


Abstract
Background: The COVID-19 pandemic has led to an increase in telemedicine use. We compared care and outcomes in patients with transient ischemic attack (TIA) or minor ischemic stroke before and after the widespread adoption of telemedicine in Ontario, Canada, in 2020.
Methods: In a population-based cohort study using linked administrative data, we identified patients with TIA or ischemic stroke discharged from any emergency department in Ontario before the widespread use of telemedicine (Apr. 1, 2015, to Mar. 31, 2020) and after (Apr. 1, 2020, to Mar. 31, 2021). We measured care, including visits with a physician, investigations and medication renewal. We compared 90-day death before and after 2020 using Cox proportional hazards models, and we compared 90-day admission using cause-specific hazard models.
Results: We identified 47 601 patients (49.3% female; median age 73, interquartile range 62–82, yr) with TIA (n = 35 695, 75.0%) or ischemic stroke (n = 11 906, 25.0%). After 2020, 83.1% of patients had 1 or more telemedicine visit within 90 days of emergency department discharge, compared with 3.8% before. The overall access to outpatient visits within 90 days remained unchanged (92.9% before v. 94.0% after; risk difference 1.1, 95% confidence interval [CI] −1.3 to 3.5). Investigations and medication renewals were unchanged. Clinical outcomes were also similar before and after 2020; the adjusted hazard ratio was 0.97 (95% CI 0.91 to 1.04) for 90-day all-cause admission, 1.06 (95% CI 0.94 to 1.20) for stroke admission and 1.07 (95% CI 0.93 to 1.24) for death.
Interpretation: Care and short-term outcomes after TIA or minor stroke remained stable after the widespread implementation of telemedicine during the COVID-19 pandemic. Our findings suggest that telemedicine is an effective method of health care delivery that can be complementary to in-person care for minor ischemic cerebrovascular events.
Rapid-access clinics to evaluate patients with minor stroke or transient ischemic attack (TIA) discharged from an emergency department are the mainstay of strategies for secondary stroke prevention.1,2 Such patients are usually not admitted to hospital, but they are at high risk of experiencing a disabling stroke in the following days or weeks.3–5 The COVID-19 pandemic has disrupted outpatient clinic-based care and has created a need for telemedicine as an alternative to in-person visits.6
Before the pandemic, telemedicine for stroke in Ontario was largely limited to the Ontario Telestroke Program, which provides support for hyperacute stroke management of patients seen in the emergency departments of primary stroke centres.7 Some outpatient telemedicine care was used for patients living in remote regions with the support of an intermediary host site (e.g., nursing station or clinic) and a clinician facilitating the visit. A small number of direct-to-patient telemedicine outpatient visits took place via the pilot Ontario Virtual Care Program, in which a limited number of physicians obtained special approval to participate.8 At the pandemic onset, as in many other jurisdictions internationally, new physician fee codes for outpatient telemedicine care were introduced in Ontario, Canada (population 14.5 million), allowing for widespread direct-to-patient telemedicine care without the need for additional approval.
We used the opportunity created by the COVID-19 pandemic to compare care and outcomes in patients who were discharged from an emergency department with TIA or ischemic stroke before and after the widespread implementation of direct-to-patient telemedicine visits. We hypothesized that telemedicine could successfully maintain the quality of stroke prevention care and outcomes.
Methods
In this cohort study using linked administrative data, we identified community-dwelling adult Ontario residents who were discharged alive from any emergency department in Ontario without hospital admission with a most responsible diagnosis of TIA (G45.x except G45.4) or ischemic stroke (H34.1, I63.x, I64.x) before and after the implementation of the direct-to-patient telemedicine fee codes.9,10
Setting
Ontario residents have access to physician and hospital visits funded publicly by the Ontario Ministry of Health. Between Mar. 14 and Apr. 1, 2020, a series of new physician fee codes for video or telephone visits were announced by the ministry. 11,12 Physician reimbursement remained unchanged for services provided in person or via telemedicine. We used physician billing codes to track in-person versus telemedicine care13 and defined the pretelemedicine period as Apr. 1, 2015, to Mar. 31, 2020, and the telemedicine period as Apr. 1, 2020, to Mar. 31, 2021.
