


Abstract
Background: Cardiovascular research has traditionally been dedicated to “tombstone” outcomes, with little attention dedicated to the patient’s perspective. We evaluated disability-free survival as a patient-defined outcome after cardiac surgery.
Methods: We conducted a retrospective cohort study of patients aged 40 years and older who underwent coronary artery bypass grafting (CABG) or single or multiple valve (aortic, mitral, tricuspid) surgery in Ontario between Oct. 1, 2008, and Dec. 31, 2016. The primary outcome was disability (a composite of stroke, 3 or more nonelective hospital admissions and admission to a long-term care facility) within 1 year after surgery. We assessed the procedure-specific risk of disability using cumulative incidence functions, and the relative effect of covariates on the subdistribution hazard using Fine and Gray models.
Results: The study included 72 824 patients. The 1-year incidence of disability and death was 2431 (4.6%) and 1839 (3.5%) for CABG, 677 (6.5%) and 539 (5.2%) for single valve, 118 (9.0%) and 140 (10.7%) for multiple valve, 718 (9.0%) and 730 (9.2%) for CABG and single valve, and 87 (13.1%) and 94 (14.1%) for CABG and multiple valve surgery, respectively. With CABG as the reference group, the adjusted hazard ratios for disability were 1.34 (95% confidence interval [CI] 1.21–1.48) after single valve, 1.43 (95% CI 1.18–1.75) after multiple valve, 1.38 (95% CI 1.26–1.51) after CABG and single valve, and 1.78 (95% CI 1.43–2.23) after CABG and multiple valve surgery. Combined CABG and multiple valve surgery, heart failure, creatinine 180 μmol/L or greater, alcohol use disorder, dementia and depression were independent risk factors for disability.
Interpretation: The cumulative incidence of disability was lowest after CABG and highest after combined CABG and multiple valve surgery. Our findings point to a need for models that predict personalized disability risk to enable better patient-centred care.
Cardiac surgery is a growing field, with 2 million procedures currently being performed globally each year.1 The last 2 decades have seen important advances in surgical and perioperative care and in improved patient survival.2–4 On the other hand, as patients presenting for surgery become increasingly older and frail, they shift their goals and priorities toward how surgery might affect personal freedom and mobility, rather than longevity alone.5–9 New or residual impairments after surgery are of particular concern to patients and clinicians alike, but the quality and standard of cardiac care has long been assessed by traditional “tombstone” measures such as mortality and major adverse cardiovascular events.5,8,10–12 Patient-centred care represents a priority area for modern medical practice and research, and the facilitation of shared surgical decision-making could be improved by incorporating patient perspectives and patient-derived data.13–15
Our group has recently derived “disability-free survival” as a patient-defined outcome through a large-scale survey of more than 3000 patients with cardiovascular diseases.16 According to patient preferences and values, disability was defined as the composite of stroke, recurrent nonelective hospital admissions and admission to a nursing home.16 Before this outcome measure could be meaningfully used to inform patient-centred decision-making, its epidemiology and impact need to be described first at the population level. We therefore conducted the current study to evaluate disability-free survival after major cardiac surgery in a population-based cohort.
Methods
Design and study population
We conducted a population-based, retrospective cohort study in Ontario, Canada. We included adults residing in Ontario aged 40 years or older and who had undergone CABG, or aortic, mitral or tricuspid valve surgery between Oct. 1, 2008, and Dec. 31, 2016 (Appendix 1, Supplementary Table 1, available at www.cmajopen.ca/content/9/2/E384/suppl/DC1). For those patients who underwent multiple cardiac procedures during the study period, we considered the first procedure to be the index procedure. Exclusion criteria were non-Ontario residency status, those with missing information regarding age and sex, and those who had concomitant arrhythmia, or pulmonic valve or thoracic aorta surgery. During the study period, Ontario was Canada’s most populous province with a publicly funded, universal health care system that reimburses all covered services and providers.
