


Abstract
Background: Cisgender women with HIV experience an elevated risk of cervical cancer compared with HIV-negative women, but this cancer can be prevented through regular cervical cancer screening. Our study objective was to measure adherence to current national cervical cancer screening guidelines among women with HIV in 3 Canadian provinces and identify factors associated with delays.
Methods: We conducted a cross-sectional study using the baseline questionnaire of the Canadian HIV Women’s Sexual and Reproductive Health Cohort Study (CHIWOS). Participants were recruited through clinics, peers and community organizations in British Columbia, Ontario and Quebec. Women were eligible for inclusion if they were cisgender female with HIV, aged 21–70 years, and never had cervicectomy/hysterectomy.
Results: Of 1189 eligible participants, 815 (68.5%) had received cervical cancer screening less than 1 year ago (i.e., as recommended), 211 (17.7%) 1–3 years ago (i.e., moderate delay) and 163 (13.7%) at least 3 years ago or never (i.e., long delay). Overall, 309 (26.0%) had never discussed the need for a Papanicolaou smear with a nurse/doctor. Factors associated with a long delay were living in Ontario (adjusted odds ratio [OR] 2.51, 95% confidence interval [CI] 1.29–4.88) or Quebec (adjusted OR 3.70, 95% CI 1.79–7.67) (v. BC), being sexually inactive in the past 6 months (adjusted OR 2.02, 95% CI 1.25–3.25), having unknown or < 200 cells/mm3 CD4 counts (adjusted OR 1.78, 95% CI 1.11–2.85) and having a male HIV care provider (adjusted OR 2.15, 95% CI 1.36–3.42).
Interpretation: Over one-third of women reported cervical cancer screening delays, and one-quarter had never discussed cervical cancer screening recommendations with a health care provider. Additional efforts are needed to improve women’s and health care providers’ awareness of cervical cancer screening recommendations, particularly among women who are sexually inactive, who are immunosuppressed and who have male HIV care providers.
An estimated one-quarter of all people living with HIV in Canada are women,1 and cisgender women with HIV have a higher risk of cervical cancer than HIV-negative cisgender women2–4 because of a higher persistence of high-risk human papillomavirus (HPV) infections. 5–7 Cervical cancer has been an AIDS-defining condition since 1993.8–10 It is the 16th leading cause of death among women in Canada11 but the third leading cause of death among women in low-income countries,12 which are often regions with the greatest burden of HIV.13
Cervical cancer is largely preventable with routine cervical cancer screening (Papanicolaou smears) and HPV vaccination. 14,15 Since the introduction of Pap smears, the incidence of cervical cancer has decreased dramatically in Canada and has stabilized since 2006 at 7–8 per 100 000 women.11 Canadian guidelines recommend yearly cervical cytology for women with HIV and do not consider HPV cotesting in this population.16–20 In the United States, recommendations were recently modified to increase cervical cancer screening intervals to every 3 years following 3 consecutive Pap smears with normal results, and they included consideration of HPV cotesting, where available, for women with HIV who are older than 30 years.21 Previous studies in high-income countries reported that only 29%–58% of women with HIV had been screened for cervical cancer in the previous 1–3 years,22–25 with higher HIV viral loads and lower CD4 counts associated with longer delays.24
Our primary objectives were to measure the prevalence of self-reported adherence to cervical cancer screening among women with HIV in Canada and to identify factors associated with delays in cervical cancer screening. A secondary objective was to identify participants’ reasons for not receiving cervical cancer screening according to the length of the delay, to inform future care interventions.
Methods
Study design
We conducted a cross-sectional study using the baseline questionnaire of the Canadian HIV Women’s Sexual and Reproductive Health Cohort Study (CHIWOS). CHIWOS (www.chiwos.ca) is a cohort study of 1422 women with HIV, grounded in community-based research principles. The cohort profile was described in more detail in previous publications. 26,27 Briefly, eligible participants self-identified as women with HIV, were 16 years of age or older and resided in British Columbia, Ontario or Quebec. Participants were recruited through clinics (A.d.P., K.P.-B., I.B., N.P., M.L.), peers and community organizations (D.B., K.P.-B., A.K.) using a nonrandom, purposive sampling strategy.28 Within each province, we aimed to recruit women according to the same geographical distribution as that reported by public health reports.26 Purposive sampling was also done to recruit trans women, Indigenous women, women who inject drugs and young women (< 30 yr) to allow analysis of health care access and outcomes for these specific vulnerable populations. Throughout this paper, we used the term women with HIV rather than females with HIV to respect community preference on language.29
Data source
For the present analysis, we used data from the baseline questionnaire (see Appendix 1, available at www.cmajopen.ca/content/7/2/E217/suppl/DC1 and at www.chiwos.ca; A.d.P., A.B, K.S., N.O., D.B., K.P.-B., I.B., N.P., M.L. and A.K. participated in writing the questionnaire) completed between August 2013 and May 2015. Trained peer research associates (women with lived experience with HIV who underwent research training) administered questionnaires in English or French using the Web-based platform FluidSurveys to facilitate data collection. Interviews were conducted in person at collaborating HIV clinics, at AIDS service or community organizations, in women’s homes or by phone or Skype for participants living in rural areas. We restricted the present analysis to cisgender women eligible for cervical cancer screening aged 21–70 years, excluding women who reported previous cervicectomy/hysterectomy and those who answered “don’t know” or “prefer not to answer” or did not respond to the 2 questions on Pap smear testing.