Outcomes
The main clinical outcomes of interest were all-cause admission, admission for stroke (ischemic and hemorrhagic) and death within 90 days of the emergency department discharge date. We described care by comparing the pretelemedicine and telemedicine periods, including the frequency of in-person or telemedicine visits with a family physician or stroke specialist (neurologist, internist, cardiologist or geriatrician) within 28 days and 90 days of emergency department discharge; investigations, including neuroimaging, vascular imaging and echocardiogram studies; and, for patients older than 65 years, renewal of baseline anti-hypertensive, anti-hyperlipidemia or anti-hyperglycemic medications within 100 days of the emergency department visit. Neuroimaging is defined as imaging with computed tomography (CT) or magnetic resonance imaging (MRI) of the head. Vascular imaging is defined as vessel imaging with carotid Dopplers, CT angiography or MRI angiography. We show neuroimaging and vascular imaging performed during the emergency department visit and within 14 days of the emergency department visit, including imaging performed in the emergency department, separately because the timing of neurovascular imaging is highly relevant in the management of TIA.14 We defined baseline medication as any prescription filled between 100 days before the emergency department visit and up to 7 days after the visit. We chose this definition to capture active medications, but we acknowledge that we may have missed some medications with longer intervals between dispensations. See Appendix 1, Supplemental Table 1, available at www.cmajopen.ca/content/10/4/E865/suppl/DC1, for case definitions.
Patient characteristics before and after the implementation of outpatient telemedicine billing codes
Statistical analysis
We compared patient characteristics in the pretelemedicine and telemedicine periods using standardized differences. To address the possibility that the pandemic modified health-seeking behaviour and may have reduced emergency department visits for TIA, we computed the annual age–sex standardized rates of emergency department visits, discharged without admission, for TIA or ischemic stroke, standardized to the Ontario adult population of 2020. We calculated the risk difference and 95% confidence interval (CI) to compare care in the 2 periods. We used Cox proportional hazards models to estimate the adjusted hazard ratio (HR) and 95% CI for 90-day death during the telemedicine compared with the pretelemedicine period, adjusted for age (continuous), sex, neighbourhood income quintile, rurality, most responsible diagnosis (TIA v. stroke), hypertension, diabetes, atrial fibrillation, dyslipidemia, history of stroke, coronary artery disease and peripheral artery disease (Appendix 1, Supplemental Table 1). We used adjusted cause-specific hazard models to evaluate 90-day hospital admission accounting for the competing risk of death.15 All data analyses were performed using SAS Enterprise Guide version 9.4 (SAS Institute Inc.).
Ethics approval
Data sets were linked using unique encoded identifiers and analyzed at ICES. The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act without the requirement for research ethics board approval.
Results
We identified 47 601 patients discharged from an emergency department with diagnosis of TIA (n = 35 695, 75.0%) or ischemic stroke (n = 11 906, 25.0%). Median age was 73 (interquartile range 62–82) years, and 49.3% were female (n = 23 468). Patient characteristics in the pretelemedicine and telemedicine periods were balanced, except for a small reduction in the number of patients evaluated in nondesignated centres, with a corresponding increase in the number evaluated at comprehensive stroke centres (Table 1). Although the age–sex standardized rate of emergency department visits for TIA or ischemic stroke was lower in 2020 than in previous years, the decrease was consistent with the temporal trends throughout the study period (Figure 1).

Age–sex standardized rates and standard error of emergency department visits for transient ischemic attack or ischemic stroke per 100 000 discharged without admission.
Telemedicine visits increased after Apr. 1, 2020, with 83.1% (n = 6236) of patients having at least 1 telemedicine visit within 90 days of emergency department discharge, compared with 3.8% (n = 1531) at baseline (Figure 2). When all visit modalities were considered, physician visits remained unchanged between the pretelemedicine and telemedicine periods (83.2% v. 85.3% at 28 d, risk difference 2.2 [95% CI −0.1 to 4.4]; and 92.9% v. 94.0% at 90 d, risk difference 1.1 [95% CI −1.3 to 3.5]) (Figure 3; Appendix 1, Supplemental Table 2).