Baseline characteristics, stratified by type of surgery*
Data sources
We used the administrative health care databases from ICES with information on all Ontario residents, and the detailed clinical registry data from CorHealth Ontario. CorHealth Ontario maintains a prospective registry of all patients who undergo invasive cardiac procedures in Ontario. All 20 advanced cardiac hospitals in Ontario participate in the registry. It captures demographic characteristics and comorbidity- and procedural-related information and has been validated through selected chart audits. In addition, ejection fraction and angiographic data in the CorHealth Ontario database undergo core laboratory validation.17
We identified individuals who underwent the specified cardiac procedures from the CorHealth Ontario registry, and linked them deterministically to the ICES administrative databases by using encrypted unique confidential codes. Specifically, we linked the date and type of cardiac procedures, physiologic and comorbidity data from CorHealth Ontario with the Canadian Institute for Health Information’s Discharge Abstract Database (comorbidities and hospital admissions) and Same Day Surgery database (comorbidities), the Ontario Health Insurance Plan database (physician service claims), the Registered Persons Database (ascertainment of vital statistics), the Continuing Care Reporting System (admissions to long-term care facilities) and the Canadian Census. The administrative databases have been validated for many outcomes, exposures and comorbidities, including heart failure, chronic obstructive pulmonary disease, asthma, hypertension, myocardial infarction and diabetes.18–21
Comorbidities
We identified comorbidities from the CorHealth Ontario registry and supplemented the information with data from the Discharge Abstract Database, Same Day Surgery database and Ontario Health Insurance Plan using International Classification of Diseases, 10th Revision codes22 within 5 years before the index procedure, according to validated algorithms.18,20,23–25 We estimated socioeconomic status based on patients’ neighbourhood median income in the Canadian Census, and determined their residence (rural v. urban) using the definitions from Statistics Canada.26 We ascertained emergent procedural status from the CorHealth Ontario registry, as cases requiring operative intervention within 48 hours of acute presentation to hospital. We identified height, weight and body mass index from the CorHealth Ontario registry and used it to define class 3 or severe obesity (weight > 159 kg or body mass index ≥ 40).16,25,27,28 We identified frailty status using the Johns Hopkins Adjusted Clinical Groups frailty-defining diagnoses indicator, which is an instrument that uses administrative data and is designed and validated for research of frailty-related outcomes and use of resources.28–33
Outcomes
The primary outcome was disability, defined as patient-derived composite of stroke, de novo nursing home admission and recurrent nonelective hospital admissions for 3 or more episodes occurring within 1 year of surgery.16 Secondary outcomes consisted of all-cause death and each individual component of disability. We identified stroke requiring hospital admission using a validated algorithm with 70% sensitivity and 99% specificity.34 We ascertained nonelective hospital admissions using the Discharge Abstract Database, and long-term care admissions using the Continuing Care Reporting System.
Statistical analysis
Continuous variables were expressed as mean (standard deviation) and categorical variables as number (proportions). We assessed outcomes through Dec. 31, 2017. Patients were censored when they lost possession of a valid Ontario health insurance card. We defined disability-free survival as survival time from the date of index surgery until the date of a disability-defining event, death or last follow-up, whichever occurred earlier. For patients who had recurrent nonelective hospital admissions, we considered disability to have occurred on the date of the first admission. To account for death as a competing risk, we estimated the cumulative incidence of disability over time using cumulative incidence functions (CIFs), and the relative effect of covariates on the subdistribution hazard using a Fine and Gray model. We explored whether sex had a modifying effect on the relation between disability and type of surgery, by using a multiplicative interaction term of sex × type of surgery within each of the multivariable time-to-event models. Post hoc, we also examined the cumulative incidence of disability, death, and the composite of these end points, as stratified by age.
We performed analyses using SAS 9.4 (SAS Institute), with statistical significance defined by a 2-sided p value of < 0.05. We used the adjusted hazard ratio (HR) and associated 95% confidence intervals (CIs) to describe the measure of association.
Ethics approval
The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a research ethics board.35
Results
The study included 72 824 patients. A flow diagram detailing the process used to select the study cohort is provided in Appendix 1, Supplementary Figure 1. The baseline patient characteristics according to type of surgery are summarized in Table 1. Isolated CABG accounted for 72.2% of the provincial procedure volume. These were most likely to be performed in younger men with a history of previous myocardial infarction and percutaneous coronary intervention, and least likely to have been performed in those with heart failure.
