


Abstract
Background: Risk factors for cause-specific mortality have not been widely studied among people with HIV infection. Our objectives were to estimate rates of and risk factors for all-cause and cause-specific mortality from 1995 to 2014 among HIV-infected people in Ontario.
Methods: We conducted a population-based retrospective cohort study using provincial health databases of people with HIV infection who were aged 16 years or more, were residents of Ontario between 1995 and 2014, and had HIV infection according to a previously validated algorithm. We used International Classification of Diseases codes to classify the underlying cause of death and estimated age-adjusted mortality rates per 100 person-years for 1995 to 2014. We used descriptive statistics to characterize the cohort at baseline and calculated adjusted mortality rate ratios (RRs) using generalized estimating equations.
Results: Among 23 043 people, the all-cause mortality rate declined from 6.69 to 1.53 per 100 person-years over the study period, and the rate of death from HIV/AIDS declined from 4.75 to 0.46 per 100 person-years. Concomitantly, the proportions of deaths due to cancer, cardiovascular disease and other noncommunicable diseases rose; however, rates remained constant or declined. Compared to males, females had higher mortality due to cardiovascular disease (adjusted RR 1.36, 95% confidence interval [CI] 1.04–1.77), noncommunicable causes (adjusted RR 1.75, 95% CI 1.39–2.20) and, by 2010–2014, any cause (adjusted RR 1.19, 95% CI 1.02–1.38). Residing in a low-income neighbourhood was associated with increased risk for most causes, including HIV/AIDS (adjusted RR in 2010–2014 1.86, 95% CI 1.49–2.31). Rural residence was associated with increased mortality due to malignant disease (adjusted RR 1.60, 95% CI 1.10–2.34) and noncommunicable disease (adjusted RR 1.86, 95% CI 1.25–2.77). Being an immigrant was associated with lower risk of death from all causes.
Interpretation: Over the study period, death was increasingly due to common chronic conditions rather than to HIV infection itself. Care should incorporate the prevention and management of these conditions, especially among females and those residing in rural and low-income areas.
The introduction of combination antiretroviral therapy (cART), in 1996, marked an important achievement toward prolonging the lifespan of people with HIV infection, resulting in shifting patterns in both mortality rates and leading causes of death in high-income countries. 1–3 In large cohorts in North America and Europe, allcause mortality declined, although it remains higher than among general populations.4–11 For example, the Antiretroviral Therapy Cohort Collaboration reported a nearly 40% reduction in crude rates from 1996–1999 to 2003–2005, with the greatest mortality attributed to AIDS-defining illnesses. 11 Among Antiretroviral Therapy Cohort Collaboration participants receiving long-standing treatment, most deaths were non–HIV-related.5 Among HIV-infected people in England and Wales, all-cause mortality declined by 69.7% between 1999 and 2008, with AIDS-related deaths accounting for 43% of all deaths.12 Similar declines in allcause mortality among people with HIV infection have been reported for British Columbia — from 3.88 to 2.15 deaths per 100 person-years between 2000 and 2012 — as well as a decrease in deaths due to HIV-related causes, from 2.34 to 0.56 per 100 person-years.7,8 Declines in rates of death from chronic liver disease (in particular due to hepatitis B and C), cardiovascular disease and suicide were also observed,7,8 which represents new trends in the primary causes of death in people with HIV infection.
Ontario is home to the largest number of HIV-infected people in Canada.13 Most new infections were acquired through sexual activity, such that mortality patterns may differ from those in British Columbia, where more infections were acquired via injection drug use.14 Antoniou and colleagues15 reported a decrease in all-cause mortality of 71.9% (from 5.7 to 1.6 per 100 person-years) in Ontario between 1996 and 2010 but did not report cause-specific mortality, which is critical to plan for prevention and delivery of health care services. As people with HIV infection age, many experience multiple chronic comorbidities,16 yet risk factors for cause-specific mortality have not been widely studied.10,17,18 Our objectives were to estimate rates of and risk factors for all-cause and cause-specific mortality from 1995 to 2014 among HIV-infected people in Ontario.
Methods
Study design
We conducted a population-based retrospective cohort study of people with HIV infection in Ontario using data held at ICES.