Primary outcome
The primary outcome was delay in cervical cancer screening (either a moderate delay, i.e., reporting their last Pap smear was 1–3 years ago, or a long delay, i.e., reporting their last Pap smear was at least 3 years ago or they had never been tested) compared with the recommended interval based on current Canadian guidelines. Two questions were asked on the basis of questions from the Canadian Community Health Survey.30 Women were asked: “Have you ever had a Pap test? The answer options were (a) yes, (b) no, (c) don’t know and (d) prefer not to answer. Women who answered yes were then asked: “When, approximately, was the last time you had a Pap test?” The answer options were (a) less than 6 months ago, (b) 6 months to less than 1 year ago, (c) 1 year to less than 3 years ago, (d) 3 years to less than 5 years ago, (e) 5 years ago or more, (f) don’t know and (g) prefer not to answer.
Covariates
Potential correlates for time since last Pap smear included characteristics related to sociodemographic factors (age, education, ethnicity, household yearly income, city size and province of residence); sexual and reproductive health (sexual orientation, relationship status, sexual activity in previous 6 months, experience of sexual violence, having children, menopause status, use of hormonal birth control); self-reported markers of health (smoking, drug use, body mass index, CD4 count, HIV viral load, use of antiretroviral therapy, general health); and factors related to health care services (HIV medical care, gender and specialty of HIV care provider, location of clinic, travel time from residence to clinic, and whether Pap smears were offered at their HIV clinic). The use of a hormonal contraceptive method included the birth control pill, hormonal intrauterine device, patches, implants, rings or injections.
Statistical analysis
Descriptive statistics (median and interquartile range [IQR] for continuous variables, and no. [%] for categorical variables) were used to characterize distributions of study variables, with 95% confidence intervals (CIs) when pertinent. Multinomial regression analyses were conducted using a 3-category outcome based on timing since last Pap smear: less than 1 year ago (reference category, recent testing), between 1 and 3 years ago (moderate delay), and at least 3 years ago or never (long delay). For the analyses including variables for characteristics of health care, only women who had accessed HIV care in the last year were included. A multivariable model was built retaining age by default, but other variables were included if unadjusted analyses revealed a significant association for 1 of the outcome categories at p < 0.20. Variables were then removed if they did not improve in significance or did not alter the significance of other variables. Knowledge of whether the clinic offered Pap smears was discarded from the multivariable model because of concerns regarding reverse causality. Data were analyzed (A.d.P, A.B., K.S., E.D.) with Stata version 11.2 (StataCorp LLC).
Ethics approval
The study was reviewed and approved by the Community Advisory Committee of the Canadian Institutes of Health Research — Canadian HIV Trials Network, and by the research ethics boards of Simon Fraser University, University of British Columbia Providence Health Care, Women’s College Hospital and McGill University Health Centre. All participants provided written and voluntary informed consent.
Results
A total of 1422 women completed the baseline interview. The median survey completion time was 120 (IQR 90–150) minutes. Of the women who completed the interview, 233 were excluded from this analysis: 57 identified as trans women, 29 were younger than 21 years or older than 70 years, 98 had had a cervicectomy, 36 had had a hysterectomy and 13 did not answer the cervical cancer screening questions. These exclusions yielded a final analytical sample of 1189 women (291 from BC, 604 from Ontario and 294 from Quebec).
The median age was 42 (IQR 35–50) years; 40% identified as white, 31% as African, Caribbean or black, and 22% as Indigenous (Table 1). Most (95%) had received HIV medical care in the previous year, 83% were taking combination antiretroviral therapy and 77% reported that their most recent HIV viral load was undetectable (< 50 copies/mL).
Baseline characteristics of participants in the Canadian HIV Women’s Sexual and Reproductive Health Cohort Study (CHIWOS) included in these analyses
Overall, 68.5% of women reported their last Pap smear was less than 1 year ago, 17.7% reported that it was between 1 and 3 years ago, 4.8% said that it was between 3 and 5 years ago, 4.6% reported that it was 5 or more years ago and 4.3% said they had never had a Pap smear.