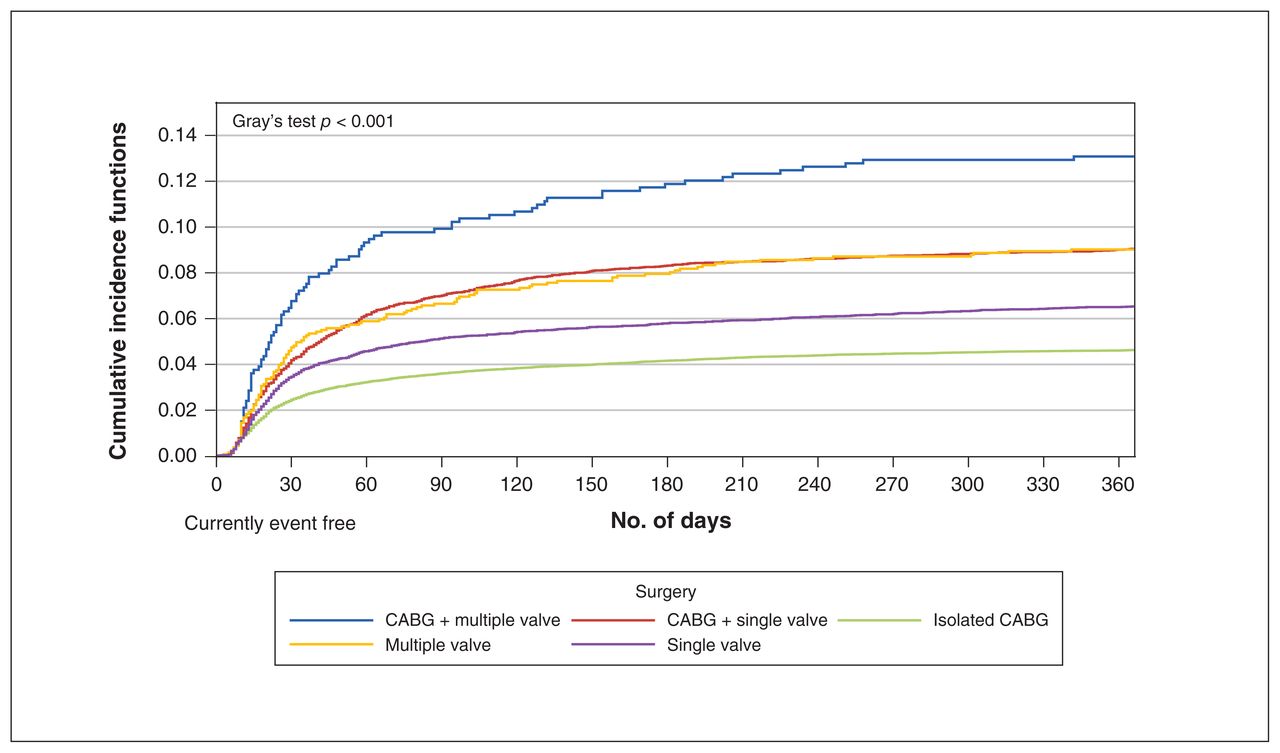
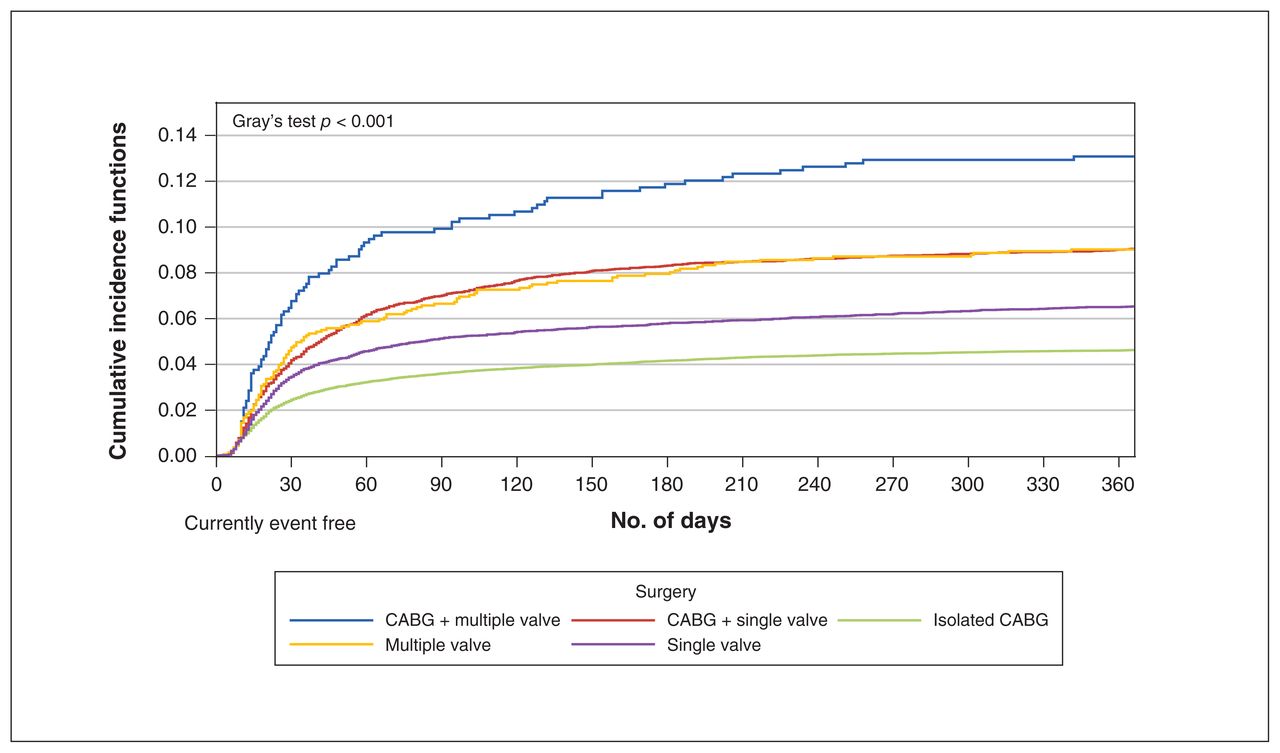
Cumulative incidence of disability within 1 year after cardiac surgery. Note: CABG = coronary artery bypass grafting.
Compared with those who underwent combined CABG and valve procedures, those who underwent isolated valve surgery were younger and were more likely to have preserved left ventricular ejection fraction and a lower burden of comorbidities, as evidenced by a lower Charlson Comorbidity Index. Further, those who underwent combined CABG and multiple valve surgery were among the frailest and burdened with the highest number of comorbidities.
As we did not observe a statistically significant interaction effect between sex and type of surgery (interaction p = 0.07), subsequent analyses were not stratified by sex.
Disability-free survival
Table 2 and Supplementary Table 2 in Appendix 1 summarize the cumulative incidence of disability, death and individual disability-defining events according to surgery type. Graphical representations of these events and their subcomponents are provided by surgery type in Figures 1 and 2, and Supplementary Figures 2–4 in Appendix 1. Figure 3 shows the cumulative incidence of disability, death and the combination of these events for all surgeries.
