


Abstract
Background: To date, there has been little research on the effect of safe consumption site and community-based naloxone programs on regional opioid-related emergency department visits and deaths. We sought to determine the impact of these interventions on regional opioid-related emergency department visit and death rates in the province of Alberta.
Methods: We used a retrospective observational design, via interrupted time series analysis, to assess municipal opioid-related emergency department visit volume and opioid-related deaths (defined by poisoning and opioid use disorder). We compared rates before and after program implementation in individual Alberta municipalities and province-wide after safe consumption site (March 2018 to October 2018) and community-based naloxone (January 2016) program implementation.
Results: A total of 24 107 emergency department visits and 2413 deaths were included in the study. After safe consumption site opening, we saw decreased opioid-related emergency department visits in Calgary (level change −22.7 [−20%] visits per month, 95% confidence interval [CI] −29.7 to −15.8) and Lethbridge (level change −8.8 [−50%] visits per month, 95% CI −11.7 to −5.9), and decreased deaths in Edmonton (level change −5.9 [−55%] deaths per month, 95% CI −8.9 to −2.9). We observed increased emergency department visits after community-based naloxone program implementation in urban Alberta (level change 38.9 [46%] visits, 95% CI 33.3 to 44.4). We also observed an increase in urban opioid-related deaths (level change 9.1 [40%] deaths, 95% CI 6.7 to 11.5).
Interpretation: The results of this study suggest differences exist between municipalities employing similar interventions. Our results also suggest contextual variation; for example, illicit drug supply toxicity may modify the ability of a community-based naloxone program to prevent opioid overdose without a thorough public health response.
In 2020, 1144 opioid overdose deaths occurred in Alberta, highlighting the lethal and complex nature of the opioid crisis.1 The pathway to opioid use and misuse is complex, as described by Jalali and colleagues in their complex framework identifying factors ranging from individual to societal.2 Interventions introduced to reduce opioid overdose in Alberta are described in a program theory (Appendix 1, available at www.cmajopen.ca/content/11/3/E537/suppl/DC1). Although these interventions may reduce deaths, they do not address all factors that contribute to opioid addiction and death.
The current study focuses on supervised consumption sites, overdose prevention sites and the widespread distribution of naloxone kits, through the community-based naloxone program. Research on supervised consumption and overdose prevention sites elsewhere has identified benefits, including a decrease in overdose fatalities and an increase in access to addiction services in Vancouver, Canada, and a reduction in ambulance visits in Sydney, Australia.3–5 Community-based naloxone programs have found success in the United States, with a region in Massachusetts identifying a decrease in fatalities and a region of North Carolina reporting reduced health care costs.6,7 However, since 2019, 3 out of 7 supervised consumption sites in the province of Alberta have been closed, and implementation of 2 additional sites has been halted by provincial authorities.8–10 These changes come on the heels of a controversial and widely critiqued review.11,12 Given the current political climate surrounding supervised consumption sites and the continuing opioid crisis, we sought to explore the evidence on the impact of the aforementioned interventions on opioid-related deaths and opioid-related emergency department visits within Alberta.13,14 Our study aims to build on previous research on neighbourhoods immediately adjacent to supervised consumption sites by studying the effect of supervised consumption sites at a municipal (defined as within city boundaries, rather than adjacent neighbourhoods) level.15
As part of a public health response to overdose deaths, Alberta scaled up and implemented both supervised consumption and overdose prevention sites beginning in 2017.16 Supervised consumption sites are locations where users can be monitored while using previously obtained drugs and may access other services such as counselling, social work and opioid agonist treatment. They are exempted from the application of federal drug laws by Health Canada and are designed for long-term operation. Overdose prevention sites are temporary supervised consumption sites where individuals may be observed while using previously obtained substances, with intervention for adverse events, such as overdose. In Alberta, supervised consumption sites currently operate in Calgary and Edmonton, and a former supervised consumption site in Lethbridge was closed in August 2020. An overdose prevention site operates in Red Deer.17 The aforementioned government report suggests that sites have seen approximately 5878 visits per month, with 5301 in Edmonton and 5683 in Calgary.11,12
