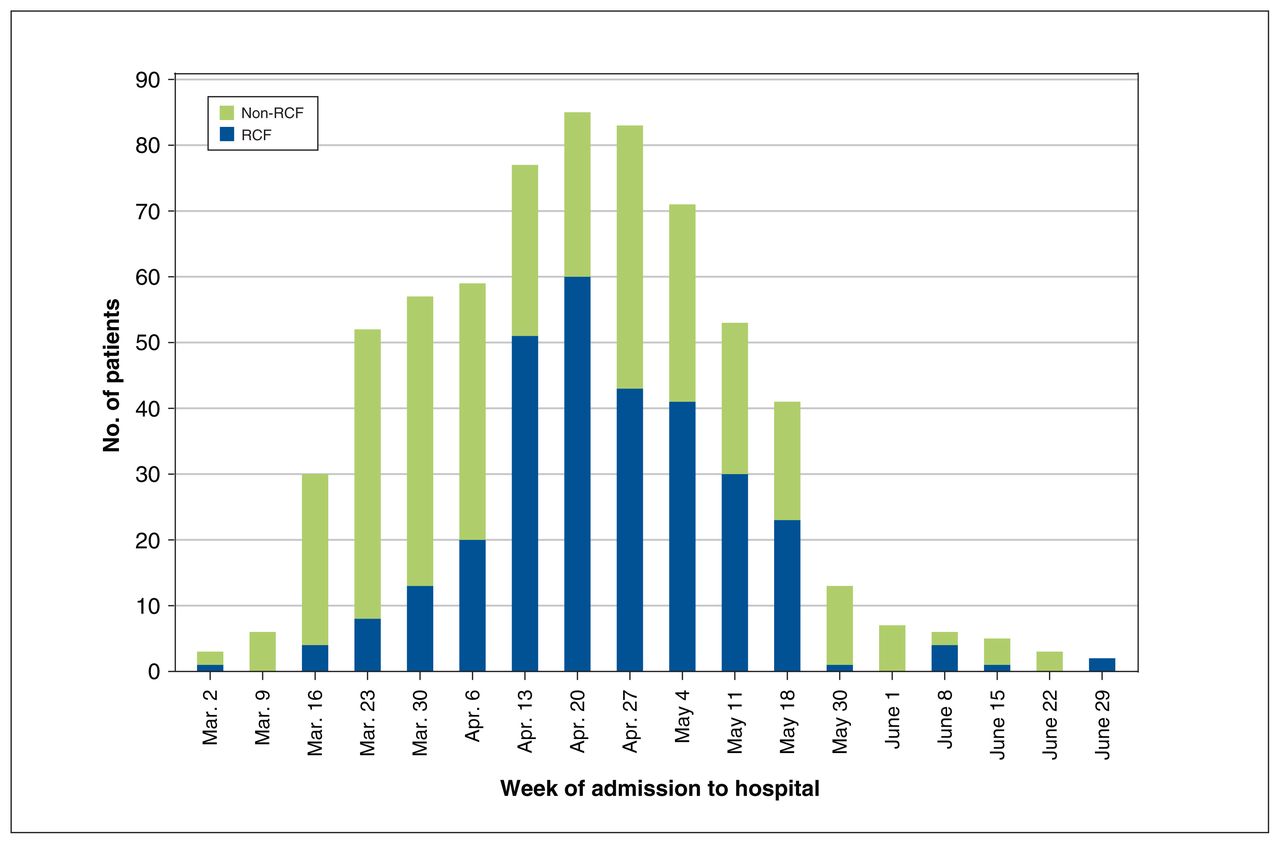
Number of patients admitted to Jewish General Hospital from Mar. 4 to June 30, 2020, by week, stratified by those living and not living in a residential care facility (RCF) before admission.
Characteristics and outcomes of patients admitted to hospital with SARS-CoV-2 infection, stratified by whether or not they live in residential care facilities
Compared with non-RCF patients, patients admitted from RCFs were older (mean 83.7 [SD 11.0] v. 63.7 [SD 18.3] yr), were more likely to be female (60.1% v. 47.3%), had a higher number of comorbidities (84.5% v. 50.2% with ≥ 2 comorbidities, and 40.3% v. 15.6% with ≥ 4 comorbidities) and were more likely to have dementia (62.0% v. 5.9%). Most patients from RCFs (74.0%) had a level of medical intervention status of 3 or 4. Fourteen (4.6%) patients from RCFs were admitted to the ICU for a median of 4.5 days (IQR 2.0–15.0); 3 (12.5%) were intubated.
