


Abstract
Background: Current methods used to estimate surgical wait times in Ontario may be subject to inconsistencies and inaccuracies. In this population-level study, we aimed to estimate cataract surgery wait times in Ontario using a novel, objective and data-driven method.
Methods: We identified adults who underwent cataract surgery between 2005 and 2019 in Ontario, using administrative records. Wait time 1 represented the number of days from referral to initial visit with the surgeon, and wait time 2 represented the number of days from the decision for surgery until the first eye surgery date. In the primary analysis, a ranking method prioritized referrals from optometrists, followed by ophthalmologists and family physicians.
Results: The cohort consisted of 1 138 532 people with mostly female patients (57.4%) and those aged 65 years and older (79.0%). In the primary analysis, the median was 67 days for wait time 1 (interquartile range [IQR] 29–147). There was a median of 77 days for wait time 2 (IQR 37–155). Overall, the following proportions of patients waited less than 3, 6 and 12 months: 54.1%, 78.5% and 91.7%, respectively. For wait time 2, the proportions of patients who waited less than 3, 6 and 12 months were 49.5%, 77.1% and 93.3%, respectively. In total, 19.3% of patients did not meet the provincial target for wait time 1, 20.5% did not meet the target for wait time 2 and 35.0% did not meet the target for wait times 1 or 2.
Interpretation: Administrative health services data can be used to estimate cataract surgery wait times. With this method, 35.0% of patients in 2005–2019 did not receive initial consultation or surgery within the provincial wait time target.
Cataract surgery is one of the most commonly performed surgeries in Canada and is expected to more than double in volume over the next 25 years.1,2 In Ontario, Canada, there will be a 128% necessary increase in cataract surgical volumes over 25 years to meet population demand.2 Current cataract surgery wait times are publicly available by way of the Wait Time Information System (WTIS).3 Two wait times are disclosed: the time from initial referral to the first appointment with an ophthalmologist (i.e., wait time 1), and the time from the decision to pursue cataract surgery to the date of surgery (i.e., wait time 2).3 Surgeons assign 1 of 4 priority levels that have corresponding surgical wait time targets (Appendix 1, available at www.cmajopen.ca/content/11/2/E329/suppl/DC1).3 Most patients are designated as priority 4, meaning there is minimal risk of disease progression affecting morbidity. According to the WTIS, 82% (for wait time 1) and 59% (for wait time 2) of patients receive care within the provincial benchmark of 182 days, respectively.3 Long wait times have been associated with substantial visual loss and an effect on quality of life.4 Wait times on the WTIS are self-reported by surgeons. We believe that wait times are overestimated or underestimated relative to true wait times depending on the surgeon or institution. This is because administrative policies for identifying cases on the system can differ, and it is difficult to independently verify the accuracy of this information.
An independent and data-driven process of reporting cataract surgery wait times in Ontario is needed. This may avoid potential data entry differences between surgeons and resultant inaccuracies. This approach may provide insights into the regions that have long wait times and need further allocation of public funding for cataract surgeries. The study objective was to use a repository of administrative health services records for the population eligible for universal health coverage in Ontario to estimate wait times for cataract surgery in Ontario, as well as the proportion of patients reaching provincial wait time targets.
Methods
We performed a retrospective population-based analysis of provincial health administrative data in Ontario from Jan. 1, 2005, to Dec. 31, 2019. Ontario is the largest Canadian province with a population of 14.5 million people. Publicly funded health care is offered in Ontario by way of the Ontario Health Insurance Plan (OHIP).
Data sources
As an independent, nonprofit research institute, ICES collects and analyzes health care and demographic data for health system evaluation and improvement. Baseline characteristics were collected by way of the Registered Persons Database. The OHIP data set contains claims for insured health services and was used to determine wait times (Appendix 2, available at www.cmajopen.ca/content/11/2/E329/suppl/DC1). These data sets were linked using unique encoded identifiers and analyzed at ICES. A privacy impact assessment was approved. The secure health services databases at ICES were accessed by an experienced data analyst (M.H.). No patient identifiers were collected or reported.
Cohort selection
Using the OHIP database, people who had cataract surgery between Jan. 1, 2005, and Dec. 31, 2019, aged 18 years and older were eligible for inclusion. If a person did not have a referral, or if they did not see their cataract surgeon before their surgery date, they were excluded from the study. People were excluded if they did not see their cataract surgeon within 2 years before their surgery, had more than 4 visits to their cataract surgeon within the 2 years preceding surgery or did not see their cataract surgeon within 3 years from their referral. The selection procedure can be found in Appendix 2.