Alberta is also home to a community-based naloxone program, which began in January 2016.17 With more than 1000 pharmacies, emergency departments, postsecondary institutions, physician offices, community services and correctional facilities participating in the program, Alberta has the largest community-based naloxone program in Canada.18 From the start of the program to December 2019, more than 78 000 kits have been distributed — an estimated 513 per month in urban areas and 889 in rural areas.19 Through the community-based naloxone program, Alberta pharmacies are permitted to distribute free naloxone to the public without collection of personal identifying information. Naloxone kits have been distributed by Safeworks in Edmonton since 2005.20 Pilot projects in other regions culminated in eventual province-wide rollout in January 2016.21,22
Although ample research exists showing strong uptake of community-based naloxone programs and municipal overdose prevention via supervised consumption sites, relatively little literature exists at the regional level comparing trends and volumes in opioid-related emergency department visits and deaths after intervention implementation.7–9 Further, though previous research has studied supervised consumption site visitation and fentanyl-related deaths, data focusing on all-opioid-related deaths and emergency department visits are lacking.23
Our study thus aimed to address the overarching question of “What is the impact of opioid-intervention strategies on municipal emergency department visits and deaths?”. To answer our overarching research question, we established 4 objectives, which included identifying changes in volume of municipal opioid-related emergency department visits after supervised consumption site openings, identifying changes in municipal opioid-related deaths after supervised consumption site openings, identifying changes in regional opioid-related emergency department visits after implementation of the community-based naloxone program, and identifying changes in regional opioid-related deaths after implementation of the community-based naloxone program.
Methods
We used a retrospective observational design, via interrupted time series analysis and autoregressive integrated moving average with explanatory variable (ARIMAX) modelling, to compare municipal opioid-related emergency department visit volume and opioid-related deaths before and after implementation of safe consumption sites (March 2018 to October 2018) and a community-based naloxone program (January 2016).
Population and data source
Data on emergency department visits were collected from the National Ambulatory Care Reporting System, and data on opioid-related fatalities were collected from the Government of Alberta Vital Statistics Office. Data are extractable from both on request, and the data were cleaned by repository owners. Data were collected from Oct. 1, 2013, to Feb. 29, 2020, for emergency department visits, and from Oct. 1, 2013, to Mar. 31, 2019, for deaths. Data from beyond 2020 were not included owing to the potential impact of the COVID-19 pandemic and related public health measures on opioid-related emergency department visits and fatalities. Data were selected based on the Canadian version of the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10-CA). Emergency department visits included any patient with a diagnosis of F12 (opioid use disorder) or T40.2 (accidental opioid poisoning). Opioid deaths were identified based on medical examiner data obtained via the Vital Statistics Office, with ICD codes selected based on the Centers for Disease Control and Prevention’s Prescription and Drug Overdose Data and Statistics Guide.24 These codes included underlying cause of death codes X40–44, 60–64, 85 and Y10–14. Where available, we also screened for contributing causes of death, which included ICD codes T40.0–40.4 and T40.6 (contributing causes of death were not available after 2017).
Setting
Urban areas were defined as Calgary, Edmonton, Sherwood Park and St. Albert hospitals (with Sherwood Park and St. Albert included owing to proximity to Edmonton). The urban areas include 16 emergency departments, 4 of which were located in urgent care centres offering limited service hours, but still providing emergency services to those with acute opioid intoxication. All other areas were considered rural. Patients were geographically categorized based on the forward sortation area (first 3 postal code digits) of the patient’s residence. Geography was defined on a local level for supervised consumption sites as site operations are city specific. Community-based naloxone program geography was defined broadly as distribution was not affected by local governance.
