


Abstract
Background: In 2010, HIV treatment as prevention (TasP), encompassing widespread HIV testing and immediate initiation of free antiretroviral treatment (ART), was piloted under the Seek and Treat for Optimal Prevention of HIV/AIDS initiative (STOP) in British Columbia, Canada. We compared the time from HIV diagnosis to treatment initiation, and from treatment initiation to first virologic suppression, before (2005–2009) and after (2010–2016) the implementation of STOP.
Methods: In this population-based cohort study, we used longitudinal data of all people living with an HIV diagnosis in BC from 1996 to 2017. We included those aged 18 years or older who had never received ART and had received an HIV diagnosis in the 2005–2016 period. We defined the virologic suppression date as the first date of at least 2 consecutive test results within 4 months with a viral load of less than 200 copies/mL. Negative binomial regression models assessed the effect of STOP on the time to ART initiation and suppression, adjusting for confounders. All p values were 2-sided, and we set the significance level at 0.05.
Results: Participants who received an HIV diagnosis before STOP (n = 1601) were statistically different from those with a diagnosis after STOP (n = 1700); 81% versus 84% were men (p = 0.0187), 30% versus 15% had ever injected drugs (p < 0.0001), and 27% versus 49% had 350 CD4 cells/μL or more at diagnosis (p < 0.0001). The STOP initiative was associated with a 64% shorter time from diagnosis to treatment (adjusted mean ratio 0.36, 95% confidence interval [CI] 0.34–0.39) and a 21% shorter time from treatment to suppression (adjusted mean ratio 0.79, 95% CI 0.73–0.85).
Interpretation: In a population with universal health coverage, a TasP intervention was associated with shorter times from HIV diagnosis to treatment initiation, and from treatment initiation to viral suppression. Our results show accelerating progress toward the United Nations’ 90-90-90 target of people with HIV who have a diagnosis, those who are on antiretroviral therapy and those who are virologically suppressed, and support the global expansion of TasP to accelerate the control of HIV/AIDS.
The personal and public health benefits of early initiation of antiretroviral treatment (ART) are well documented.1–5 In addition to decreasing morbidity and mortality rates among people living with HIV/AIDS,1–3 ART has also been shown to reduce the incidence of HIV cases in a population.4,5 This evidence led to the conception of HIV treatment as prevention (TasP), the scaling-up of testing followed by the immediate initiation of ART, as a strategy for reducing AIDS-related morbidity and death, as well as the spread of HIV.6–8 The success of TasP for HIV transmission relies on the ART-led suppression of HIV replication, resulting in sustained undetectable viral load in bodily fluids and a risk of sexual transmission of HIV that is effectively zero — referred to as “undetectable = untransmissible” (U=U).9,10
To achieve the goal of ending AIDS as a pandemic by 2030, the United Nations Joint AIDS Programs (UNAIDS) proposed the TasP-based 90-90-90 target, whereby at least 90% of people living with HIV have a diagnosis, 90% of people with an HIV diagnosis are treated with ART and 90% of ART-treated people living with HIV are virologically suppressed by 2020.11 Meeting the 90-90-90 target would result in a substantial decrease in AIDS-related morbidity and mortality rates and new HIV infections within a decade.12,13 The global progress toward the 90-90-90 target has been encouraging, despite political, fiscal and programmatic challenges.14–18
In British Columbia, Canada, TasP was piloted in 2010 and subsequently expanded across the province under the publicly funded Seek and Treat for Optimal Prevention of HIV/AIDS initiative (STOP). The STOP initiative used TasP as a framework to address the HIV care continuum, including widespread HIV testing, immediate ART initiation, public health follow-ups for care interruptions and targeted community outreach.19 By 2016, BC achieved a ratio of 84-85-93,20 and by December 2020, BC surpassed the 90-90-90 target.21
Evidence-based strategies that improve HIV clinical outcomes in a timely manner are needed to inform future prevention and care efforts. As such, we aimed to assess the population-level impact of a TasP intervention in accelerating the progression toward the UNAIDS 90-90-90 target by comparing the time from HIV diagnosis to ART initiation, and, among those who achieved suppression, the time from ART initiation to virologic suppression, before and after the implementation of STOP (2005–2009 and 2010–2016, respectively). To evaluate whether STOP affected various population subgroups equally, we further stratified analyses of both outcomes by demographic and clinical characteristics.