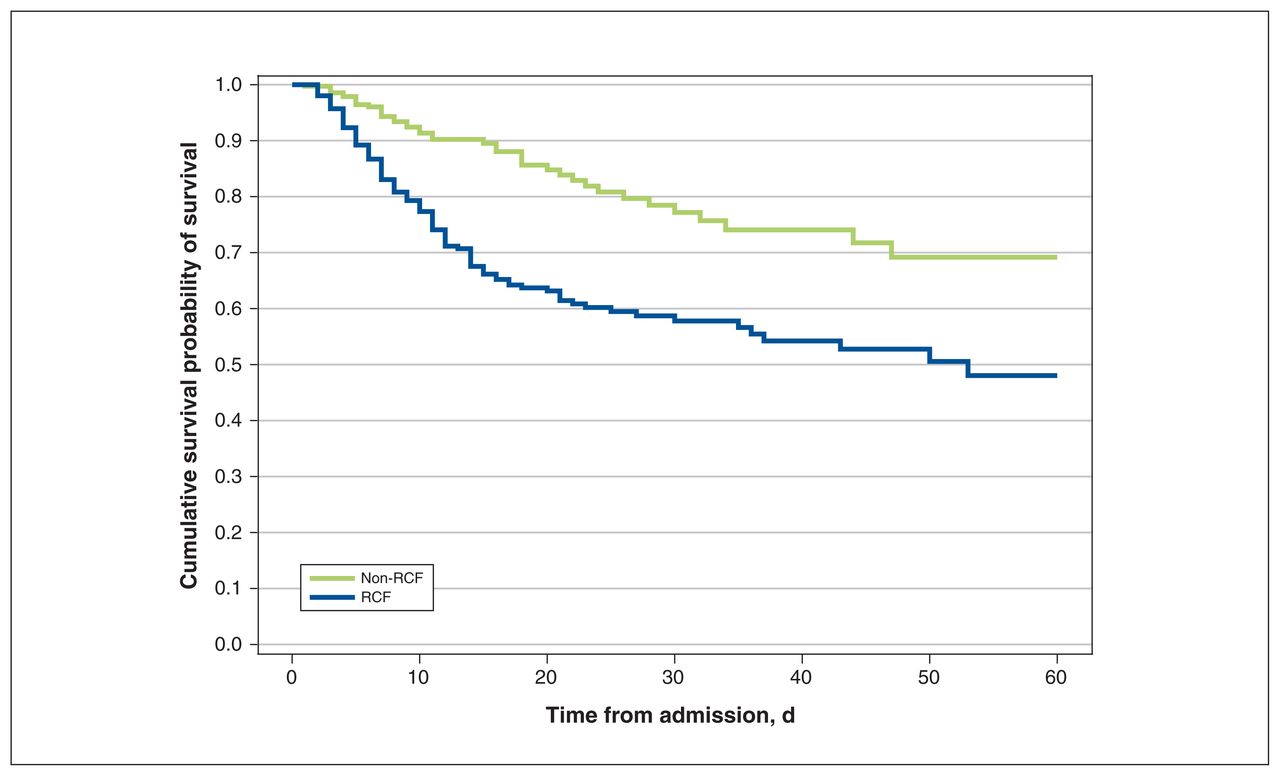
At the end of the study period, 111 (36.6%) of 303 patients from RCFs had died in hospital, compared with 45 (12.7%) of 353 non-RCF patients. The median length of hospital stay for patients from RCFs was 14 days (IQR 7.0–26.0), compared with 9 days (IQR 5.0–20.0) for non-RCF patients (Table 2). Patients from RCFs were more likely to die in hospital and died earlier than non-RCF patients, as shown in the Kaplan–Meier survival curves (Figure 2).