Pattern of clinic visits within 90 days of emergency department discharge for transient ischemic attack or minor stroke.
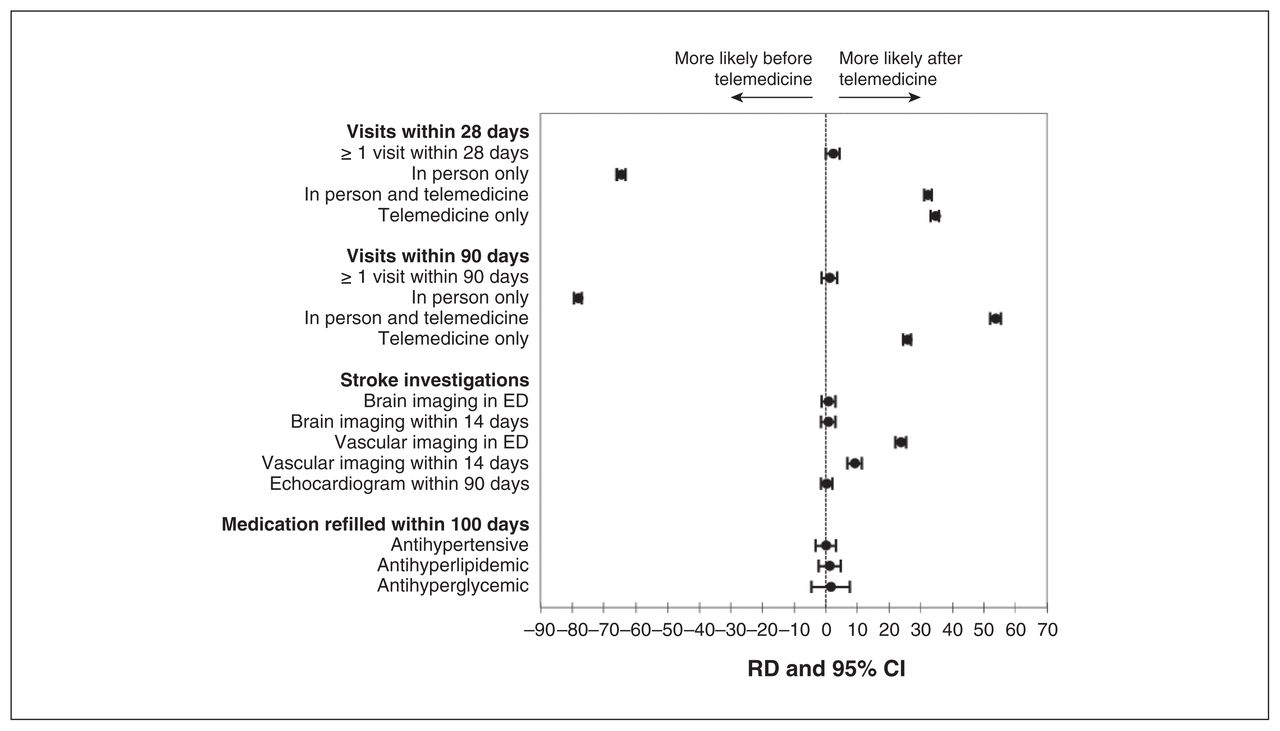
Forest plot of the risk difference (RD) and 95% confidence interval (CI) of clinic visits, stroke investigations and medication refills after the implementation of telemedicine compared with before. Note: ED = emergency department.
Admission and death within 90 days of emergency department discharge before and after the implementation of outpatient telemedicine billing codes
To explore whether certain patient groups were more vulnerable to a lack of follow-up, we compared the characteristics of the patients who had no follow-up visits within 28 days of emergency department discharge with the characteristics of patients who had at least 1 visit. Patients without any visits were more likely to live in the lowest income quintile neighbourhoods (v. other quintiles), to live in rural regions (v. urban ones) and to have a diagnosis of stroke (v. TIA). These patterns were similar before and after the implementation of telemedicine (Appendix 1, Supplemental Table 3).