Cumulative incidence of events within 1 year after cardiac surgery, stratified by type of surgery**

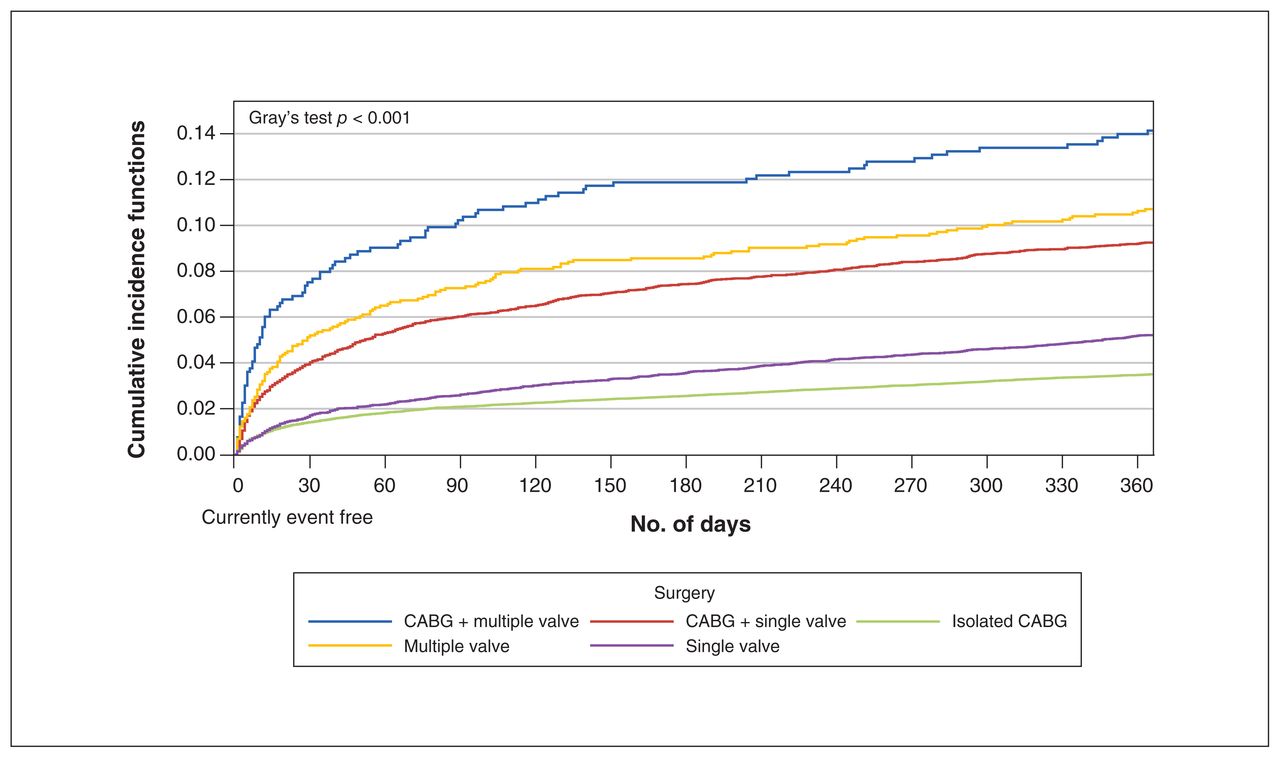
Cumulative incidence of death within 1 year after cardiac surgery. Note: CABG = coronary artery bypass grafting.

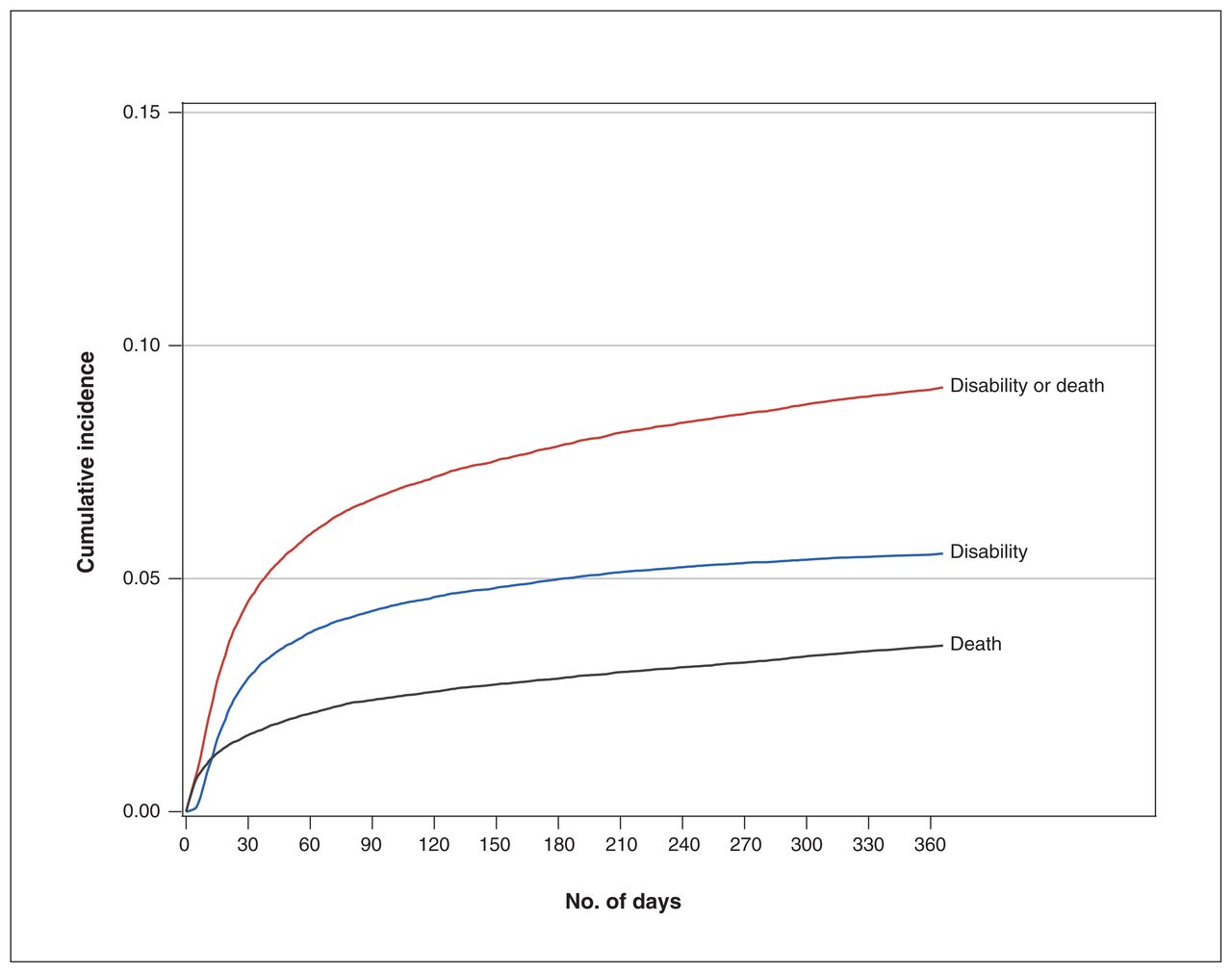
Cumulative incidence of disability, death and the combination of these outcomes at 1 year after cardiac surgery.
The incidence proportions of disability and death were as follows: 2431 (4.6%) versus 1839 (3.5%) in the CABG-only group; 677 (6.5%) versus 540 (5.2%) in the single valve group; 118 (9.0%) versus (10.7%) in the multiple valve group; 718 (9.0%) versus 734 (9.2%) in the CABG and single valve group; and 87 (13.1%) versus 94 (14.1%) in the CABG and multiple valve group. Overall, the 1-year cumulative incidence of disability was lowest in patients who underwent isolated CABG and highest after CABG and multiple valve surgery. Disability occurred more frequently than death in the year after isolated CABG and single valve surgery. Of those who developed disability, 755 (18.7%) subsequently died within the year after surgery.
Disability and patient age
Post hoc, we evaluated the impact of patient age on disability, death and the combination of these events. The cumulative incidence of these events was lowest in adults aged 40–49 years and 50–59 years, and was incrementally higher for each decade above the age of 60 years (Appendix 1, Supplementary Figures 5–7).