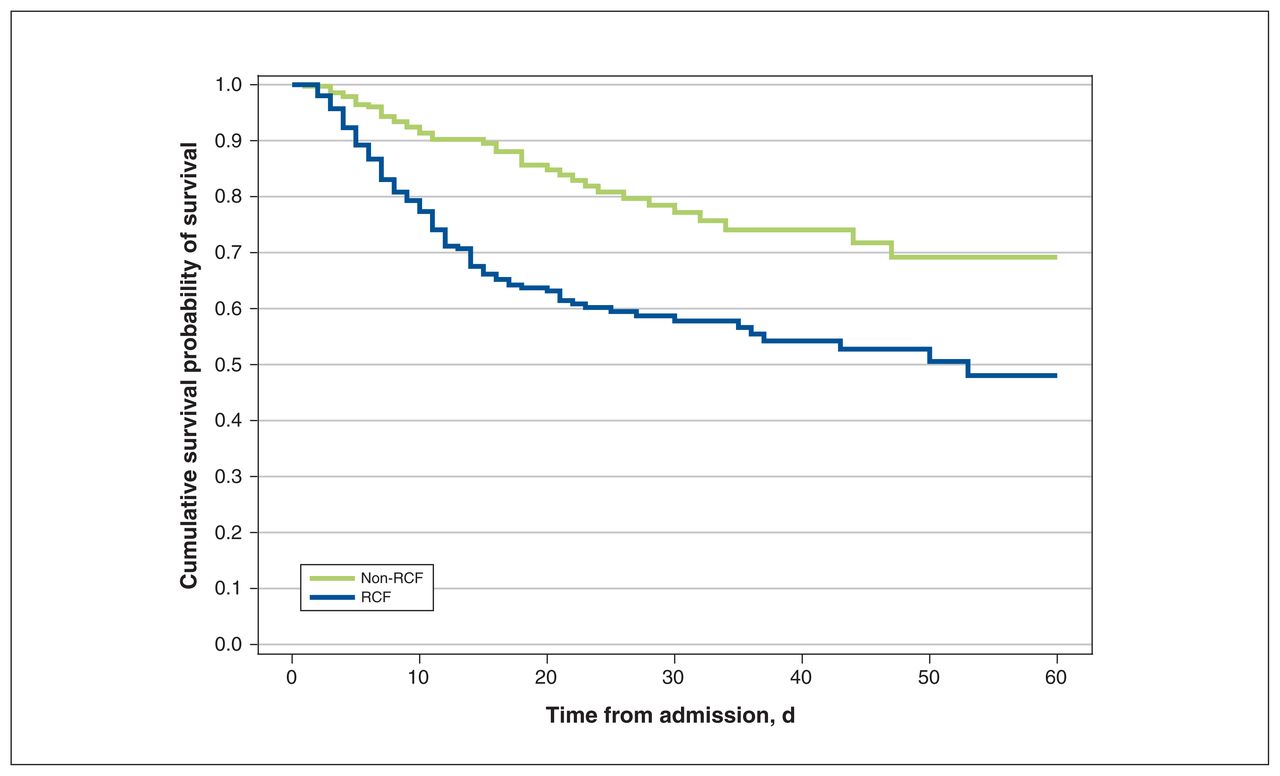
Kaplan–Meier curve of time to death after hospital admission of patients living and not living in a residential care facility (RCF) before admission. Log-rank test between RCF and non-RCF p < 0.0001.
Risk factors for in-hospital death
The characteristics and clinical outcomes of patients with COVID-19 by disposition (discharge or death) are shown in Table 3. Eight people (1.2%) were still admitted at the end of the study period; given the small numbers, they are not presented in Table 3. Of the 156 patients who died in hospital, most deaths (n = 139, 89.1%) occurred in people older than age 70 years, predominantly among those who were admitted from an RCF (n = 111, 71.2%), those with 2 or more (n = 135, 86.5%) or 4 or more medical comorbidities (n = 68, 43.6%) and patients with a level of intervention status of 3 or 4 (n = 132, 84.6%). The mortality rate among patients admitted to the ICU was 22.0% (26 of 118 patients), accounting for 26 (16.7%) of all 156 deaths.