Methods
Study design and setting
We conducted a retrospective population-based cohort study using a province-wide HIV clinical registry and administrative health data in BC. The BC Centre for Excellence in HIV/AIDS Drug Treatment Program has been responsible for ART distribution in the province since 1992.22 Antiretroviral therapy and routine laboratory monitoring (including plasma viral load and CD4 cell counts) are free of charge for all people living with HIV. BC’s HIV therapeutic guidelines provide guidance for ART eligibility, including minimum CD4 thresholds to initiate ART, which have evolved from 200 cells/μL before 2008 to 350 cells/μL in 2008 and 500 cells/μL in 2010.23 Since 2012, ART has been prescribed regardless of CD4 count. The recommended first-line ART regimens in these guidelines have also evolved.23 Credited with faster virologic suppression and reduced drug resistance, 24,25 integrase strand-transfer inhibitor–based ART has been available in BC as a first-line therapy option since 2011 for raltegravir, 2013 for elvitegravir and 2014 for dolutegravir.
The STOP initiative was piloted on Feb. 4, 2010, in 2 major urban areas where more than 50% of people living with HIV in BC resided and with the highest HIV-related mortality rates.19 During this pilot phase, STOP supportive services were also available to people living with HIV from all over BC who sought care in these urban areas, making STOP readily available to at least 80% of the BC population. The expansion of STOP and its relevant infrastructure to the rest of the province occurred shortly after the pilot began and was completed on Apr. 1, 2013. In this study, we chose the start of the pilot phase, which was the official implementation date of the STOP initiative, as the beginning of our post-STOP period.
Participants
Eligible participants included adults (aged ≥ 18 yr) living with HIV who were diagnosed in BC between Jan. 1, 2005, and Dec. 31, 2016, and who initiated ART for the first time through the Drug Treatment Program. Limiting the HIV diagnosis period to 2005 to 2016 allowed for a balanced number of participants who received their HIV diagnosis before and after the implementation of STOP. The date of the latest available data linkages from the STOP cohort for our study was Mar. 31, 2017.
Data sources
We obtained individual-level longitudinal data of all people living with HIV in BC who received their HIV diagnosis between April 1996 and March 2017 from the STOP population-based cohort.26 The cohort was constructed by linking the Drug Treatment Program’s clinical registry22 and various provincial administrative data sets26–31 that provided demographic, clinical, laboratory, health care utilization and treatment information. Relevant data stewards performed the linkages by matching individuals’ personal provincial health numbers, which were provided at birth or through immigration. The aforementioned data linkages and corresponding data capture are detailed in Appendix 1, Appendix Table 1, available at www.cmajopen.ca/content/10/1/E27/suppl/DC1).
Characteristics of people living with HIV in British Columbia from 2005 to 2016 included in the study and in each analysis*
Outcomes and exposures
Our outcomes were time from HIV diagnosis to ART initiation and from ART initiation to first virologic suppression. Our exposures were the eras of HIV diagnosis and ART initiation, each grouped into pre-STOP (2005–2009) and post-STOP (2010–2016).
Diagnosis date was the first instance of a positive HIV antigen–antibody test, a detectable plasma viral load, an HIV-related hospitalization, 3 HIV-related physician visits, an AIDS-defining illness, or ART dispensation, as previously validated. 32 AIDS-defining illnesses included indicator diseases specified by the BC Centre for Disease Control,33 and are outlined in Appendix 1, Appendix Table 2. We obtained the ART initiation date from the Drug Treatment Program.
We defined the virologic suppression date as the first instance of at least 2 consecutive test results within 4 months with a plasma viral load of less than 200 copies/mL, a conservative definition that we selected by taking into account the quantification range of plasma viral load assays during our study period. We excluded people living with HIV with less than 4 months of follow-up upon ART initiation who were therefore unable to meet the virologic suppression definition, and those who did not achieve suppression during the study period from the analysis of time from treatment to virologic suppression.