Disability-defining events
The cumulative incidence of stroke, recurrent nonelective hospital admissions and long-term care admissions varied by type of surgery (Table 1 and Appendix 1, Supplementary Figures 2–4). Specifically, the rates of all 3 events were lowest after isolated CABG, highest after combined CABG and multiple valve reconstruction, and were similar after multiple valve surgery and CABG combined with single valve surgery.
Disability risk factors
The multivariable predictors of disability are summarized in Table 3. With isolated CABG as the reference group, the adjusted subdistribution HRs for disability were 1.34 (95% CI 1.21–1.48) for single valve, 1.43 (95% CI 1.18–1.75) for multiple valve, 1.38 (95% CI 1.26–1.51) for CABG and single valve, and 1.78 (95% CI 1.43–2.23) for CABG and multiple valve reconstruction. Other statistically significant risk factors of disability were age, female sex, emergent operative status, low income, a history of hypertension, atrial fibrillation, myocardial infarction, heart failure, cerebrovascular disease, peripheral arterial disease, current smoker, chronic obstructive pulmonary disease, diabetes, anemia, renal insufficiency, liver disease, alcohol use disorder, dementia, depression and cancer. Of these, CABG and multiple valve surgery, heart failure, baseline creatinine 180 μmol/L or greater, alcohol use disorder, dementia and depression were the most clinically significant predictors of disability.