Characteristics and outcomes of patients admitted to hospital with SARS-CoV-2 infection, stratified by disposition
In a multivariable Cox proportional hazard model, including age, sex, medical comorbidities and RCF status, the adjusted hazard of in-hospital mortality was increased for age 80 years and older compared with less than 70 years (HR 2.39, 95% confidence interval [CI] 1.35–4.24), male sex (HR 1.74, 95% CI 1.25–2.41), the presence of 4 or more compared with 0–1 comorbidities (HR 2.01, 95% CI 1.18–3.42) and living in an RCF (HR 1.62, 95% CI 1.09–2.39) (Table 4). In the models stratified by RCF status, only male sex was associated with death (HR 1.68, 95% CI 1.14–2.45) among patients living in RCFs, whereas age 80 years and older (HR 3.57, 95% CI 1.54–8.26), male sex (HR 1.98, 95% CI 1.05–3.75), and the presence of 2–3 (HR 3.01, 95% CI 1.10–8.22) or 4 or more comorbidities (HR 4.82, 95% CI 1.72–13.52) were associated with increased hazard of death among patients who did not live in RCFs (Appendix 1, available at www.cmajopen.ca/content/9/3/E718/suppl/DC1). Residents of public long-term care facilities had the highest adjusted hazards of death among patients from RCFs compared with those who did not live in RCFs (HR 1.94, 95% CI 1.26–299), although differences between the 3 RCF types were not statistically significant (Appendix 1, Table 2).
Crude and adjusted Cox proportional hazards models with risk factors for in-hospital death among patients admitted to hospital with SARS-CoV-2 infection
In a sensitivity analysis, we modelled hospital discharge as a competing risk for death using the Fine and Gray method. The HRs from this analysis (Appendix 1, Table 3) were not statistically different from those presented in Table 4.
Interpretation
We found that 36.6% of patients from RCFs who were hospitalized with COVID-19 died, compared with 12.7% of patients who did not live in these facilities. Older age, male sex, the presence of more medical comorbidities before hospital admission and being admitted from an RCF were associated with increased risk of in-hospital mortality. Patients from RCFs had a 62.0% higher risk of death compared with non-RCF patients after adjusting for age, sex and underlying morbidities, suggesting that they are a particularly vulnerable population.
Older adults living in long-term care facilities were substantially affected by COVID-19 during the first wave of the pandemic in Canada and Quebec, accounting for more than 70% of all deaths associated with COVID-19.4,5 The overall mortality rate among residents of long-term care facilities across Canada during the first wave is estimated to have been 36%, ranging from 20% to 40%.4,25 We found a similar mortality rate (36.6%) among hospitalized patients admitted from an RCF. Residents of long-term care facilities in Canada are older adults, with an average age of 82 years, who are predominantly female (65%) and have multiple comorbidities, particularly dementia (70%).25–28 The patients admitted to our hospital from RCFs had a similar profile.
The overall mortality rate in our study was 23.8%, similar to the 22% in-hospital mortality rate reported in the United States and Europe.12 We found that older age, male sex and multiple comorbidities were associated with in-hospital mortality. These factors have been previously described to be associated with increased risk of death among those infected with SARS-CoV-2.15,17,29–32 We also found that being a resident of an RCF was independently associated with in-hospital mortality after adjusting for age, sex and underlying comorbidities. This may be partially explained by the level of medical intervention status of 3 or 4 assigned to most patients from RCFs, likely as a result of age and multiple comorbidities. These patients were not eligible for CPR, admission to the ICU or mechanical ventilation. Only 14 (4.6%) of all 303 patients from RCFs were admitted to the ICU, and only 3 were intubated.