Characteristics associated with delays in Pap smear testing
Several sociodemographic and HIV clinical care variables were associated with delays in Pap smear testing in unadjusted analyses (Figure 1). “Not knowing whether Pap smears were offered at the HIV clinic” (odds ratio [OR] 2.12, 95% CI 1.40–3.24 for having the last Pap smear 1–3 years ago, i.e., moderate delay; OR 3.54, 95% CI 2.31–5.44, for having it at least 3 years ago or never, i.e., long delay) and “Not having accessed HIV care in the last year” (OR 3.64, 95% CI 1.99–6.68, for moderate delay; OR 3.34, 95% CI 1.71–6.52, for long delay) showed the strongest associations.
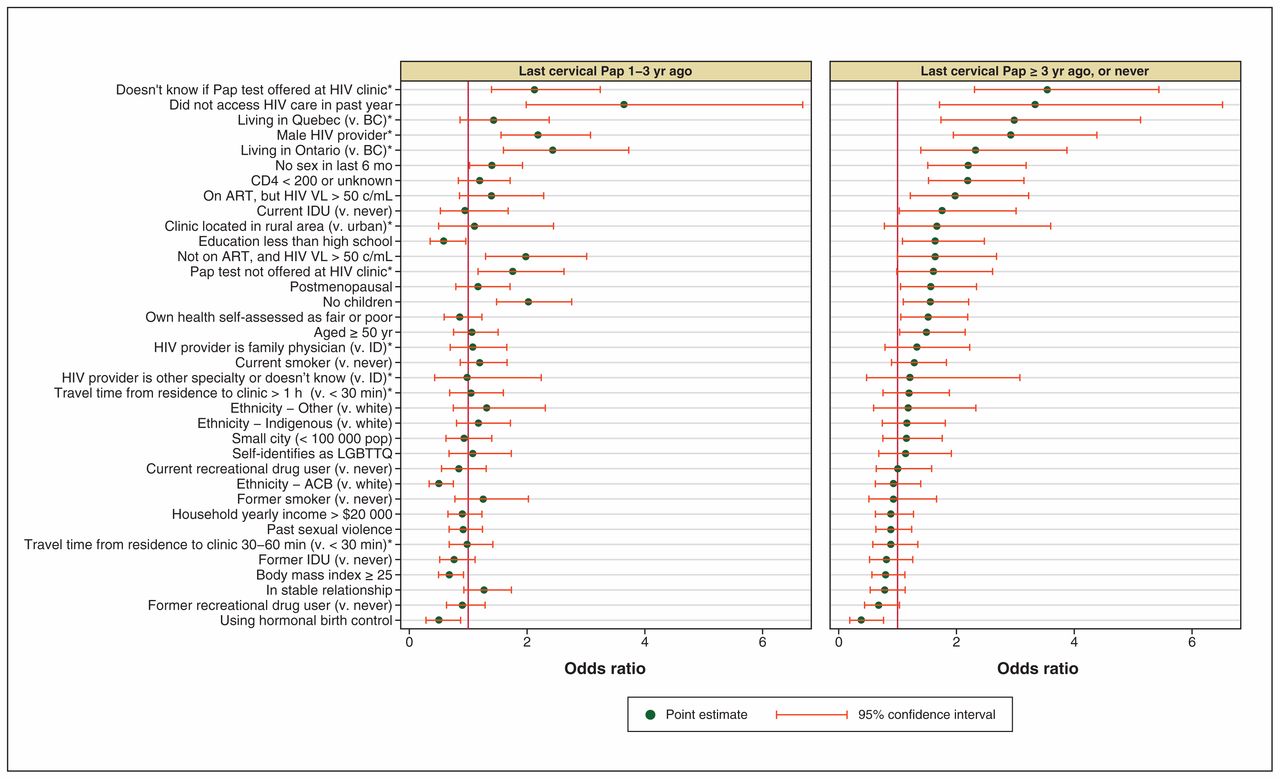
Unadjusted correlates of self-reported time since their most recent Pap smear among HIV-positive women in the Canadian HIV Women’s Sexual and Reproductive Health Cohort Study, 2013–2015. Note: *Indicates analyses restricted to women who received HIV care in the previous year (n = 1129). ACB = African, Caribbean or black, ART = antiretroviral therapy, c = copies, ID = infectious disease specialist, IDU = injection drug user, LGBTTQ = lesbian, gay, bisexual, trans, 2-spirit, queer, VL = viral load.