Statistical analysis
We conducted interrupted time series via piecewise linear regression to assess slope change. Interrupted time series analyses allow for pre–post comparison of average patient volume trends across the preintervention and postintervention periods. A one-sample test was used to compare means between the preintervention and postintervention periods, and a t test was used to compare changes in slope between the preintervention and postintervention periods. We used Wald tests to calculate confidence intervals (CIs). An ARIMAX model was used to determine expected volume postintervention based on the preintervention volume and trend. Postintervention means for true values and ARIMAX values based on preintervention trend were compared to assess differences in level. We determined significance by CIs of the mean level change in the preintervention and postintervention periods. A Ljung Box test was used to test for seasonality or autocorrelation. We used the ARIMAX model to adjust for any detected autocorrelation. Opening dates for supervised consumption sites and the province-wide community-based naloxone program were defined as the month in which the programs began. All data were adjusted to the most recent population estimates available for each municipality. This was achieved by multiplying the population for each quarter by the ratio of the previous population to the most recent population. All data analysis was completed in R (version 3.6.1), with Wald CIs calculated through the epiR package.
Ethics approval
This study was approved by the University of Calgary (REB19-0238).
Results
A total of 24 107 emergency department visits and 2413 deaths were included in the study. Population data are available in Table 1. We identified trends of increasing opioid-related emergency department visits and deaths over time. Most visits and deaths occurred in urban areas. Although more regional deaths and emergency department visits were observed after the start of the community-based naloxone program compared with municipal deaths and emergency department visits after opening of the supervised consumption sites, we note less time was available in the preintervention period for community-based naloxone program analysis. With the exception of rural opioid-related emergency department visits, we observed an increasing trend in opioid-related emergency department visits and deaths over time in all areas. Seasonality was identified in some ARIMAX models, and is identified by CIs exhibiting time-series features in the figures. In areas where no seasonality was observed, a linear CI is observed.
Population data
Supervised consumption sites
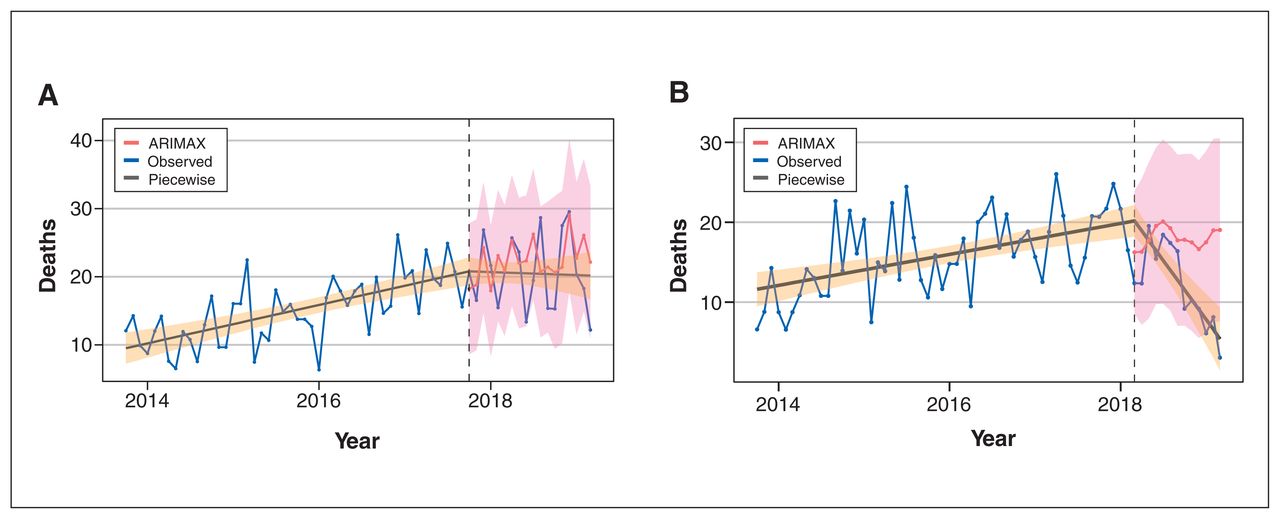
Changes in opioid-related emergency department visits and deaths after opening of supervised consumption sites can be seen in Table 2, Figure 1 and Figure 2. Changes in deaths and emergency department visits varied depending on municipality. Significant decreases in emergency department visits were observed in Calgary (absolute monthly change −22.7 [−20%], 95% CI −29.7 to −15.8) and Lethbridge (absolute monthly change −8.8 [−50%], 95% CI −11.7 to −5.9), and a significant decrease in deaths was observed in Edmonton (absolute monthly change −5.9 [−55%], 95% CI −8.9 to −2.9). We observed no significant changes in emergency department visits in Edmonton or Red Deer, and we observed no significant changes in deaths in Calgary, Red Deer or Lethbridge. Results for Lethbridge and Red Deer sites were limited by a relatively small number of deaths (n = 46) across the 2 sites over the entire study period (Appendix 2 and Appendix 3, available at www.cmajopen.ca/content/11/3/E537/suppl/DC1). There were significant negative changes in slope in Lethbridge emergency department visits and Edmonton deaths.