Data sources
The following administrative data sets were linked by means of unique encoded identifiers and were analyzed at ICES: the Registered Persons Database (an electronic registry of all Ontarians eligible for health coverage that captures patient demographic information), 2006 Statistics Canada census data (to link residential postal code to attribute the household income quintile as a proxy for socioeconomic status), the Ontario Health Insurance Plan database (contains physician billing claims for about 95% of visits), the Discharge Abstract Database (captures all hospital discharge data), the National Ambulatory Care Reporting System (contains emergency department and selected outpatient visits), the Immigration, Refugee and Citizenship Canada Permanent Resident database (includes the country of birth of immigrants who landed in Ontario beginning in 1986), the Ontario Cancer Registry and the Office of the Registrar General – Deaths Database (contains cause of death records).
Study population
Eligible people were aged 16 years or more, were residents of Ontario between Jan. 1, 1995, and Dec. 31, 2014, and had HIV infection according to a previously validated algorithm.19 This algorithm requires 3 physician claims coded for HIV infection (International Classification of Diseases, 9th revision [ICD-9] codes 042–044) over a 3-year period and has a sensitivity and specificity of 96.2% (95% confidence interval [CI] 95.2%–97.9%) and 99.6% (95% CI 99.1%–99.8%), respectively. 19 We excluded those who died before Jan. 1, 1995, those with missing age or sex, those who entered the cohort at age 15 years or less, those aged more than 105 years on Dec. 31, 2014, and those with no contact with the health care system after Jan. 1, 1995.
Outcomes
We ascertained all-cause and cause-specific mortality from 1995 to 2014. Follow-up began on the index date (Jan. 1, 1995) or the date of the first HIV billing codes that triggered the algorithm,19 whichever was later. We then followed patients until the earliest of death, loss to follow-up or Dec. 31, 2014. We considered loss to follow-up as having occurred if patients had no health care contacts for more than 7 years with no record of death. If patients had a gap of more than 7 years between health care interactions, they were censored from 7 years after the earlier interaction to the second interaction.
For cause-specific mortality, we used ICD-9 and ICD-10 codes to ascertain and rank the underlying cause of death: HIV/AIDS, other communicable disease, cardiovascular disease, malignant neoplasm, other noncommunicable disease, injury or missing/ill-defined (Supplementary Table A1, Appendix 1, available at www.cmajopen.ca/content/7/1/E1/suppl/DC1).
Variables
We examined potential risk factors for death: age (time-updated at midpoint of each calendar interval), sex (fixed covariate), calendar period (1995–1999, 2000–2004, 2005–2009, 2010–2014), urban/rural residence (i.e., major urban, non-major urban and rural, time updated at start of each calendar period), neighbourhood income quintile (time updated at start of each calendar period) and immigration status (i.e., immigrant from a country with a generalized HIV infection epidemic,20 immigrant from other country or long-term resident of Ontario) (fixed covariate).
Statistical analysis
We used descriptive statistics to characterize the cohort at baseline. We estimated age-adjusted all-cause and cause-specific mortality rates per 100 person-years using the 2011 Ontario population as the standard.21,22 We were unable to apply age and sex standardization to cause-specific rates owing to sparse age–sex cell sizes. We compared overall and cause-specific mortality by age, sex, calendar period, urban/rural residence, neighbourhood income quintile and immigration status. We conducted a complete-case analysis to estimate adjusted mortality rate ratios (RRs) with 95% CIs using generalized estimating equations with a log link and Poisson distribution, and compound symmetry covariance structure to account for the correlation among repeat observations within patients across time periods. We also tested interactions between calendar period and each covariate for overall and cause-specific mortality, and retained interactions terms if they were statistically significant at the p < 0.001 level. We centred age at 40 years and used this age as the reference group to facilitate interpretation for models with interactions with age and calendar period.
Ethics approval
Ethics approval was granted by the Sunnybrook Health Sciences Centre Research Ethics Board.
Results
Description of study population
Of the 24 525 people identified by the HIV algorithm, 23 043 met the inclusion criteria for our cohort (Table 1). Rural status was missing for 314 people (1.4%), and neighborhood income quintile was missing for 572 (2.5%). On average, at baseline, patients were 38 years old, and the greatest proportions were male (18 683 [81.1%]), lived in a major urban centre (20 625 [89.5%]) and in the lowest income quintile neighbourhoods (7165 [31.1%]), and were Canadian born or long-term residents (18 891 [82.0%]).