We did not formally measure frailty among the patients in our study, but it is likely that many of the patients from RCFs would have been classified as moderately to very severely frail, which could partly explain the increased mortality rate in this population. A large, observational, European study among patients admitted with SARS-CoV-2 infection found that those with clinical frailty scores of 5–6 (mild to moderate frailty) and 7–9 (severe frailty, very severe frailty and terminally ill) had an increased risk of in-hospital death (1.83 and 2.39, respectively), after adjusting for age, sex, diabetes, chronic renal disease and hypertension.33 We found that patients admitted from public long-term care facilities were the most likely to die in hospital, after adjusting for age, sex and underlying medical comorbidities. Those living in private residential facilities and public intermediate care facilities also had increased mortality, but this did not reach statistical significance. In a Quebec report that described all deaths (hospitalized and not hospitalized) associated with COVID-19 between March and July 2020, a similar pattern of risk of death was found among persons living in RCFs, with those living in public long-term care facilities being at greatest risk.4 In this report, residents of a public long-term care, public intermediate care and private care facilities had a 3.17, 1.72 and 1.47 increased odds of dying from COVID-19, respectively, compared with patients not living in an RCF, after adjusting for age, sex and medical comorbidities.4
The higher proportion of women in our study population (53.2%) reflects the high proportion of women (58.8%) in RCFs.28 Despite the greater number of women in our study, male sex was associated with higher in-hospital mortality rates among both patients who did and did not live in RCFs. The higher risk of severe COVID-19 among males is well described.31,32 These differences may be from sex-specific mechanisms modulating the course of disease, including increased expression of the viral entry receptor angiotensin-converting enzyme 2, the impact of sex hormones on receptor expression, or innate and adaptive immune responses and immunosenescence.31,32
Residential care facilities in Ontario and Quebec have been important centres of the COVID-19 epidemic in Canada, and in many other cities across North America.26,34,35 In Quebec, the crisis started in mid-April, where outbreaks in RCFs led to almost half of hospitalizations for COVID-19 and 83% of deaths from COVID-19 during the first wave of the pandemic.4 Widespread transmission of SARS-CoV-2 in RCFs was facilitated by chronic structural deficiencies in these institutions, including crowding, communal spaces, low staff-to-resident ratios, reliance on a precariously employed workforce that worked in several facilities and the lack of adequate personal protective equipment.25,36 This exacerbated the risk of infection among residents already at high risk for severe disease, given the presence of multiple comorbidities and frailty.25,36,37
After the first wave of the pandemic, the Quebec government published an action plan for the second wave that proposed to strengthen administrative teams within RCFs, improve communication with public authorities, recruit 10 000 new patient attendants, prohibit workforce mobility, ensure adequate testing, and improve infection and prevention measures.38 Residents of RCFs were also identified as a priority group for vaccination in Quebec.39 Despite these plans and efforts, outbreaks continued to occur in RCFs in Quebec during the second wave that started in September 2020. Residents of RCFs still accounted for a disproportionate number of deaths (n = 2892/4372, 66%) during the second wave of the pandemic (data as of Feb. 13, 2021).1
Limitations
Our study has several limitations common to retrospective studies using chart review. Characteristics such as obesity, frailty and ethnic origin are associated with severe COVID-19 outcomes, but were not reported in the medical chart and are not accounted for.17,33,40 These unmeasured confounders may potentially attenuate the hazard rate of mortality among patients living in RCFs. This is a single-centre study in Montréal, Canada, and may not be applicable to other jurisdictions.
Conclusion
We report a large case series of patients hospitalized with SARS-CoV-2 infection in Montréal, Canada, that showed a high mortality rate among residents living in RCFs despite admission to an acute care facility, attesting to the extreme vulnerability of this population. The pandemic has laid bare the need to reassess processes and policies in RCFs in Canada. People living in RCFs are at increased risk of death from COVID-19, and efforts must be put in place to protect this population.
Footnotes
Competing interests: Laurent Azoulay reports personal fees from Janssen and Pfizer, outside the submitted work. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Ling Yuan Kong and Christina Greenaway conceived the study, and Adam Palayew, Machelle Wilchesky, Laurent Azoulay and Christina Greenaway designed it. Jordan Mah, Anthony Lieu, Pouria Alipour, Ling Yuan Kong, Stephen Su Yang and Jed Lipes collected data, which Sunny Song, Adam Palayew and Marc Antoine Tutt-Guérette analyzed. Jordan Mah, Anthony Lieu, Mark Palayew and Christina Greenaway drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work. Jordan Mah and Anthony Lieu contributed equally to this manuscript.
Funding: Laurent Azoulay holds a Chercheur-Boursier Senior Award from the Fonds de Recherche du Québec - Santé and is the recipient of a William Dawson Scholar award from McGill University.
Data sharing: The data in this study cannot be shared with other researchers.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/9/3/E718/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2021 CMA Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.