Wait time definition
Estimates for wait time 2 were determined first. Records from OHIP were examined to a maximum of 2 years before surgery date, and the second last visit to the cataract surgeon was defined as the date the decision for surgery was made. The second last visit to the surgeon was chosen as the start of wait time 2, given that this is most often the date that the decision to pursue surgery is made, and when the preoperative visit (i.e., last visit before surgery) is booked where preoperative testing is performed and reviewed with the patient. If there was only 1 visit with the cataract surgeon within the 2-year lookback window, then that visit was used. The number of days from the second last visit or only visit preoperatively to the surgery date was defined as the estimate for wait time 2.
Given that most cataract surgery referrals are made by optometrists,5 a ranking method was used for the primary analysis. Rationale for this method can be found in Appendix 2. This ranking method ranked the source of referral to determine the referral date. The referral date from an optometrist was selected first. If no optometrist referral existed, then the referral from an external ophthalmologist was used. If both referrals did not exist, the referral date from the family physician was used (Appendix 2). We note that there is no provincial coverage of routine eye examinations for people aged 20–64 years.
Two sensitivity analyses were conducted to evaluate wait times: choosing the earliest (i.e., furthest from surgery date) and the latest (i.e., closest to surgery date) potential referral from any source. The number of days from referral to the first visit to the cataract surgeon after their referral, to a maximum of 3 years, was defined as the estimate for wait time 1.
Statistical analysis
The primary objective was to estimate wait times 1 and 2 for cataract surgery with this method. Wait times 1 and 2 represented the categorical and continuous outcomes. We investigated the proportion of patients who had a wait time 1 or 2 of less than 3, 6 and 12 months, and the proportion that did not meet the target time of 182 days for wait times 1 and 2. The primary analysis used the ranking method. All patients were compared with the wait time targets for priority 4 cases as no information on surgical priority groups were available. To evaluate a differing set of assumptions, secondary analyses computed wait times stratified by referral source and a subgroup analysis evaluated wait times in patients with a single referral and patients with multiple eligible referrals separately. A second subgroup analysis evaluated wait times based on the age of the patient. Temporal patterns in the percentage of patients not meeting provincial wait time thresholds were descriptively recorded. All analyses were conducted at ICES using SAS statistical software (version 9.4).
Ethics approval
Ethics approval was granted by the Trillium Health Partners Research Ethics Board (ID No. 1057). The Reporting of Studies Conducted using Observational Routinely-collected Data (RECORD) reporting guidelines were followed.6
Results
Overall, we identified 20 795 884 people with a valid sex, age and OHIP identification number. After exclusions, the study cohort consisted of 1 138 532 people (Figure 1). Table 1 and Appendix 3, available at www.cmajopen.ca/content/11/2/E329/suppl/DC1, detail the baseline demographic information for the cohort. In general, more females (n = 651 890, 57.3%) and people aged 65 years and older (n = 898 926, 79.0%) underwent cataract surgery. Most patients (n = 869 724, 76.4%) had 2 or 3 potential referrals before surgery within the prespecified lookback window. Cataract surgeries occurred at a similar volume throughout the study period (Appendix 3).

Consolidated Standards of Reporting Trials (CONSORT) flowchart for study selection. Note: IKN = ICES key number.
Summary of baseline demographic characteristics and their distribution in the study cohort
The practitioner type for initial referral is provided in Table 2. In the primary analysis, optometrists saw patients preoperatively as the potential referral source in 78.8% of cases (n = 897 524). In the sensitivity analysis of the earliest potential referral, about one-third of patients saw an optometrist, and more than one-half saw a family physician. In the sensitivity analysis of the latest potential referral, more than one-half of patients saw an optometrist and more than one-third saw a family physician.
Source of initial referral stratified by analysis type
Primary analysis
In the primary analysis, the median wait time 1 using the referral source ranking method was 67 days (interquartile range [IQR] 29–147) (Figure 2). Overall, the following proportion of patients waited less than 3, 6 and 12 months: 54.1%, 78.5% and 91.7%, respectively. A total of 19.3% of patients did not meet the provincial target time of 182 days for wait time 1 using the same method. In the sensitivity analysis, there was a median of 173 days for wait time 1 (IQR 67–397) when using the earliest possible referral method to the maximum of 3 years between referral and initial consultation with the cataract surgeon. This was in contrast to a wait time 1 of 49 days (IQR 21–104) when using the latest possible referral within the same lookback window.