Characteristics of HIV-infected people at the start of follow-up, Ontario, 1995–2014
All-cause and cause-specific mortality
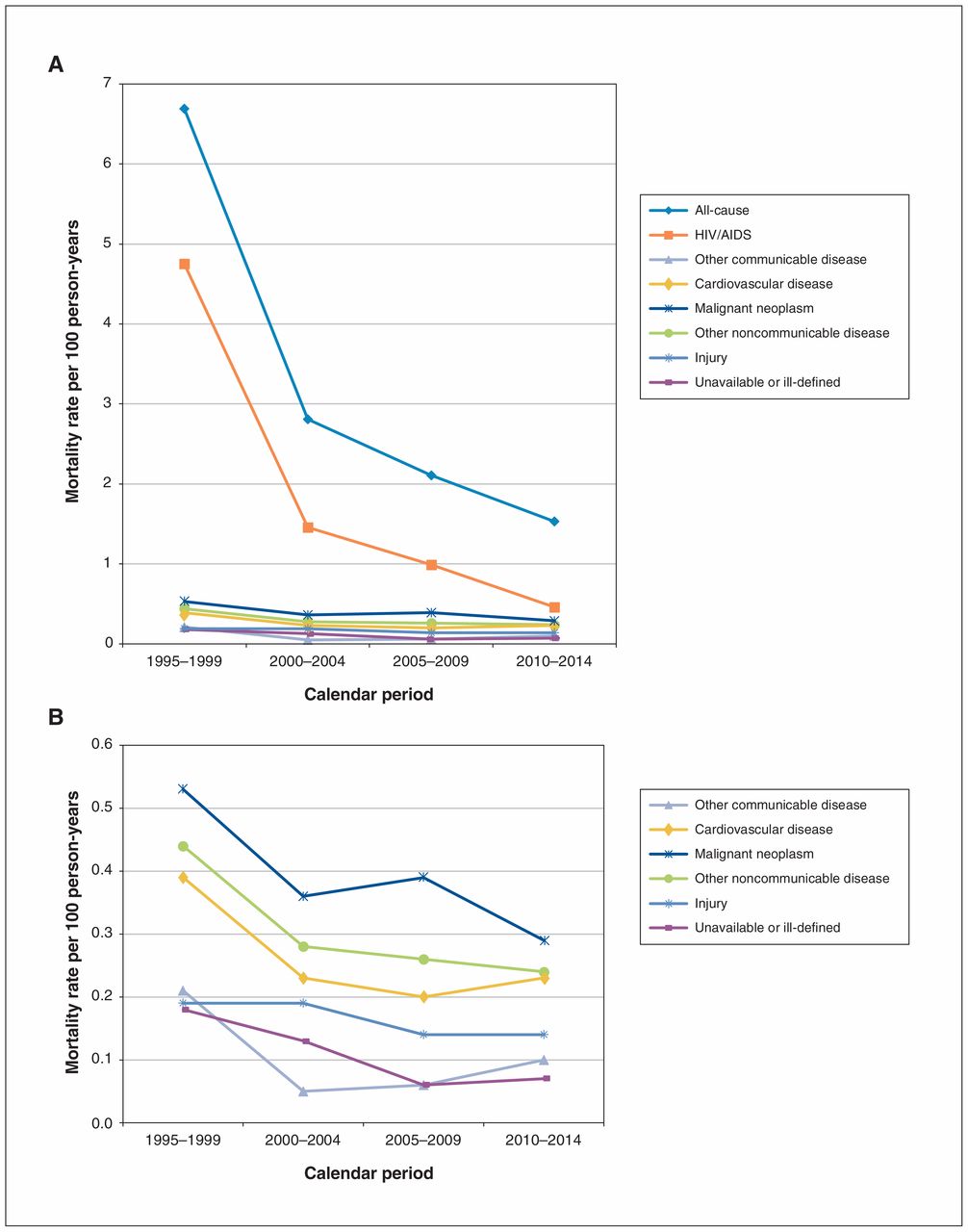
There were 5015 deaths over 221 601 person-years, for an overall crude mortality rate of 2.26 per 100 person-years. As expected, age-adjusted all-cause mortality rates decreased over the study period, from 6.69 per 100 person-years in 1995–1999 to 1.53 per 100 person-years in 2010–2014, a decline of 77.1% (Figure 1, Table 2).