We found some differences in the pattern of visits with family physicians versus stroke specialists. Compared with the pretelemedicine period, there was a greater proportion of patients without any family physician visit within 90 days of the emergency department discharge during the telemedicine period (21.8% v. 24.0%; risk difference 2.2 [95% CI 1.0 to 3.4]), but fewer patients had no specialist visit (23.0% v. 19.1%; risk difference −3.9 [95% CI −5.0 to −2.9]) (Appendix 1, Supplemental Table 2). However, among patients who were seen by a physician, a higher proportion of patients had 3 or more visits with a family physician (30.9% v. 36.8%; risk difference 5.9 [95% CI 4.4 to 7.3]) or a specialist (12.7% v. 19.6%; risk difference 6.9 [95% CI 5.9 to 8.0]) after the implementation of telemedicine compared with baseline.
Use of stroke investigations and early renewal of medications for vascular risk factors were largely similar in the 2 periods (Figure 3). There was an overall increase in use of vascular imaging and a shift from carotid Dopplers in favour of CT angiography (Appendix 1, Supplemental Figure 1). Finally, all clinical outcomes including all-cause and stroke-specific admissions and death within 90 days remained unchanged during the 2 periods (Table 2).
Interpretation
In this population-based analysis, we showed a rapid uptake in telemedicine use for the outpatient management of acute minor ischemic cerebrovascular events after Apr. 1, 2020. The number and timeliness of visits with family physicians or specialists and the use of stroke investigations and early medication renewals remained largely stable, and clinical outcomes were unchanged.
We found an increase in the use of neurovascular imaging after Apr. 1, 2020, but this was likely due to a change in clinical practice because neurovascular imaging increased throughout the study period (Appendix 1, Supplemental Figure 1). This observation, along with the shift from carotid Dopplers to CT angiography, are consistent with the Canadian Stroke Best Practice Recommendations,14 and it is reassuring that these gains appear to have been maintained despite the implementation of telemedicine during the pandemic.
Transient ischemic attack and minor stroke account for most of the burden of ischemic cerebrovascular disease and represent an important opportunity for stroke prevention.16 Our findings suggest that telemedicine is an effective complementary or alternative health care delivery method to maintain standard of care when in-person care is disrupted. Given that telemedicine has many potential benefits beyond protection against infectious disease exposure during the pandemic, including improved access to stroke experts for patients living in remote regions, reduced time and costs related to travel for the patient, and better engagement of family members and caregivers, our study supports maintaining telemedicine beyond the pandemic.6,17
The stability in hospital admissions and deaths outcomes with the widespread adoption of telemedicine was reassuring, particularly because the telemedicine cohort may be vulnerable to selection bias for patients with more severe events. Indeed, prior reports have found that patients with non-disabling strokes were less likely to present to medical attention during the pandemic.18,19 Nevertheless, about 15% of patients in our cohort did not have any physician follow-up within 28 days of an emergency department visit for TIA or ischemic stroke, suggesting that the availability of telemedicine as an alternative visit modality may be insufficient to improve access to care for those who are vulnerable to loss to follow-up, including patients who live in neighbourhoods with low income quintile and rural areas, or who are diagnosed with stroke as opposed to TIA.
In addition, we found some differences in the patterns of physician visits: a higher proportion of patients had a follow-up with a specialist, but a lower proportion had a follow-up with a family physician during the telemedicine period compared with baseline. Telemedicine fee codes were announced simultaneously for family physicians and specialists, but their uptake may have been slower among family physicians, who may be more likely to have a private practice, while specialists may be more likely part of a larger group practice or have hospital affiliations, which may have facilitated the initial transition from in-person to telemedicine care. We do not know if other factors, such as familiarity with the use of telemedicine or comfort with virtual assessments for neurologic disorders, affected uptake in different physician groups. However, we observed that once a patient had connected with a family doctor or specialist, they were more likely to have subsequent visits in the telemedicine period compared with pretelemedicine. It is not clear if the subsequent visits were driven by the need for additional clinical evaluation (e.g., a comprehensive physical examination after a telephone visit), or if they reflected care via video or telephone that was already occurring before telemedicine (e.g., a phone call to discuss a test result), but this latter type of visit was not previously remunerated and therefore not captured.