Distribution of time from initial referral to initial consultation with a cataract surgeon (wait time 1) in the primary analysis.
There was a median of 77 days for wait time 2 (IQR 37–155) with the referral source ranking method in the primary analysis. For wait time 2, the proportion of patients who waited less than 3, 6 and 12 months were 49.5%, 77.1% and 93.3%, respectively. With this method, 20.5% of surgeries did not meet the provincial wait time target.
Secondary analysis: referral source
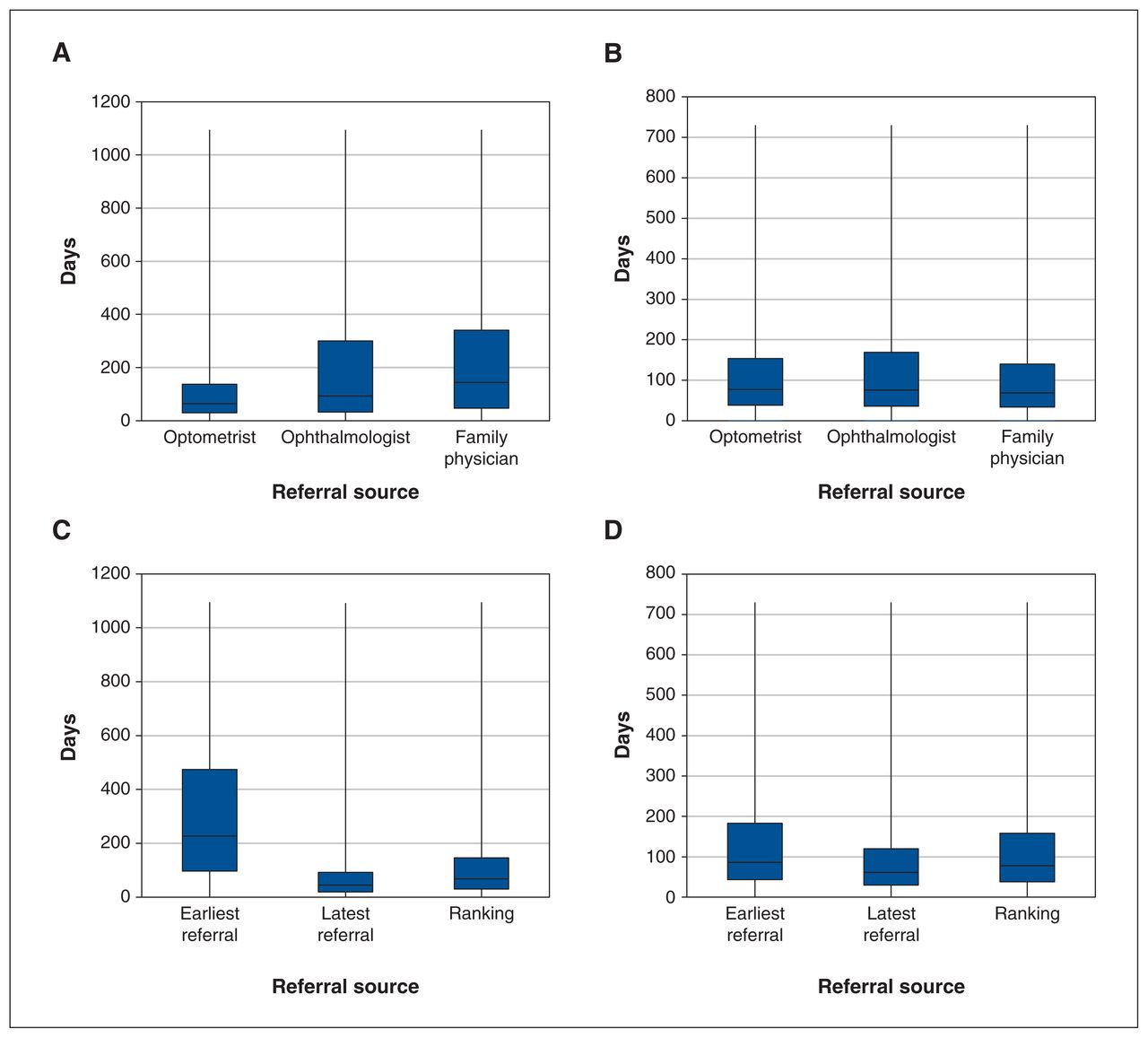
When the analysis was stratified by referral source, there was a median of 65 days for wait time 1 (IQR 30–138) for patients seen by an optometrist, 93 days (IQR 33–300) for patients seen by an ophthalmologist and 144 days (IQR 47–341) for patients seen by a family physician (Figure 3A). The median was 77 days for wait time 2 (IQR 38–154) for patients seen by an optometrist, 76 days (IQR 36–169) for patients seen by an ophthalmologist and 69 days (IQR 34–140) for patients seen by a family physician (Figure 3B).