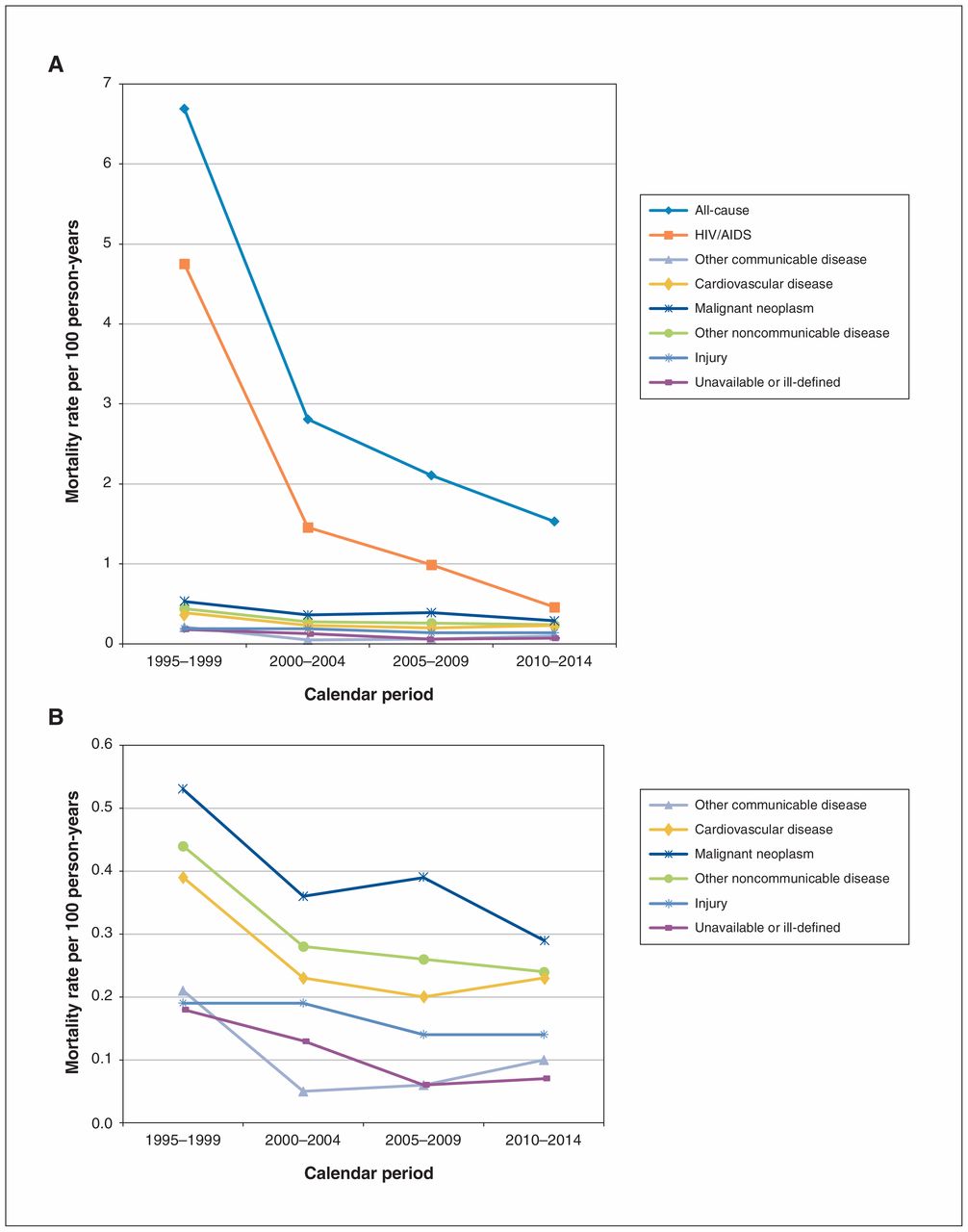
All-cause (A) and cause-specific (B) age-adjusted mortality rate per 100 person-years among HIV-infected people in Ontario, 1995–2014.
Age-adjusted all-cause and cause-specific mortality rates per 100 person-years among HIV-infected people in Ontario, 1995–2014
HIV/AIDS was the single most commonly recorded cause of death (Figure 1, Table 2). However, the pattern changed over time: the proportion of deaths attributed to HIV/AIDS decreased from 79.5% in 1995–1999 to 34.8% in 2010–2014. Concomitantly, the cause-specific rate decreased over time, from 4.75 per 100 person-years in 1995–1999 to 0.46 per 100 person-years in 2010–2014. The highest proportional increases for other causes were for cancer (4.0% to 18.0%), cardiovascular disease (3.0% to 12.2%) and other noncommunicable diseases (4.3% to 15.7%). Nevertheless, no cause-specific mortality rate increased over the study period; indeed, rates of death due to cardiovascular disease, other communicable diseases and other noncommunicable diseases declined statistically significantly.