Interrupted time series analyses
Opioid-related emergency department visits after opening of supervised consumption sites. Piecewise 95% confidence interval (CI) in orange, ARIMAX 95% CI in pink. (A) Calgary: intervention on Oct. 1, 2017. (B) Edmonton: intervention on Mar. 1, 2018. (C) Red Deer: intervention on Oct. 1, 2018. (D) Lethbridge: intervention on Mar. 1, 2018. Note: ARIMAX = autoregressive integrated moving average with explanatory variable.
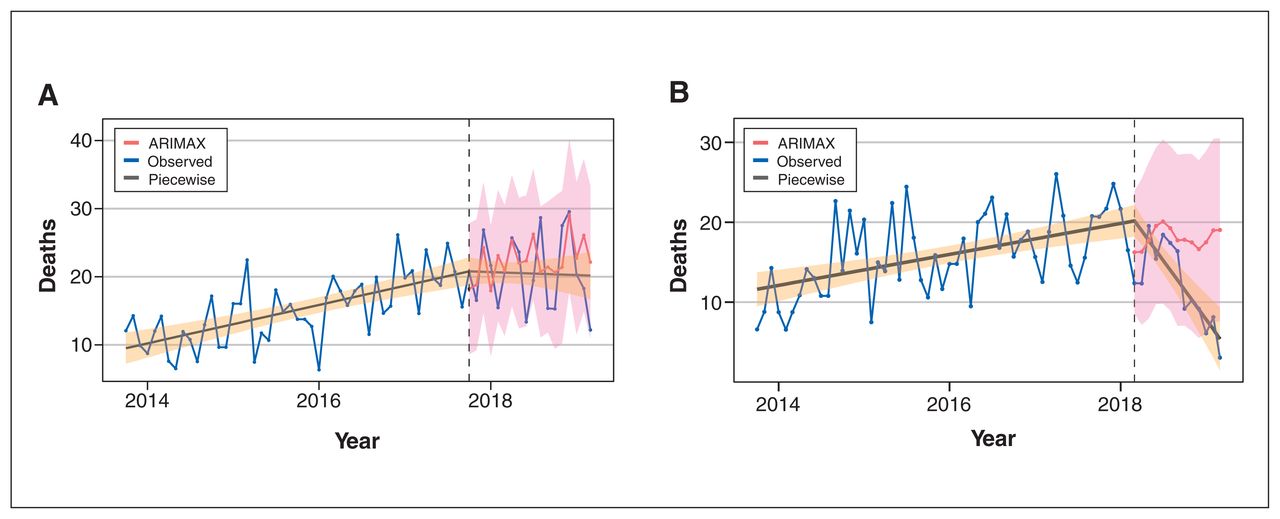
Opioid-related deaths after opening of supervised consumption sites. Piecewise 95% confidence interval (CI) in orange, ARIMAX 95% CI in pink. (A) Calgary: intervention on Oct. 1, 2017. (B) Edmonton: intervention on Mar. 1, 2018. Note: ARIMAX = autoregressive integrated moving average with explanatory variable.