(A) Distribution of time from initial referral to initial consultation with cataract surgeon (wait time 1) stratified by referral source. (B) Distribution of time from initial consultation with cataract surgeon to cataract surgery (wait time 2) stratified by referral source. (C) Distribution of time from initial referral to initial consultation with cataract surgeon (wait time 1) restricted to patients with multiple referral sources. (D) Distribution of time from initial consultation with cataract surgeon to cataract surgery (wait time 2) restricted to patients with multiple referral sources. Note: The box represents the interquartile range and the whisker plot shows whiskers extending to the minimum and maximum wait times.
Subgroup analysis: single eligible referral
After restricting the analysis to patients with a single eligible referral, the median was 68 days for wait time 1 (IQR 28–152). The median was 74 days for wait time 2 (IQR 36–149).
Subgroup analysis: multiple eligible referrals
When restricting the analysis to consider only patients with multiple eligible referrals, the median was 67 days for wait time 1 (IQR 30–146) for the ranking method, which contrasted with 227 days (IQR 97–474) when the earliest potential referral was considered, and 45 days (IQR 20–92) when considering the latest potential referral (Figure 3C). The median was 78 days for wait time 2 (IQR 38–158) using the ranking method, which was in line with the results when the earliest potential referral (median 86 d, IQR 43–183) or latest potential referral (median 61 d, IQR 30–120) were considered (Figure 3D).
Subgroup analysis: age
Using the ranking method, the median for patients aged 20–64 years was slightly shorter relative to those aged 65 years and older (wait time 1: 65 d v. 68 d; wait time 2: 68 d v. 79 d).
Time trend analysis
The highest proportion of patients not meeting provincial wait time targets for wait times 1 and 2 were seen in 2005 and 2017–2019, based on the date of surgery (Figure 4). The lowest proportion was observed from 2008 to 2013.

Time trend analysis of the proportion of patients not meeting provincial wait time targets from 2005 to 2019. Note: WT1 = wait time 1; WT2 = wait time 2. Error bars represent 95% confidence intervals.
Interpretation
In this analysis, the wait times from initial referral to first consultation (wait time 1) and from first consultation to cataract surgery (wait time 2) were investigated for more than 1 million patients in Ontario, Canada. In the primary analysis, there was significant variability in wait time 1 (median 67 d), depending on what method was used to identify the initial referral date. For wait time 2, the medians were similar across the methods used, and the results showed a median of 2 to 3 months. A high proportion (35.0%) of cataract patients receiving surgery between 2005 and 2019 did not meet the priority 4 provincial wait time target for either wait times 1 or 2.
When compared with data from the Canadian Institute for Health Information (CIHI), our median of 92 days (wait time 2) was longer than the reported CIHI data (63 d) from April to September 2019.5 Canadian Institute for Health Information wait times are derived from WTIS data of only 94 Ontario hospitals that perform adult surgery, effectively representing a subset of Ontario cataract surgeries.7 We also believe that current self-reported wait time data submitted to CIHI may not be accurate, and may be underestimating the actual wait times for cataract surgery.
The use of a large health administrative database for documentation of cataract surgical wait times has multiple advantages. By using an objective, data-driven, standardized methodology, policy-makers can appreciate regional differences in cataract surgical wait times, which would allow for further allocation of surgical cases to centres most in need. In addition, wait times from the administrative database can be scrutinized over time. Important uncertainty estimations can be provided in the analysis of administrative data, such as a sensitivity analysis using the latest and earliest referral date. A major conclusion of this analysis is that when using administrative data for tabulation of wait times, there is likely to be a higher degree of confidence with wait time 2 results observed relative to wait time 1.