Confounders
We investigated the following potential confounders, selected based on relevance and availability of data: gender (women, men), age (< 30, 30–39, 40–49, ≥ 50 yr), health authority of residence (Fraser, Interior, Northern, Vancouver Coastal, Vancouver Island, unknown), CD4 count (< 200, 200–349, ≥ 350 cells/mm3, unmeasured), ethnicity (white, non-white, unknown) and risk group for HIV acquisition (gay, bisexual and other men who have sex with men; people who have ever injected drugs; heterosexual or other; unknown).
We collected age, health authority of residence and CD4 count at time of diagnosis and at time of ART initiation. For analysis of the time from treatment to viral suppression, we also assessed additional treatment-related potential confounders, measured at ART initiation, namely plasma viral load (continuous in log10 copies/mL) and first-line ART class (non-nucleoside reverse transcriptase inhibitor, protease inhibitor, integrase strand-transfer inhibitor, integrase strand-transfer inhibitor combined with non-nucleoside reverse transcriptase inhibitor and/or protease inhibitor, other). We used the CD4 count closest to (within a year before) the diagnosis and ART initiation dates, respectively. If unavailable, we chose the closest CD4 count measured within 3 months after these dates. We applied similar criteria when establishing plasma viral load at ART initiation. To accommodate differential quantification limits across monitoring assays for viral load,34 we categorized all values of less than 50 copies/mL as 49 copies/mL and values over 100 000 copies/mL as 100 010 copies/mL.
Statistical analysis
We explored the annual trends (2005–2016) in time from diagnosis to treatment, and from treatment to viral suppression. We also evaluated the distribution of the 2 outcomes pre- and post-STOP, across gender, age, health authority of residence, CD4 count, ethnicity and HIV acquisition risk groups to account for population subgroup differences. Lastly, we estimated the relative effects of STOP on time from diagnosis to treatment, and from treatment to viral suppression, adjusted for confounders.
We compared categorical variables using the Fisher exact test or χ2 test, and compared continuous variables using the Kruskal–Wallis test.35 We modelled the overdispersed time from diagnosis to treatment and from treatment to viral suppression using a negative binomial regression model.36 Starting with a full model, we gradually omitted confounding variables until the change in the coefficient for the main explanatory variable was 5% or more.37 We modelled time from diagnosis to treatment and from treatment to viral suppression in days, although for descriptive purposes and ease of reading, we converted these to months. All p values are 2-sided, and we set the significance level at 0.05. We performed analyses in SAS version 9.4 and R version 3.6.0.
Ethics approval
Linkage and usage of administrative databases were approved and performed by data stewards in each collaborating agency and facilitated by the BC Ministry of Health. The University of British Columbia Ethics Review Committee at the St. Paul’s Hospital site provided ethics approval for this study (H18-02208). This study was conducted using strictly anonymized laboratory and administrative databases, and thus informed consent was not required. This study complies with BC’s Freedom of Information and Protection of Privacy Act.
Results
Of the 3301 eligible people in BC living with HIV who received their diagnosis in 2005–2016, 2719 (82%) were men, 1906 (58%) were aged 30 to 49 years old, 1831 (55%) were white, 1690 (51%) were residents of the Vancouver Coastal health authority, 1259 (38%) had a CD4 count of less than 350 cells/μL at diagnosis, and 1359 (41%) were part of the risk group of gay, bisexual and other men who have sex with men (Table 1). Those diagnosed pre-(n = 1601, 49%) and post-STOP (n = 1700, 51%) were significantly different in all demographic and clinical characteristics except for ethnicity.
Of the 2979 (90%) people living with HIV who achieved viral suppression, those who initiated ART pre- (n = 998, 34%) and post-STOP (n = 1981, 66%) were statistically significantly different on all characteristics except gender, ethnicity and health authority of residence. Of the 322 (10%) people living with HIV who were excluded from the analysis of time from treatment to viral suppression, 114 did not have the required minimum 4 months of follow-up, and 208 did not achieve suppression within the study period (median follow-up 2 [25th, 75th percentile (Q1, Q3) 1, 3] mo v. median follow-up 22 [Q1 8, Q3 43], mo respectively).
Time from HIV diagnosis to treatment initiation
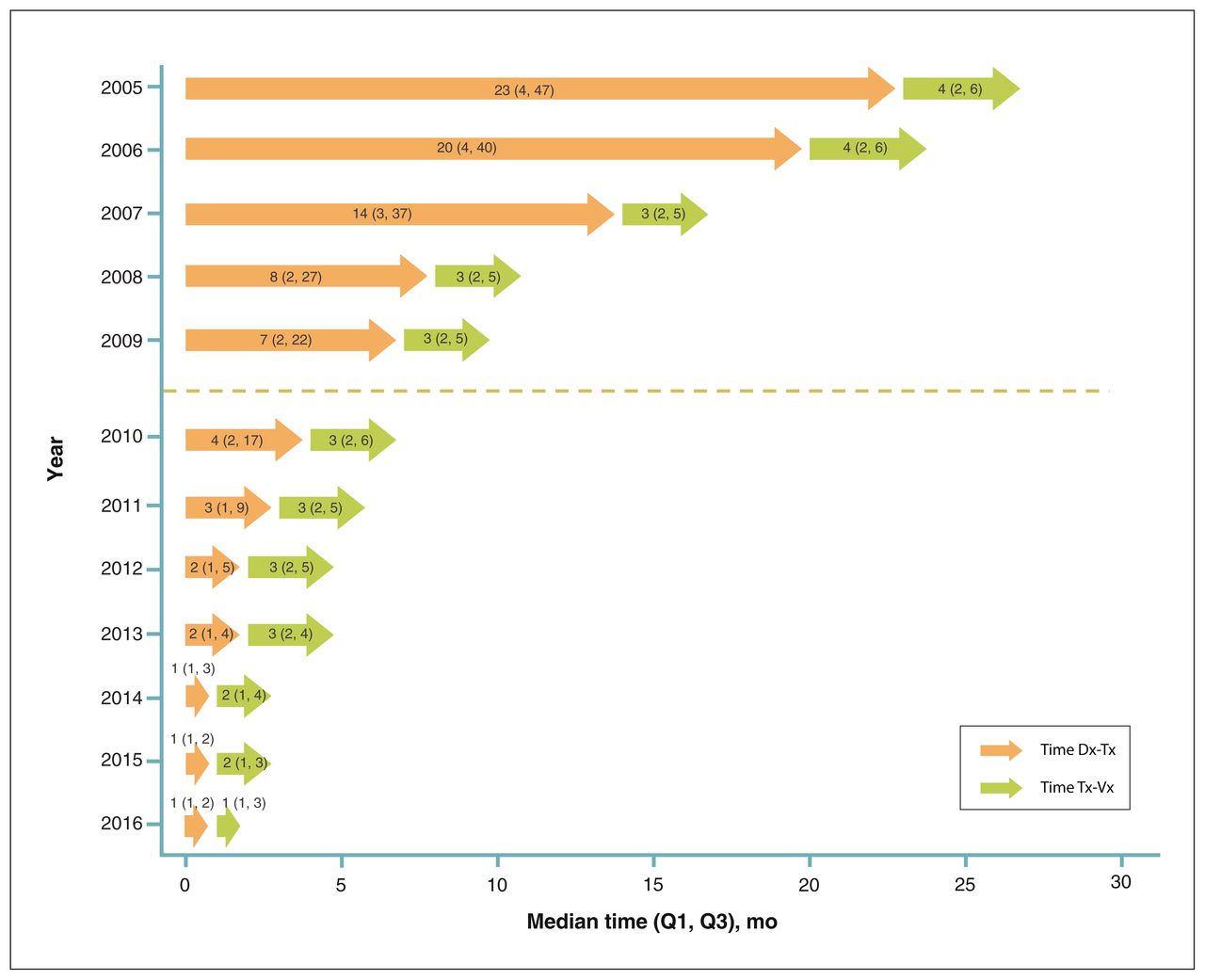
The median time from HIV diagnosis to ART initiation declined from 23 (Q1 4, Q3 47) months in 2005 to 1 (Q1 1, Q3 2) month in 2016 (Figure 1). The decline in time from diagnosis to treatment before and after STOP was statistically significant across all population subgroups (Appendix 2, available at www.cmajopen.ca/content/10/1/E27/suppl/DC1). Additionally, the gaps in time from diagnosis to treatment across age, CD4 count and HIV acquisition risk groups narrowed after the implementation of STOP. For instance, before STOP, the median time from diagnosis to treatment among people younger than 30 years old was 20 months longer than those aged 50 years and older. After STOP, people living with HIV across all age groups initiated ART within a median of 2 months. After adjusting for CD4 count at diagnosis, the time from diagnosis to treatment was, on average, 64% shorter after STOP (adjusted mean ratio 0.36, 95% confidence interval [CI] 0.34–0.39) than before STOP.

The distribution of time from HIV diagnosis to initiation of antiretroviral treatment (time Dx-Tx) and from HIV treatment initiation to viral suppression (time Tx-Vx) among people living with HIV in British Columbia from 2005 to 2016. Time is in months, presented as median, with 25th and 75th percentiles (Q1, Q3). The dotted line represents the implementation date of the Seek and Treat for Optimal Prevention of HIV/AIDS initiative on Feb. 4, 2010.
Time from treatment initiation to viral suppression
The annual median time from treatment to viral suppression declined from 4 (Q1 2, Q3 6) months in 2005 to 1 (Q1 1, Q3 3) month in 2016; people who initiated ART in 2007 to 2013 achieved suppression within a steady median of 3 months (Figure 1). The decline in time from treatment to viral suppression before and after STOP was statistically significant, except among women, residents of the Northern health authority and those initiating ART with 200 to 349 CD4 cells/μL (Appendix 2). After the initiation of STOP, residents of the Northern health authority and people who had ever injected drugs had the longest median time from treatment to viral suppression at 4 (Q1 2, Q3 9) months. On average, after adjusting for health authority of residence, CD4 count at ART initiation, HIV acquisition risk group and type of first-line ART, STOP was associated with a 21% shorter time from treatment initiation to viral suppression (adjusted mean ratio 0.79, 95% CI 0.73–0.85).
Interpretation
Within our universal health care setting, a TasP intervention was strongly associated with earlier ART initiation and shorter time to virologic suppression. Even when adjusted for changes in ART eligibility, first-line ART preferences and other confounders, the TasP intervention implemented in BC was associated with a 64% shorter time from diagnosis to treatment and a 21% shorter time from treatment to suppression.
Observational studies from the Netherlands, South Korea, Thailand and New York City also reported a significant decrease in time from HIV diagnosis to treatment initiation in the 2012 to 2015 period,38–41 when international guidelines began to recommend rapid ART initiation independent of CD4 count.42–46 By 2015, however, 75% of people living with HIV in BC initiated ART within 2 months of their diagnosis, compared with 6 months, as noted in the other observational studies.38–41 Although the independent impact of STOP in accelerating time from HIV diagnosis to treatment in BC was evident, the full public benefit of early ART to reduce transmission risk requires a decline in another, more complex, time component, namely time from infection to diagnosis. Delayed HIV diagnosis has previously been observed in 1 in 7 people living with HIV in BC, particularly those who were older, were heterosexual, had ever injected drugs and resided in the Northern health authority.47 This reality argues for targeted interventions to improve HIV screening among the identified populations.
During our study period, other North American cohort studies also reported shorter times from treatment initiation to viral suppression.48,49 Others reported faster suppression from the time of diagnosis,50–56 which can be driven by shorter time from diagnosis to treatment or from treatment to viral suppression. In 2016, BC’s combined median time from diagnosis to suppression was up to 2 months faster than that observed in several US jurisdictions.54,55 Although our annual trends signalled that regimens using integrase strand-transfer inhibitors likely contributed to the faster decline in time from treatment to viral suppression, our multivariable model corroborated the independent impact of STOP.
In the present U=U era, a shortened time to achieve suppression is a critical measure of HIV care success.57,58 This assertion urges population-wide improvements in key risk factors of virologic suppression, such as removing barriers to ART adherence, reducing substance use and managing mental health disorders.59–61 Our study showed BC’s remarkable progress on rapid viral suppression by 2016, but further studies should investigate how the COVID-19 pandemic may affect this progress. Interrupted health care access, medication disruption and psychological stress from self-isolation and income loss are among additional challenges faced by people living with HIV during this pandemic, threatening progress on the control of HIV/AIDS.62–65 Our study indicated potential disparities in the impact of STOP on early ART initiation across gender and health authority of residence. Further studies should explore specific barriers that may prevent population subgroups, such as women and residents of the Northern health authority, from receiving the full benefits of STOP.
Limitations
Administrative health data are susceptible to coding errors. We thus used validated case-finding algorithms, specifically developed to ascertain HIV diagnosis dates in administrative data sets. Our lack of granular data on ethnicity limited our ability to assess ethnic disparities in our outcomes fully. However, a recent study found no difference in HIV treatment outcomes between Indigenous and non-Indigenous people living with HIV who injected drugs in BC.66
We were able to assess only the overall impact of STOP, and not the individual impact of STOP’s various supportive services. We did not distinguish STOP’s pilot and full rollout phases, and thus our findings represented the overall impact of the implementation of STOP initiative. Our data availability and structure rendered us unable to evaluate smaller time intervals. Consequently, although we found strong associations between STOP and faster ART initiation and virologic suppression, we were unable to separate the role of STOP and the role of time (i.e., other management and policy changes). A small proportion (2%–24%) of data on CD4 count, HIV acquisition risk group, health authority and ethnicity were unknown or unmeasured, which may minimally affect our findings.
People who recently received an HIV diagnosis may have achieved virologic suppression after the administrative censoring date of Mar. 31, 2017, and were thus excluded from the analysis of time from treatment initiation to viral suppression. Given the high suppression rates, the impact of this administrative censoring on our findings should be minimal. Our data were limited to this administrative censoring date. Nevertheless, given that ART eligibility has not changed between 2017 and the present, our findings remain valuable in elucidating STOP’s contribution in optimizing the HIV care continuum.
Conclusion
Our large population-based study offers empirical evidence of the impact of a TasP intervention in accelerating the progress of BC toward the UNAIDS 90–90–90 target, in that the intervention was strongly associated with earlier ART initiation and shorter time to virologic suppression. These findings support the continued expansion of sustainable and equitable TasP-based policy and programmatic efforts that target underserved and hard-to-reach populations as key tools to reduce AIDS-related morbidity and mortality rates, as well as HIV transmission rates further, and thus alleviate the overall global burden of HIV/AIDS.
Acknowledgements
The authors thank all the participants included in STOP HIV/AIDS, as well as the British Columbia Centre for Excellence in HIV/AIDS, the BC Ministry of Health and the institutional data stewards for granting access to the data.
Footnotes
Competing interests: Julio Montaner has received institutional grants from Gilead Sciences and Merck. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Ni Gusti Ayu Nanditha and Viviane Lima conceived and designed the study. Xinzhe Dong, Hiwot Tafessu, Lu Wang, Michelle Lu and Viviane Lima contributed to acquisition, analysis and interpretation of the data. Ni Gusti Ayu Nanditha and Viviane Lima drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This work was supported by the Public Health Agency of Canada and the British Columbia Ministry of Health, paid to the institution in support of Julio Montaner’s Treatment as Prevention research. Viviane Lima is funded by grants from the Canadian Institutes of Health Research (PJT-148595 and PJT-156147), and the Canadian Foundation for AIDS Research (CANFAR Innovation Grant – 30-101). Ni Gusti Ayu Nanditha is supported by the Canada Graduate Student Master’s Award from the Canadian Institutes of Health Research and the University of British Columbia’s Four-Year Doctoral Fellowship.
Disclaimer: The sponsors had no role in the design, data collection, data analysis, data interpretation or writing of the report. All inferences, opinions, and conclusions drawn in this manuscript are those of the authors, and do not reflect the opinions or policies of the data stewards.
Data sharing: The British Columbia Centre for Excellence in HIV/AIDS is prohibited from making individual-level data available publicly because of provisions in service contracts, institutional policy and ethical requirements. To facilitate research, such data are available via data access requests. Some data are not available externally because of prohibitions in service contracts with funders or data providers. Institutional policies stipulate that all external data requests require collaboration with a British Columbia Centre for Excellence in HIV/AIDS researcher. For more information or to make a request, please contact Mark Helberg, Senior Director, Internal and External Relations, and Strategic Development at mhelberg{at}bccfe.ca. The underlying analytical codes are available by request to the authors.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/10/1/E27/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/.
References
- © 2022 CMA Impact Inc. or its licensors
In this issue

{kind=link}
Article tools