In the adjusted model (Table 2 and Figure 2), women had higher odds of a moderate delay in cervical cancer screening if they were living in Ontario (adjusted OR 2.28, 95% CI 1.35–3.87) or if their HIV provider was a man (adjusted OR 1.69, 95% CI 1.15–2.49). They had lower odds of a moderate delay if they identified as African, Caribbean or black (adjusted OR 0.47, 95% CI 0.29–0.77) or if they were in a relationship (adjusted OR 0.62, 95% CI 0.42–0.93). Women had higher odds of a long delay if they were living in Ontario (adjusted OR 2.51, 95% CI 1.29–4.88) or Quebec (adjusted OR 3.70, 95% CI 1.79–7.67), were sexually inactive (adjusted OR 2.02, 95% CI 1.25–3.25), had CD4 counts that were unknown or less than 200 cells/mm3 (adjusted OR 1.78, 95% CI 1.11–2.85) or if their HIV provider was a man (adjusted OR 2.15, 95% CI 1.36–3.42).
Correlates of self-reported time since their most recent Pap smear among HIV-positive women who had received HIV care in the last year, in the Canadian HIV Women’s Sexual and Reproductive Health Cohort Study, 2013–2015 (multivariable model, n = 1129)

Adjusted correlates of self-reported time since their most recent Pap smear among HIV-positive women who accessed HIV care in the previous year (n = 1129), in the Canadian HIV Women’s Sexual and Reproductive Health Cohort Study, 2013–2015. Note: ACB = African, Caribbean and black, ART = antiretroviral therapy, c = copies, IDU = injection drug user, VL = viral load. The estimates presented are those of the multivariable model including all of these variables.
Reasons for delay in Pap smear testing
When participants were asked if a doctor or nurse had ever discussed with them the need for a regular Pap smear, 306 (25.7%) answered no. This proportion rose to 57.1% (64/112) for women who had previously had a Pap smear but it had been at least 3 years ago, and to 72.5% (37/51) for women who had never had a Pap smear. The most common self-reported reason for not having a Pap smear in the past 12 months (women could select multiple answers) was “not getting around to it” (47%, 174/374) followed by “not thinking it was necessary” (38%, 142/374), “disliking having the procedure done” (20%, 74/374), “my health care provider has never mentioned it” (19%, 72/374) and “fear” (14%, 54/374, included fear of pain, embarrassment, HIV disclosure or finding something wrong). Reporting “not getting around to it” was less common among women with long delays than among women with moderate delays (36%, 58/163 v. 55%, 116/211, respectively), whereas the opposite was observed for “disliking having the procedure done” (25%, 41/163 v. 16%, 33/211, respectively) and “fear” (19%, 31/163 v. 11%, 23/211, respectively) (Figure 3).