Multivariable predictors of disability at 1-year after major cardiac surgery
Interpretation
In this population-based study, we systematically described the incidence and risk factors of patient-defined disability after common cardiac procedures. We found that the cumulative incidence of disability was lowest after isolated CABG and highest after CABG and multiple valve surgery. Disability occurred more frequently than death in the year after isolated CABG and single valve surgery. Combined CABG and multiple valve surgery, heart failure, baseline creatinine 180 μmol/L or greater, alcohol use disorder, dementia and depression were important predictors of disability in the year after cardiac surgery.
Traditional revascularization trials have sometimes been referred to as “tombstone trials”6 because of their focus on death and complications. However, a survey of cardiovascular patients indicated that important outcomes identified by patients were in fact very different compared with those from the clinician’s view.16 Our findings suggest that most patients who experience disability after cardiac surgery will continue to live with disability. Thus, the incorporation of patient perceptions and values into the design of outcome measures has been proposed as a priority area for cardiovascular research. Such a paradigm shift has been shown to increase the relevance of the research to the end user, speed up the uptake of research into practice and empower patients to make better-informed decisions.36
To date, few studies have directly engaged surgical patients to determine what outcomes were meaningful to them, as important end users of the research. Such studies include surveys of noncardiac surgery patients to rank outcomes such as postoperative nausea, vomiting, pain and somnolence in order of unpleasantness,37–39 but similar research has not been conducted in the realm of cardiac surgery. “Patient-centred” cardiac surgery research has instead employed standard, clinician-derived instruments (e.g., Seattle Angina Questionnaire, Rose Dyspnea Scale and Patient Health Questionnaire) that were based on expert consensus alone, without active input from patients.40 These standard instruments may not be meaningful to all patients as they do not capture all relevant aspects of outcomes after treatment.41 Outcomes are an important determinant of treatment satisfaction, and the use of patient-defined outcomes has the unique advantage of improving both patient satisfaction and adherence to treatment.
There is no universal agreement on the definition of disability in cardiovascular research.11 Prospective studies using clinician-derived instruments are often limited by small sample size and short follow-up durations, within a single centre setting. In the present study, we used a new and versatile definition of disability based on patient preferences,16 which is adaptable to both prospective trials and large retrospective cohorts. Knowledge generated from this broad epidemiologic study will inform areas of focus for practice-changing research in the future.
CABG is an advancing field in which operative mortality has steadily declined over the years.42 This, together with the younger age of presentation for CABG, could explain the lower observed rates of disability after this procedure as compared with complex CABG and multiple valve procedures, which are often performed on older and frailer patients. Complex surgery is associated with greater physiologic stresses such as fluid and electrolyte shifts, prolonged bypass durations, and a higher likelihood of exposure to low cardiac output, hypotension, end organ injury and death.43
Single valve surgery, which constitutes mostly operations on the aortic and mitral valves, was associated with a higher incidence of disability than CABG. This observation could be explained by the fact that although patients requiring aortic valve surgery are a mixed population of younger, healthier (e.g., congenital bicuspid aortic valve) and older, sicker candidates (e.g., degenerative aortic valve disease), patients who undergo isolated mitral valve surgery are generally younger, with fewer comorbidities. In contrast, patients who undergo CABG often have other substantial comorbidities that coexist with coronary artery disease to affect their outcomes adversely.