Community-based naloxone program
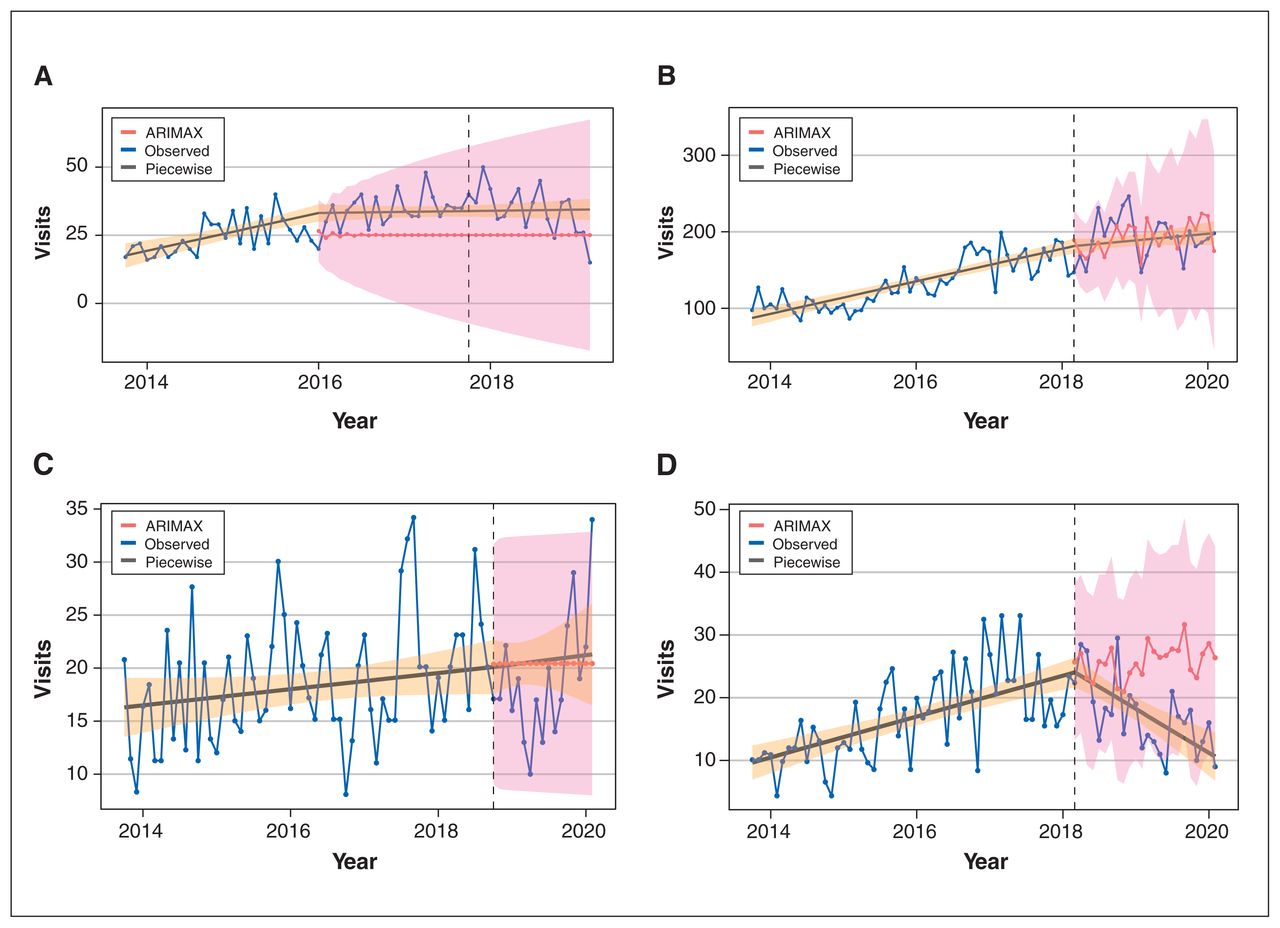
Changes in opioid-related emergency department visits and deaths can be seen in Table 2 and Figure 3. Increases were observed in opioid-related emergency department visits after community-based naloxone program initiation in urban and rural areas. This included an increase by 38.9 (46%) visits per month in urban areas (95% CI 33.3 to 44.4). An increase in deaths was also observed in urban areas, with an additional 9.1 (40%) deaths per month (95% CI 6.7 to 11.5) after the start of the community-based naloxone program. We observed no differences in deaths within rural areas after the start of the program. There were significant negative slope changes in rural emergency department visits, and in urban emergency department visits and deaths.