Risk factors for death
In adjusted generalized estimating equation models, greater age was significantly associated with increasing risk of death for all causes except injury (Supplementary Table A3, Appendix 1). The strongest association was for cardiovascular disease, whereas the weakest was for HIV/AIDS. For all-cause mortality, the magnitude of the RR for a 10-year difference in age increased with time, from 1.24 (95% CI 1.18–1.29) in 1995–1999 to 1.72 (95% CI 1.63–1.82) in 2010–2014 (Supplementary Table A3, Appendix 1).
Sex differences in mortality risk were heterogeneous across time and across specific causes of death (Supplementary Tables A2 and A3, Appendix 1). All-cause mortality was higher among males than females in 1995–1999, but by 2010–2014, the reverse was true. Females also had a significantly lower risk of death due to HIV/AIDS in the early years (adjusted RR for females v. males in 1995–1999 0.50, 95% CI 0.41–0.62), but sex differences were not significantly different from null in later years (adjusted RR in 2010–2014 0.89, 95% CI 0.67–1.17). Females had a higher risk of death due to cardiovascular disease and noncommunicable causes than did males, neither of which varied with time.
All-cause mortality was higher among those who lived in a low-income neighbourhood (Supplementary Tables A2 and A3, Appendix 1). This pattern generally held for the various causes of death (although not all RRs reached statistical significance). Exceptionally, in the early years, there was no difference in death due to HIV/AIDS according to neighbourhood income (adjusted RR for lowest income quintile v. higher quintiles in 1995–1999 1.04, 95% CI 0.93–1.16), but by 2010–2014, living in a low-income neighbourhood was associated with a nearly twofold increased risk (adjusted RR 1.86, 95% CI 1.49–2.31). Residing in rural Ontario rather than an urban or suburban centre was significantly associated with increased all-cause mortality, a trend that was also observed for cancer-related deaths and those related to noncommunicable diseases.
Finally, being an immigrant compared to a long-term resident was significantly associated with lower risk of death from all causes, including HIV/AIDS, but not for other communicable diseases (Supplementary Table A3, Appendix 1).
Interpretation
Among HIV-infected adults in Ontario, we observed declines in all-cause and cause-specific mortality rates from 1995 to 2014 accompanied by a shift in leading causes of death. In more recent years, death was less likely to be attributed to HIV/AIDS and more likely to be reported as being due to other causes, predominantly cancer and cardiovascular disease. Nevertheless, HIV/AIDS was still the most commonly recorded cause of death, even by 2010–2014.
We observed a 77% reduction in all-cause mortality over the study period, from 6.69 to 1.53 deaths per 100 person-years. Our results confirm previous research in Ontario showing that the ratio of deaths due to HIV/AIDS to all-cause deaths declined significantly between 2000 and 2012, from 80% to 45%.10 This is undoubtedly a result of the widespread availability of cART since 1996, as well as the evolution to safer and more effective cART regimens. Similar findings have been reported in high-income countries where cART has been available for the past 2 decades.4,5,7,9 Such studies also show that death is increasingly attributed to non–AIDS-related causes, including non–AIDS-defining malignant disease, 5,6 cardiovascular disease6 and liver disease,4,6 even as rates of death from these causes decline.7,8 In the current study, in 1995–1999, age differences in HIV/AIDS-associated mortality were modest, likely because cART was not yet in widespread use. As time passed, greater age became more strongly associated with death from HIV/AIDS, following the pattern more consistently observed for cancer, cardiovascular disease, and communicable and noncommunicable diseases.