To date, disability after cardiac surgery has been reported in the form of health-related quality of life, using instruments such as the Medical Outcomes Study 36-item Short Form (SF-36),44 in several small observational studies. In a single-centre study of 112 patients, patients reported higher than normative scores in subscales of social functioning, role physical and role emotional; and lower scores in physical function, bodily pain, general health, vitality social function and mental health at 1 year after CABG.45 In a study of 534 consecutive patients aged 75 years and older who had undergone cardiac surgery, mean reported quality of life improved at 6 months postoperatively as compared with that at baseline.46 In a study of 154 nonagenarians who underwent CABG or valve procedures, 83% of the survivors reported an improvement in quality of life and 4% a decline in quality of life 1 year after surgery.47
Our findings show that the incidence of patient-defined disability may be greater than that previously described by traditional instruments. Moreover, we were able to describe the population-based incidence of disability by type of surgery and across a wider patient age range. We found that the burden of disability was higher than death after routine procedures such as isolated CABG and single valve surgery, and these findings were driven mostly by recurrent hospital admissions, followed by stroke, especially in those with heart failure, renal dysfunction, alcohol use disorder, dementia and depression. As patients’ ability to make informed decisions is often influenced by the emotional and logistical repercussions of their disease diagnosis and limitations in health literacy, patients with these high-risk features should be the focus of informed perioperative counselling and undergo formal heart-team evaluation regarding the risks and benefits of alternative treatment strategies.
Limitations
Although it is possible that we attributed outcomes to the index surgery that may be a consequence of repeat surgery, having a repeat procedure within 1 year of index cardiac surgery is rare. In the present study, of a total of 4031 patients who developed disability during the year after surgery, only 145 (3.6%) had a repeat cardiac procedure before the onset of disability. Repeat procedures may be viewed as a moderator of disability, as patients who are prone to developing disability are also prone to procedure failure.
This study has several limitations. Data pertaining to stroke severity are unavailable in the databases used. As some patients who have a stroke experience full functional recovery, our findings may have overestimated the burden of stroke-related disability. Our definition of disability was based solely on patient perceptions and values. Further studies could aim to elicit feedback from family members and caregivers as well to codefine outcomes, with input and guidance from clinicians. We were unable to incorporate or validate our disability outcome with commonly used clinical disability assessment tools, as our definition of disability is limited by what is available in administrative data. Finally, cohort studies are by nature subject to residual confounding.
Conclusion
We studied the procedure-specific incidence of a patient-defined disability outcome in a large cohort of cardiac surgical patients. We found disability to be a more frequent complication than death in the year after isolated CABG and single valve surgeries. In addition, patients who undergo combined CABG and multiple valve surgery, and those who have a history of heart failure, baseline creatinine 180 μmol/L or greater, alcohol use disorder, dementia and depression are at the greatest risk for developing disability. Future research should be dedicated to personalized disability risk prediction to inform better the joint therapeutic decision-making process and, in doing so, to improve the efficiency and effectiveness of health care delivery as well as patient satisfaction.
Acknowledgement
This study is supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). The authors acknowledge that the clinical registry data used in this analysis is from participating hospitals through CorHealth Ontario, which serves as an advisory body to the MOHLTC, is funded by the MOHLTC, and is dedicated to improving the quality, efficiency, access and equity in the delivery of the continuum of adult cardiac and stroke care in Ontario, Canada. The authors also acknowledge the usage of data compiled and provided by the Canadian Institute for Health Information. These data sets were linked using unique encoded identifiers and analyzed at ICES.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Louise Sun contributed to conception and design of the study. Louise Sun and Anan Bader Eddeen contributed to data acquisition and analysis. Louise Sun, Anan Bader Eddeen and Thierry Mesana contributed to interpretation of data. Louise Sun drafted the work and Louise Sun, Anan Bader Eddeen and Thierry Mesana revised it critically for important intellectual content. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Data sharing: The data set from this study is held securely in coded form at ICES. Although data sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at https://www.ices.on.ca/DAS.
Funding: The authors acknowledge support from an operating grant from the Canadian Institutes of Health Research (Grant #4752). Louise Sun was named Heart and Stroke Foundation of Canada National New Investigator and is supported by the University of Ottawa Tier 2 Clinical Research Chair in Big Data and Cardiovascular Outcomes and the Ottawa Heart Institute Research Corporation.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/9/2/E384/suppl/DC1.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2021 Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- Derivation and validation of pragmatic clinical models to predict hospital length of stay after cardiac surgery in Ontario, Canada: a population-based cohort study
- Derivation and validation of a clinical risk score to predict death among patients awaiting cardiac surgery in Ontario, Canada: a population-based study
- Derivation and validation of a clinical model to predict death or cardiac hospitalizations while on the cardiac surgery waitlist