Opioid-related emergency department (ED) visits and deaths after community-based naloxone program initiation. Piecewise 95% confidence interval (CI) in orange. ARIMAX 95% CI in pink. (A) Urban opioid-related ED visits: intervention on Jan. 1, 2016. (B) Rural opioid-related deaths: intervention on Jan. 1, 2016. (C) Urban opioid-related deaths: intervention on Jan. 1, 2016. (D) Rural opioid-related ED visits: intervention on Jan. 1, 2016. Note: ARIMAX = autoregressive integrated moving average with explanatory variable.
Interpretation
In this study, we report on the regional effects of community-based naloxone programs and municipal-level effects of supervised consumption sites in Alberta using interrupted time series analysis. Despite potentially far-reaching implications of supervised consumption sites on the broader health system, including minimizing blood-borne infection and complication-related costs, the literature typically focuses on outcomes proximal to the supervised consumption site (i.e., overdoses reversed).25,26 Further, our analysis allowed us to account for existing trends in opioid-related emergency department visits and deaths at the municipal and provincial levels. To our knowledge, the use of ARIMAX modelling is previously unreported in the literature with respect to emergency department visits. In evaluation of all results for both supervised consumption site and community-based naloxone programs, such proximal harm-reduction interventions are not the only methods of reducing deaths from opioid overdose, and many complex societal factors, as described in previous research, are at play.2 Although contextual factors may mask the effectiveness of harm-reduction interventions, these interventions still demonstrate life-saving capability and reduce the burden of the opioid crisis.
Supervised consumption site analysis
Municipality-dependent variation in emergency department visit and usage trends after supervised consumption site implementation suggests that differences between programs may influence usage of supervised consumption sites among vulnerable populations. For example, the Calgary site is operated by the provincial health authority and is located within an existing health care facility. The Edmonton site is operated by an independent not-for-profit organization. The decrease in Edmonton deaths may be due to individuals trusting and developing a stronger relationship with facility operators, rather than a government body, leading to better use and reduced deaths. Similarly, the Edmonton site is downtown and 200 m away from a transit station. It may be more accessible for individuals outside the immediate area of the site. The Calgary site is further from transit, and from downtown, making it less accessible. Similarly, in Edmonton, the most recent provincial report on opioid deaths suggests they are concentrated primarily in the city centre, whereas they are concentrated in multiple areas in the Calgary area, sometimes far from the supervised consumption site.13 This may have contributed to the decrease in deaths in Edmonton, as more Edmonton opioid users could access the supervised consumption site, whereas fewer in Calgary could do the same, leading them to use substances at closer, possibly private, locations, far from the downtown site.
Provincial data suggest that at sites in Calgary and Edmonton, most (89% and 66% respectively) visits are by unique individuals, whereas in Lethbridge, the opposite is true (25%) (Red Deer data were unavailable). There are poor data on individual-specific visits and access patterns to supervised consumption sites owing to confidentiality, limiting capacity for confirmatory research of these hypotheses. Consequently, it was difficult to determine for all regions whether there were changes in usage patterns over time. Further, supervised consumption sites may also test substance toxicity, reducing the risk of individuals consuming substances laced with unexpected opioids. We note supervised consumption site services did not appear to be correlated with any increase in deaths or opioid-related emergency department visits.
Our study compares favourably with other studies, which have identified a decline or projected decline in emergency department visits and deaths after supervised consumption site openings in North American cities.27–29 Although not every municipality studied saw significant changes in opioid-related emergency department visits and deaths, previous research has found that supervised consumption sites may help reduce use of emergency medical services (EMS) and spread of blood-borne illnesses, contributing to a reduction in costs to the health care system.25–28 Research from Vancouver has also highlighted a reduction in all-cause deaths among substance users after opening of a supervised consumption site.30 Because most opioid-related deaths occur when an individual is alone while using substances, supervised consumption sites allow for individuals to have drugs tested and use substances under supervision to prevent deaths.31 Local research focusing on the Calgary supervised consumption site has identified a savings of $2.3 million over a period of 2 years and 3 months.32 These benefits, even if small, should not be underestimated in evaluating the efficacy of supervised consumption sites.
Concurrent programs may have contributed to observed reductions in the Edmonton and Calgary municipalities. In April of 2017, a virtual opioid dependency program was launched to help individuals access opioid agonist therapy. This program involved thousands of unique client visits, potentially contributing to reductions in deaths and emergency department visits. Similarly, Alberta launched an opioid agonist therapy program starting in May 2018, which distributed buprenorphine and naltrexone or methadone to individuals struggling with opioid addiction.33
Community-based naloxone analysis
With regard to the community-based naloxone program, our findings of increasing opioid-related emergency department visits and deaths contrasted with results from the existing literature focusing on initiation of community-based naloxone programs. The existing literature has generally identified decreased opioid-related deaths.6,34–36 We suspect this difference stems from several factors, including a lack of data granularity, unique scope, our focus on the regional effect of the community-based naloxone program (rather than local or population-specific impact), the recommendation of Alberta’s community-based naloxone program that EMS be used any time naloxone is used, and the time required to mature the community-based naloxone program.17,18,34 Spackman and colleagues have conducted a highly detailed analysis of the community-based naloxone program at the health zone level and identified an inverse relation between deaths and available naloxone kits (Dr. Eldon Spackman, University of Calgary: unpublished data, 2021). Their results combined with results of the current study suggest that over time, as more kits are distributed, deaths prevented by community-based naloxone will exceed deaths caused by opioids as more kits per capita are available. Our results support this hypothesis, as more kits were distributed in rural areas, where deaths remained stable, whereas urban areas with fewer kits per capita saw an increase in deaths. The contrast between the analysis by Spackman and colleagues and the current study suggests that environmental variation, such as uptake frequency, should be included to have a full picture of the relation between community-based naloxone programs, emergency department visits and deaths. Further, the community-based naloxone program recommendation of EMS attendance after kit use may cause emergency department visits to increase in a dose-dependent manner, because of overdoses being reversed. This hypothesis is congruent with Spackman and colleagues’ findings of an inverse, dose-dependent relation between deaths and kit distribution. Our observed short-term increase in deaths may be influenced by difficult-to-measure ecological variables, including increasing opioid use in the context of a province-wide recession that took place in 2015–2016, and an increasingly toxic drug supply discussed later.37,38 We hypothesize the increase in opioid toxicity and opioid use outpaced the short-term capacity of the community-based naloxone program to prevent deaths and emergency department visits at the regional level.
Lack of granular data on the community-based naloxone program limited our capacity to draw concrete conclusions. In particular, we lacked data on frequency of naloxone kit use, or when naloxone kit distribution began to scale up in urban and rural regions. Thus, we caution against using our findings to inform future policy; rather, our findings highlight the importance of capturing more detailed data surrounding naloxone use.
Opioid toxicity
Observed trends in opioid-related deaths and visits, municipally and provincially, are influenced by opioid supply toxicity, particularly after 2016. National toxicity tracking has identified increasing frequency of fentanyl and fentanyl analogues (particularly carfentanil) in tested Alberta opioids.38,39 They now account for most opioid-associated deaths in Alberta. Between 2016 and 2017, carfentanil saw a dramatic increase in commonality, going from a near-unidentified fentanyl analogue in 2016, to the most common (at 1/100 samples) by 2017. Fentanyl has also seen increasing commonality, overtaking heroin among tested samples in 2015 (at 4 and 2/100 samples, respectively). 38 Supervised consumption sites are critical resources in preventing overdose fatalities through onsite overdose prevention, intervention, drug testing (in some cases) and referral to services, breaking the cycle of addiction.
Future directions
We hope future multivariable analyses can account for environmental variations affecting opioid-related emergency department visits and deaths, and that additional data can be gleaned on other effects of supervised consumption sites and community-based naloxone programs on health services, such as callouts to emergency services. Researchers conducting future studies may wish to employ prospective analysis to collect outcome-specific data. Policy-makers should make publicly available up-to-date information on all opioid-related interventions, such as total and unique patient contacts; operation length; basic demographic data, such as age and gender; accurate, location-based volume data; patient outcomes; and intervention frequency (i.e., number of community-based naloxone kits distributed). This would help identify the most cost-effective interventions and allow for better confounder control. Lastly, up-to-date death counts are important to assess the immediate effect of opioid interventions.
Limitations
Our study had several methodological limitations, including death data available only up to March 2019, despite a late 2020 request, owing to longer provincial data processing times when compared with emergency department data. This, combined with few total deaths in Lethbridge and Red Deer, contributed to low power in analysis and reduced ability to identify significant differences. Our study relies on reported home residence for fatalities. We acknowledge that individuals may have travelled from their home residence to the studied municipalities and died within the municipality following opioid overdose. This may have led to overreporting of opioid deaths in certain municipalities and underreporting of deaths in others. Similarly, emergency department visits may be overestimated, as users may have travelled from one location to another to access opioid-related care. Some rural sites have grown over time, potentially contributing to increased opioid-related visits as part of an increase in all-cause visits. As our study compared only individual interventions, it is highly likely other environmental factors included in Appendix 1 influenced opioid-related deaths and emergency department visits in the period surrounding the opening of supervised consumption sites and surrounding the start of the community-based naloxone program.
Publicly available data on the community-based naloxone program lacked granularity, as discussed previously. It was difficult to find data for both interventions to assess changes in program scale as time progressed, and this was not included in our analysis. It is possible changes in scale may have contributed to greater program use later. It is unlikely the interventions examined were delivered in the same way on their opening date as with the most recent date of available data. This may have contributed to altered usage patterns. We find strength in the length of data available and the quality of data, with Alberta 1 of 4 provinces where emergency departments are mandated to submit data with all codiagnoses made in the emergency department to the National Ambulatory Care Reporting System. Similarly, the Vital Statistics Office collects data on all deaths in Alberta.
Conclusion
The relation between supervised consumption site introduction, deaths and emergency department visitation varies depending on municipality, but the sites appear beneficial, with decreases in deaths and emergency department visits observed in several municipalities. Further research is necessary to determine why differences exist, and more detailed analysis and data are necessary to determine the effectiveness of supervised consumption sites. Our findings should be approached with caution owing to insufficient data and inability to account for important contextual factors driving opioid use since 2016. However, our findings suggest that supervised consumption sites and community-based naloxone programs do save lives and should be expanded in practice to reduce deaths and emergency department visits. The effectiveness of these programs is determined based on many community-specific contextual factors, such as location, and it may take several years to observe benefit. The programs are important tools for Alberta in developing a broader public health and harm-reduction response to the opioid epidemic.
Acknowledgements
The authors thank Rebecca Haines-Saah and Eldon Spackman for providing input on content and statistical analysis, as well as for providing background research critical to our paper. Access to study protocol, deidentified aggregate data or programming code can be requested via the main author. The authors also thank Colin Weaver for his contributions in developing the original statistical model that was refined throughout manuscript development.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Matthew Yeung contributed to data collection and protocol drafting. Riley Hartmann and Eddy Lang contributed to protocol development. Chel Hee Lee assisted with data analysis after review. All authors revised the manuscript, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: Funding was provided by the Alberta Health Services Department of Emergency Medicine for open access publication. No other support was received for this project.
Data sharing: Deidentified aggregate data are available on request from the corresponding author. The raw data cannot be released owing to protection by University of Calgary ethics policies.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/3/E537/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.