Sex differences in mortality rates varied across time and cause of death. Males were at higher risk for all-cause and HIV/AIDS-related mortality in 1995–1999, but by 2010–2014, females were at higher risk of all-cause mortality, and HIV/AIDS-related mortality did not differ by sex. Females were at higher risk for death due to cardiovascular disease or other noncommunicable disease across all years studied. Other investigators have found a shorter life expectancy among women with HIV infection in North America.23,24 These sex-based disparities are concerning and merit further investigation to determine to what degree they are due to differences in the course of HIV infection, response to cART or social determinants of health. Sex comparisons over time are also complicated by underlying secular changes in the nature of HIV infection epidemics in Ontario.25 In 1995–1999, most HIV-infected males would have been with untreated infection for longer than women or were infected via injection drug use, which heightens the risk of death,5,26–28 whereas in later years, male mortality patterns would have been weighted in favour of men who have sex with men, who have better profiles of engagement with HIV infection care.29,30
Neighbourhood income was unassociated with death due to HIV/AIDS in the earlier periods, a finding that we attribute to lesser use of cART among people of all socioeconomic groups in 1995–1999. More recently, the association between low neighbourhood income and HIV/AIDS-related mortality was more consistent with income-related health disparities that are widely recognized for people with HIV infection10,31,32 and with many other conditions.33–35 Mortality rates were generally lower among immigrants than among long-term residents, consistent with the “healthy immigrant effect,” whereby new immigrants are typically healthier than those native to a country,36 including in Canada.37,38 Greenaway and colleagues39 found that immigrants in Quebec had lower rates of problematic drug use than nonimmigrants, which may further explain our finding. Rural residents had a greater risk for all-cause mortality, which confirms previous research among people with HIV infection.40,41 This may be partially explained by the considerable challenges in accessing health care providers with HIV expertise in rural locations.42
Strengths and limitations
A strength of our study is that we used population-level data from a broad and diverse population of HIV-infected people. Nevertheless, there are limitations. Although we used a validated algorithm to identify people with HIV infection, our estimates are restricted to those whose infection had been diagnosed and who were receiving care. We relied on vital statistics data to classify underlying cause of death based on death certificate reports, for which data quality is imperfect.43 We suspect that misclassification, if it occurred, would have been either nondifferential or overcalling of HIV/AIDS as the cause of death, meaning that rates of death due to HIV/AIDS may have been overestimated and rates due to other causes underestimated.44 Finally, important risk factors for death, including CD4 count or HIV viral load,4,5,11,45,46 injection drug use,47 and time since HIV infection diagnosis, treatment initiation and treatment adherence,2,10,48 were unavailable for our analyses.
Conclusion
Our findings show that mortality rates declined between 1995–1999 and 2010–2014 among people with HIV infection in Ontario, although HIV/AIDS remained the leading cause of death. As deaths were increasingly non–HIV/AIDS-related over the study period, care should also focus on the prevention and management of common chronic conditions such as cardiovascular disease and screening for common cancers. Special attention should be given to comprehensive care models for those living in low-income neighbourhoods and in nonurban settings, which may include initiatives to increase care accessibility such as e-consultations and telemedicine.49–51
Acknowledgements
The authors gratefully acknowledge Amy Mark Fraser for carrying out preliminary analyses. They also acknowledge medical writer Jennifer Pereira for assistance with preparation of early versions of the manuscript.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Ann Burchell, Janet Raboud, Jessy Donelle and Claire Kendall conducted the analysis and initial interpretation of the data. Ann Burchell, Janet Raboud and Claire Kendall drafted the manuscript. All of the authors contributed to the conception and design of the study, critically revised the manuscript for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Data sharing: The data set from this study is held securely in coded form at ICES. Although data-sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS. The full data set creation plan and underlying analytic code are available from the authors on request, with the understanding that the programs may rely on coding templates or macros that are unique to ICES.
Funding: This study was funded by Canadian Institutes of Health Research grant FRN-TT5-128270.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred. Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions and statements expressed herein are those of the authors and not necessarily those of CIHI. Parts of this material are based on data and information provided by Cancer Care Ontario (CCO). The opinions, results, view and conclusions reported in this paper are those of the authors and do not necessarily reflect those of CCO. No endorsement by CCO is intended or should be inferred. Parts of this report are based on Ontario Registrar General information on deaths, the original source of which is Service Ontario. The views expressed herein are those of the authors and do not necessarily reflect those of the Ontario Registrar General or Ministry of Government Services.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/7/1/E1/suppl/DC1.
References
- Copyright 2019, Joule Inc. or its licensors
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- The burden of cancer among people living with HIV in Ontario, Canada, 1997-2020: a retrospective population-based cohort study using administrative health data
- British Columbia CARMA-CHIWOS Collaboration (BCC3): protocol for a community-collaborative cohort study examining healthy ageing with and for women living with HIV