Limitations
With the administrative databases used, there is no identifier for the date of referral, with sensitivity analyses based on differing assumptions about the referring provider used to recognize the uncertainty in these estimates. We acknowledge the possibility of misclassification of the referring physician, especially for people aged younger than 65 years who paid out of pocket for an optometrist evaluation and referral for cataract surgery. We did not consider referrals for cataract surgery that did not involve an optometrist, ophthalmologist or family physician, as well as patient referrals that were requested outside of a billable appointment by a referring provider. These other referrals likely represent a minority of cases, and only 1.8% of patients were excluded owing to not having an initial visit by at least 1 of these health care professionals or for not having a visit to the cataract surgeon before surgery (Figure 1). For this reason, we acknowledge that a potential advantage of self-reporting of wait times, as is currently done, is that a greater proportion of referrals are captured. For wait time 1, optometrists do not always report a billing code with a cataract diagnosis, and therefore other diagnostic optometrist codes were considered. Based on clinical experience, unique cases in which wait time 1 exceeded 3 years or wait time 2 exceeded 2 years were excluded in the analysis, though these were a minority of cases (0.9%, Figure 1). This method of data reporting would not be able to account for changes to surgeon behaviour in referral management in the setting of an incentivized system. For wait time 2, patients followed at baseline by a cataract surgeon had an unclear date of visually significant cataract diagnosis, thus affecting the accuracy of the observed wait time 2. Similarly, factors that may influence wait time 2, such as preoperative anesthesia or subspecialist consultation, preoperative management of ocular comorbidities or patient hesitancy, could not be captured in the databases analyzed. These factors may lead to an overestimation of wait time 2. It is also important to mention that our study does not comment on the appropriateness of cataract surgery for included patients, and excludes patients with cataracts who did not receive surgery.
Conclusion
The use of administrative health data to systematically calculate cataract surgery wait times represents a promising modality. In our analysis, 35.0% of cataract surgery patients in 2005–2019 did not receive initial ophthalmic consultation or surgery within the wait time target of 182 days when considering the ranking method. The method provided allows for regions to be identified and prioritized for further government funding based on long wait times, as well as an evaluation of predictors of wait times. These methods can be easily incorporated in the evaluation of wait times of other ambulatory surgeries. We believe that the reporting of wait time 2 is reproducible and accurate; however, there is an inherent uncertainty regarding wait time 1 owing to the inability to identify the date of referral. The creation of new billing codes made at the time of referral should be explored as this would improve the accuracy of wait time 1 estimates. In our efforts to characterize wait times, we hope to aid researchers and policymakers in highlighting the access and disparities to cataract surgery care in Ontario.
Footnotes
Competing interests: Marko Popovic has received research grant support from PSI Foundation and Fighting Blindness Canada. Matthew Schlenker has received consulting fees and speaker honoraria from Alcon and Allergan. He has also received speaker honoraria from Bausch Health, Johnson & Johnson Vision and Théa-Labtician. He has received consulting fees from Light Matter Interaction and Santen. Iqbal Ahmed has received consulting fees from Aequus, Aerie Pharmaceuticals, Akorn, Alcon, Allergan, Aquea Health, Inc, ArcScan, Bausch Health, Beaver Visitec, Beyeonics, Carl Zeiss Meditec, Centricity Vision, Inc., CorNeat Vision, Costum Surgical, ELT Sight, ElutiMed, Equinox, Genentech, Glaukos, Gore, Iantrek, InjectSense, Iridex, iStar, Ivantis, Johnson & Johnson Vision, LayerBio, Leica Microsystems, Long Bridge Medical, Inc., MicroOptx, MST Surgical, New World Medical, Ocular Instruments, Ocular Therapeutix, Oculo, Omega Ophthalmics, PolyActiva, Radiance Therapeutics, Inc., Ripple Therapeutics, Sanoculis, Santen, Shifamed, LLC, Sight Sciences, Smartlens, Inc., Stroma, Thea Pharma, ViaLase and Vizzario. He has also received speaker honoraria from Alcon, Allergan, Carl Zeiss Meditec, Johnson & Johnson Vision and MST Surgical. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Marko Popovic, Iqbal Ahmed, Laura Rosella and Matthew Schlenker contributed to the conception of the study and all authors contributed to the design of the work. Marko Popovic and Mack Hurst drafted the study protocol. All authors contributed to data analysis and interpretation. Marko Popovic drafted the manuscript and all authors revised the manuscript for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). This study also received funding from a Canada Research Chair in Population Health Analytics. Parts of this material are based on data and information compiled and provided by the MOH and CIHI. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Data sharing: Data used in this analysis are not publicly available and were accessed by way of the ICES databases.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/2/E329/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.