Limitations
Our study has several limitations. Residual confounding from the effects of the pandemic, stroke severity, admission thresholds, patient health-seeking behaviour or other unmeasured confounders is possible. The widespread use of telemedicine coincided with the global pandemic onset, making it impossible to distinguish the effects of one from the other on TIA and stroke care and outcomes. Nevertheless, we adjusted for major vascular comorbidities, and all patients in the cohort were discharged from the emergency department without admission, suggesting that their event was unlikely to be severely disabling. Other limitations include the inability to differentiate video from telephone encounters, a lack of information on patient satisfaction or potential barriers to telemedicine, and no pharmacy data for patients younger than 65 years, and we could not evaluate renewal of acetylsalicylic acid, as this medication is available over the counter, nor lifestyle interventions for stroke prevention (e.g., diet, exercise), as this information is not available in administrative data. Our study focused on the first 90 days after TIA because this is the highest period for stroke recurrence,3,4 and future studies on telemedicine and longer-term outcomes after TIA are needed. Administrative data codes for TIA have moderate to high specificity (> 90%) and positive predictive value (> 76%), but low sensitivity (37%),9,10 partially reflecting the inherent clinical challenges in making a diagnosis of TIA in the emergency department. The Canadian Institute for Health Information coding standards for TIA remained unchanged during the study period; thus, we do not anticipate any differences in patient selection before versus after the implementation of telemedicine. We did not evaluate the economic implications of telemedicine for either patients or the health care system, and this is a relevant area for future study. Finally, our study population all had an in-person visit with an emergency department physician and were presumably discharged without hospitalization because there were no disabling deficits identified on physical examination. Our findings may not be generalizable to other clinical scenarios where in-person assessments are required. The external generalizability of our findings to countries without publicly funded access to physician and hospital visits is also limited.
Conclusion
Understanding care and short-term outcomes after a TIA or minor ischemic stroke in the context of the pandemic and widespread telemedicine use is relevant because this patient population requires urgent outpatient follow-up and may be particularly vulnerable to delays in care. Our findings suggest that care via telemedicine can be complementary to in-person assessments without negatively affecting care and outcomes. Further work on minimizing loss to follow-up of patients with TIA or minor stroke is needed.
Acknowledgement
This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). This study also received funding from the Ontario Health Data Platform (OHDP), a Province of Ontario initiative to support Ontario’s ongoing response to COVID-19 and its related impacts. Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information (CIHI). The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. The authors thank IQVIA Solutions Canada Inc. for use of its Drug Information File.
Footnotes
Competing interests: Amy Yu reports a grant and a National New Investigator Award from the Heart and Stroke Foundation of Canada, and funding from the Ontario Health Data Platform. No other competing interests were declared.
This article has been peer reviewed.
Data sharing: The data set from this study is held securely in coded form at ICES. While data sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet criteria for confidential access following an application process.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/10/4/E865/suppl/DC1.
Contributors: Amy Yu contributed to the funding acquisition, literature search, study design, data interpretation, and manuscript drafting and editing. Jeremy Penn, Peter Austin, Douglas Lee, Joan Porter, Jiming Fang, Donald Redelmeier and Moira Kapral contributed to the study design, data interpretation, and manuscript reviewing and editing. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: Amy Yu holds a National New Investigator Award. Peter Austin and Moira Kapral hold Mid-Career Investigator Awards from the Heart and Stroke Foundation of Canada. Moira Kapral holds the Lillian Love Chair in Women’s Health at the University Health Network. Donald Redelmeier is supported by a Canada Research Chair in Medical Decision Sciences. Douglas Lee is the Ted Rogers Chair in Heart Function Outcomes, a joint chair of the University Health Network and University of Toronto. This study was supported by the Heart and Stroke Foundation of Canada (Grant-in-Aid G-19-0024262).
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2022 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools