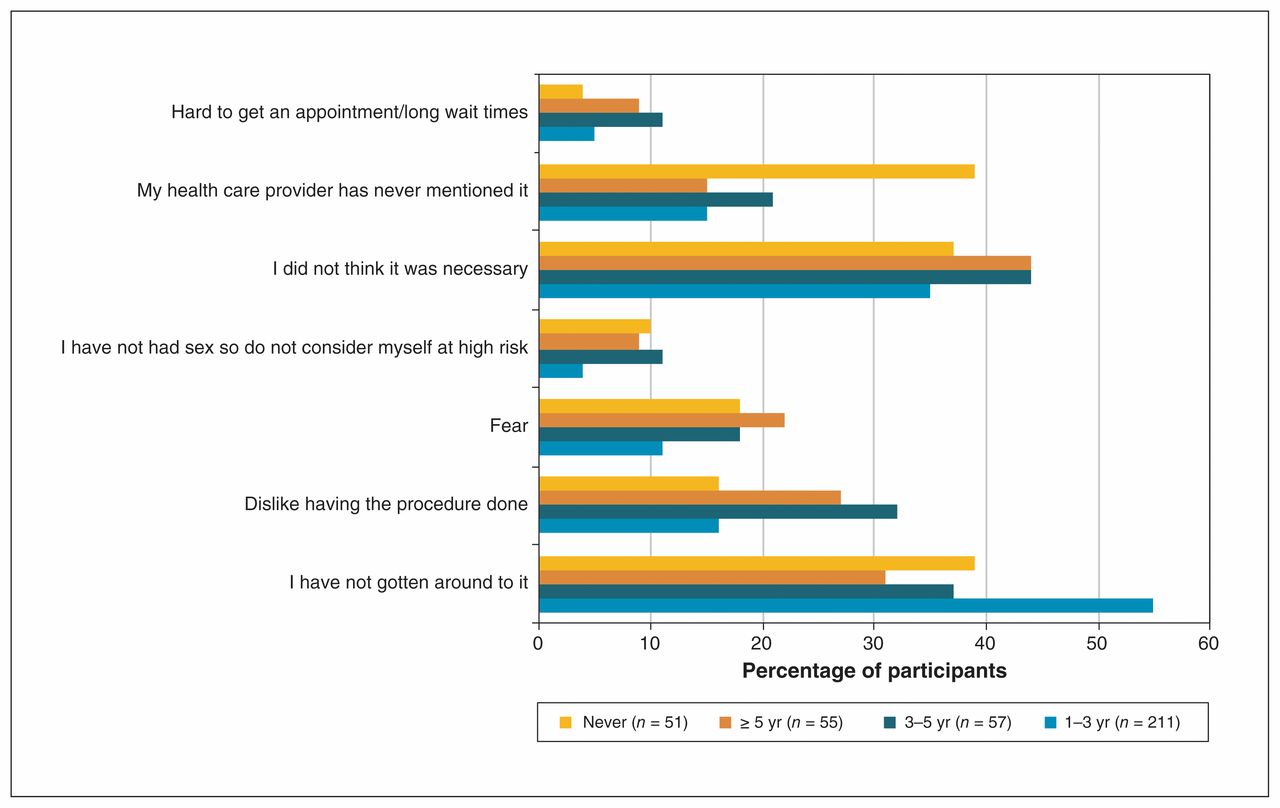
Percentages of participants who reported various reasons for not having had a Pap smear in the last 12 months, in the Canadian HIV Women’s Sexual and Reproductive Health Cohort Study, 2013–2015. Participants are grouped according to the length of time since their most recent Pap smear.
Subanalyses to examine interprovincial differences
Pap smear testing in the past year was reported by 81.1% of participants living in BC, 63.1% of participants living in Ontario and 67.3% of participants living in Quebec. To examine interprovincial differences, post-hoc analyses were conducted. In BC, 114 of the 288 included participants attended an HIV clinic for women with HIV and their families located in a provincial women’s health hospital. There is no women’s only HIV clinic within a women’s only hospital in Quebec or Ontario. We stratified women in BC according to their HIV clinic and found that 93.0% of women followed at the clinic located in the women’s health hospital reported having had a Pap smear in the past year, compared with 74.1% of women of BC followed elsewhere and 66.9% of women in Ontario and Quebec (combined).
Interprovincial differences were also identified when we applied the adjusted model to women stratified by provinces. The gender of the HIV provider had no effect in Quebec, while having a male HIV provider strongly increased the odds of a long delay in BC (adjusted OR 5.97, 95% CI 1.77–20.21) and of both moderate (adjusted OR 1.79, 95% CI 1.02–3.14) and long delays in Ontario (adjusted OR 2.18, 95% CI 1.12–4.67).
Interpretation
In this large, cross-sectional analysis of Canadian women living with HIV, 68.5% of women self-reported having had a Pap smear within the preceding year, as recommended by current Canadian cervical cancer screening guidelines.16–20 Moderate delays were not uncommon, with 17.7% reporting that their last Pap test occurred 1–3 years ago. Among women who had accessed HIV care in the previous year, women with moderate delays tended to live in Ontario; identify with an ethnicity other than African, Caribbean or black; be in a relationship; and have a male HIV provider. Long delays (i.e., ≥ 3 yr or never), reported by 13.7%, were more common among women living in Ontario or Quebec, who were sexually inactive, who did not know their CD4 count or reported having a lower CD4 count, and who reported that their HIV provider was a man.
More than a quarter of participants reported that a nurse or doctor had never discussed with them the need for regular cervical cancer screening (73% for women who had never had a Pap smear). As previously reported in the general population, providers have a crucial role to play in the adherence to cervical cancer screening recommendations31,32 and our results underline the importance of better communicating the need for cervical cancer screening to women with HIV. The specialty of the HIV provider as reported by participants did not change the odds of adherence to cervical cancer screening. Others previously reported that women with HIV receiving care from a gynecologist or family physician had increased receipt of Pap smears,23,33–36 but when looking at the specialty of the HIV provider specifically, another study reported an absence of effect.37 Our finding could also be due to misclassification of the specialty by participants. However, the gender of the HIV provider did affect delays in cervical cancer screening, particularly in BC and Ontario. This finding was also previously documented in Ontario36 and may be due to a combination of male providers prioritizing different issues and women feeling uncomfortable having a gynecological examination done by a man. Women with HIV experience disproportionate rates of violence38,39 and providing trauma informed care40 could also improve women’s care experience. In circumstances where performing a Pap smear is problematic for either the provider or the patient, potential solutions may include office/schedule organization;22,41 systematic reminders;42,43 collaboration with a nurse, female colleague, family physician or gynecologist to provide cervical cancer screening;23,33,44 or offering HPV self-sampling. Indeed, HPV self-sampling for cervical cancer screening has been shown to be very acceptable and feasible for hard-to-reach women, including ethnic minorities and Indigenous women,45,46 particularly when the kits are mailed or delivered home in person.32,47–49
Being in a relationship and sexually inactive increased the likelihood of cervical cancer screening delays, as previously reported by others.50,51 Explanations about HPV-related cancers need to specify that the risk remains even if a woman is no longer sexually active, because decades can pass between an initial HPV infection and the development of cervical cancer. The effect direction of ethnicity differs widely in the literature, but the impact of lower CD4 counts on cervical cancer screening adherence was previously reported by others.52,53 We hypothesize that multiple competing health or social priorities probably lead to postponement of preventive care. The interprovincial differences may be caused by a difference in providers’ practices, in health care systems, in billing systems, in public health promotion of cervical cancer screening or in characteristics of women, but they remain unexplained by our data. However, the results for women who attended the women’s HIV clinic in a women’s hospital showed the benefit of the clinic’s approach for cervical cancer screening adherence. Part of their success is likely due to the “one-stop shop” approach, which means that women do not have to seek to have all of their care needs met through fragmented care delivery.44,54 When this approach is not possible, effective communication between providers is essential to ensure integrated care.44
Limitations
There are many strengths to our analysis, including the fact that the CHIWOS survey incorporated questions assessing multiple factors influencing the receipt of cervical cancer screening, incorporating both patient and health care system variables. The questionnaires were created and piloted by both women with HIV and medical experts.55 CHIWOS is the largest Canadian cohort of women with HIV, and 81% of all women with HIV in Canada reside in the 3 participating provinces. Nevertheless, our study has limitations. Although CHIWOS recruited approximately 10% of all women living with HIV in Canada, participants were not sampled randomly and may not be representative of all women living with HIV in Canada. We do not have data on women who declined the invitation to participate, but we assume that they would differ in some manner from the participants. The data were collected between 3 and 5 years ago. The time since last cervical cancer screening was measured using self-report, which may underestimate delays because of telescoping bias (i.e., women underestimating the time since the test occurred); this limitation of self-reported data when compared with administrative records has been identified by others.56 Measurement via interview might also have underestimated delay because of social desirability bias. Also, the category “1–3 years” may combine delays that would not be perceived as clinically significant (e.g., 14 mo) with delays that would be more concerning (e.g., 30 mo). Our questions on providers were specific to HIV providers. We did not ask whether participants received care from a primary care physician other than their HIV provider.
Conclusion
Our results confirm the need to improve delivery of cervical cancer screening for women with HIV in Canada and indicate multiple opportunities to do so. Women with HIV first need to access HIV care because lower immunity increases their risk for HPV persistence and development of cancers. Once women are in care, discussions on cervical cancer screening benefits need to occur regularly. More sensitive behaviour and attention to patient’s comfort by the Pap smear test performer can strongly affect the experience of patients and their ensuing adherence with screening recommendations. HIV care providers should facilitate awareness of and access to cervical cancer screening for all women with HIV.
Acknowledgements
The members of the CHIWOS Research Team thank all of the women living with HIV who participated in the research and entrusted CHIWOS with their experiences of HIV treatment, care and support. They also thank the entire national team of co-investigators, collaborators and peer research associates. They acknowledge the three provincial community advisory boards, the national CHIWOS Aboriginal advisory board and their partnering organizations for supporting the study. They also acknowledge the BC Centre for Excellence in HIV/AIDS for in-kind data management and analytic support.
Footnotes
CHIWOS Research Team: British Columbia: Aranka Anema (University of British Columbia, Vancouver), Denise Becker (Positive Living Society of British Columbia, Vancouver), Lori Brotto (University of British Columbia, Vancouver), Allison Carter (British Columbia Centre for Excellence in HIV/AIDS, Vancouver, and Simon Fraser University, Burnaby), Claudette Cardinal (Simon Fraser University, Burnaby), Guillaume Colley (British Columbia Centre for Excellence in HIV/AIDS, Vancouver), Erin Ding (British Columbia Centre for Excellence in HIV/AIDS, Vancouver), Janice Duddy (Pacific AIDS Network, Vancouver), Nada Gataric (British Columbia Centre for Excellence in HIV/AIDS, Vancouver), Robert S. Hogg (British Columbia Centre for Excellence in HIV/AIDS, Vancouver, and Simon Fraser University, Burnaby), Terry Howard (Positive Living Society of British Columbia, Vancouver), Shahab Jabbari (British Columbia Centre for Excellence in HIV/AIDS, Vancouver), Evin Jones (Pacific AIDS Network, Vancouver), Mary Kestler (Oak Tree Clinic, BC Women’s Hospital and Health Centre, Vancouver), Andrea Langlois (Pacific AIDS Network, Vancouver), Viviane Lima (British Columbia Centre for Excellence in HIV/AIDS, Vancouver), Elisa Lloyd-Smith (Providence Health Care Elisa Lloyd-Smith), Melissa Medjuck (Positive Women’s Network, Vancouver), Cari Miller (Simon Fraser University, Burnaby), Deborah Money (Women’s Health Research Institute, Vancouver), Valerie Nicholson (Simon Fraser University, Burnaby), Gina Ogilvie (British Columbia Centre for Disease Control, Vancouver), Sophie Patterson (Simon Fraser University, Burnaby), Neora Pick (Oak Tree Clinic, BC Women’s Hospital and Health Centre, Vancouver), Eric Roth (University of Victoria, Victoria), Kate Salters (Simon Fraser University, Burnaby), Margarite Sanchez (ViVA, Positive Living Society of British Columbia, Vancouver), Jacquie Sas (CIHR Canadian HIV Trials Network, Vancouver), Paul Sereda (British Columbia Centre for Excellence in HIV/AIDS, Vancouver), Marcie Summers (Positive Women’s Network, Vancouver), Christina Tom (Simon Fraser University, Burnaby), Clara Wang (British Columbia Centre for Excellence in HIV/AIDS, Vancouver), Kath Webster (Simon Fraser University, Burnaby), Wendy Zhang (British Columbia Centre for Excellence in HIV/AIDS, Vancouver). Ontario: Rahma Abdul-Noor (Women’s College Research Institute, Toronto), Jonathan Angel (Ottawa Hospital Research Institute, Ottawa), Fatimatou Barry (Women’s College Research Institute, Toronto), Greta Bauer (University of Western Ontario, London), Kerrigan Beaver (Women’s College Research Institute, Toronto), Anita Benoit (Women’s College Research Institute, Toronto), Breklyn Bertozzi (Women’s College Research Institute, Toronto), Sheila Borton (Women’s College Research Institute, Toronto), Tammy Bourque (Women’s College Research Institute, Toronto), Jason Brophy (Children’s Hospital of Eastern Ontario, Ottawa), Ann Burchell (University of Toronto, Toronto), Allison Carlson (Women’s College Research Institute, Toronto), Lynne Cioppa (Women’s College Research Institute, Toronto), Jeffrey Cohen (Windsor Regional Hospital, Windsor), Tracey Conway (Women’s College Research Institute, Toronto), Curtis Cooper (Ottawa Hospital Research Institute, Ottawa), Jasmine Cotnam (Women’s College Research Institute, Toronto), Janette Cousineau (Women’s College Research Institute, Toronto), Marisol Desbiens (Women’s College Research Institute, Toronto), Annette Fraleigh (Women’s College Research Institute, Toronto), Brenda Gagnier (Women’s College Research Institute, Toronto), Claudine Gasingirwa (Women’s College Research Institute, Toronto), Saara Greene (McMaster University, Hamilton), Trevor Hart (Ryerson University, Toronto), Shazia Islam (Women’s College Research Institute, Toronto), Charu Kaushic (McMaster University, Hamilton), Logan Kennedy (Women’s College Research Institute, Toronto), Desiree Kerr (Women’s College Research Institute, Toronto), Gladys Kwaramba (Women’s College Research Institute, Toronto), Lynne Leonard (University of Ottawa, Ottawa), Johanna Lewis (Women’s College Research Institute, Toronto), Carmen Logie (University of Toronto, Toronto), Shari Margolese (Women’s College Research Institute, Toronto), Marvelous Muchenje (Women’s Health in Women’s Hands, Toronto), Mary (Muthoni) Ndung’u (Women’s College Research Institute, Toronto), Kelly O’Brien (University of Toronto, Toronto), Charlene Ouellette (Women’s College Research Institute, Toronto), Je Powis (Toronto East General Hospital, Toronto), Corinna Quan (Windsor Regional Hospital, Windsor), Janet Raboud (Ontario HIV Treatment Network, Toronto), Anita Rachlis (Sunnybrook Health Sciences Centre, Toronto), Edward Ralph (St. Joseph’s Health Care, London), Sean Rourke (Ontario HIV Treatment Network, Toronto), Sergio Rueda (Ontario HIV Treatment Network, Toronto), Roger Sandre (Haven Clinic, Sudbury), Fiona Smaill (McMaster University, Hamilton), Stephanie Smith (Women’s College Research Institute, Toronto), Tsitsi Tigere (Women’s College Research Institute, Toronto), Wangari Tharao (Women’s Health in Women’s Hands, Toronto), Sharon Walmsley (Toronto General Hospital Research Institute, Toronto), Wendy Wobeser (Queen’s University, Kingston), Jessica Yee (Native Youth Sexual Health Network, Toronto), Mark Yudin (St. Michael’s Hospital, Toronto). Quebec: Dada Mamvula Bakombo (McGill University Health Centre, Montréal), Jean-Guy Baril (Université de Montréal, Montréal), Marc Boucher (Centre Hospitalier Universitaire Ste-Justine, Montréal), Isabelle Boucoiran (Centre Hospitalier Universitaire Sainte-Justine, Montréal), Nora Butler Burke (Concordia University, Montréal), Pierrette Clément (McGill University Health Cente, Montréal), José Côté (Centre Hospitalier de l’Université de Montréal, Montréal), Janice Dayle (McGill University Health Centre, Montréal), Danièle Dubuc, (McGill University Health Centre, Montréal), Mylène Fernet (Université du Québec à Montréal, Montréal), Marilyn Fortin-Hugues (Université du Québec à Montréal, Montréal), Marilou Gagnon (University of Ottawa, Ottawa), Danielle Groleau (McGill University, Montréal), Fatima Kakkar (Centre Hospitalier Universitaire Sainte-Justine, Montréal), Maxime Kiboyogo (McGill University Health Centre, Montréal), Marina Klein (McGill University Health Centre, Montréal), Gary Lacasse (Canadian AIDS Society, Ottawa), Valérie Lamarre (Centre Hospitalier Universitaire Ste-Justine, Montréal), Carrie Martin (Native Women’s Shelter of Montreal, Montréal), Lyne Massie, (Université de Québec à Montréal, Montréal), Brigitte Ménard, (McGill University Health Centre, Montréal), Ken Monteith (COCQ-SIDA, Montréal), Nadia O’Brien (McGill University, Montréal), Joanne Otis (Université du Québec à Montréal, Montréal), Doris Peltier (Canadian Aboriginal AIDS Network, Montréal), Alie Pierre (McGill University Health Centre, Montréal), Karène Proulx-Boucher (McGill University Health Centre, Montréal), Danielle Rouleau (Centre Hospitalier de l’Université de Montréal, Montréal), Geneviève Rouleau (Centre Hospitalier de l’Université de Montréal, Montréal), Édénia Savoie (McGill University Health Centre, Montréal), Cécile Tremblay (Centre Hospitalier de l’Université de Montréal, Montréal), Benoit Trottier (Clinique Médicale Urbaine du Quartier Latin, Montréal), Jason Szabo (Clinique l’Actuel, Montréal), Sylvie Trottier (Centre Hospitalier Universitaire de Québec, Quebec City), Christos Tsoukas (McGill University Health Centre, Montréal). Other Canadian provinces or international jurisdictions: Jacqueline Gahagan (Dalhousie University, Halifax), Catherine Hankins (University of Amsterdam, Amsterdam), Renee Masching (Canadian Aboriginal AIDS Network, Dartmouth), Susanna Ogunnaike-Cooke (Public Health Agency of Canada, Ottawa). All other CHIWOS Research Team members wish to remain anonymous.
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Alexandra de Pokomandy, Ann Burchell, Nadia O’Brien, Dada Mamvula Bakombo, Karène Proulx-Boucher, Neora Pick, Mona Loufty and Angela Kaida contributed to the study conception and design. Nadia O’Brien, Dada Mamvula Bakombo and Karène Proulx-Boucher contributed to the data acquisition. Alexandra de Pokomandy, Ann Burchell, Kate Salters, Erin Ding and Angela Kaida contributed to the data analysis. All authors contributed to the interpretation of the data. Alexandra de Pokomandy, Ann Burchell, Kate Salters and Angela Kaida contributed to drafting the article and the other authors revised it critically for important intellectual content. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This work was supported by a Canadian Institutes of Health Research (CIHR) operating grant (MOP-111041), the CIHR Canadian HIV Trials Network (CTN 262), the Ontario HIV Treatment Network and the Academic Health Science Centres (AHSC) Alternative Funding Plans (AFP) Innovation Fund. Alexandra de Pokomandy received salary support from Fonds de la recherche en santé du Québec (FRQS) and Fédération des médecins omnipraticiens du Québec through an LE-250 scholarship. Nadia O’Brien and Isabelle Boucoiran also received salary support from FRQS. Ann Burchell and Angela Kaida received salary support from CIHR.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/7/2/E217/suppl/DC1.
References
- Copyright 2019, Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.