


Abstract
Background: Antimicrobial resistance is a rising threat to human health, and, with up to 90% of antibiotics prescribed in the community, it is critical to examine Canadian antibiotic stewardship practices in outpatient settings. We carried out a large-scale analysis of appropriateness in community-based prescribing of antibiotics to adults in Alberta, reporting on 3 years of data from physicians practising in the province.
Methods: The study cohort was composed of all adult (age 18–65 yr) Alberta residents who filled at least 1 antibiotic prescription written by a community-based physician between Apr. 1, 2017, and Mar. 6, 2020. We linked diagnosis codes from the clinical modification of the International Classification of Diseases, 9th Revision (ICD-9-CM), as used for billing purposes by the province’s fee-for-service community physicians, to drug dispensing records, as maintained in the province’s pharmaceutical dispensing database. We included physicians practising in community medicine, general practice, generalist mental health, geriatric medicine and occupational medicine. Following an approach used in previous research, we linked diagnosis codes with antibiotic drug dispensations, classified across a spectrum of appropriateness (always, sometimes never, no diagnosis code).
Results: We identified 3 114 400 antibiotic prescriptions dispensed to 1 351 193 adult patients by 5577 physicians. Of these prescriptions, 253 038 (8.1%) were “always appropriate,” 1 168 131 (37.5%) were “potentially appropriate,” 1 219 709 (39.2%) were “never appropriate,” and 473 522 (15.2%) were not associated with an ICD-9-CM billing code. Among all dispensed antibiotic prescriptions, amoxicillin, azithromycin and clarithromycin were the most commonly prescribed drugs labelled “never appropriate.”
Interpretation: We found that nearly 40% of prescriptions dispensed to 1.35 million adult patients in Alberta’s community-based settings over a 35-month period were inappropriate. This finding suggests that additional policies and programs to improve stewardship among physicians prescribing antibiotics for adult outpatients in Alberta may be warranted.
With few new antimicrobial drugs being developed and approved, resistant strains of bacteria are a rising threat to human health. A series of World Health Organization reports have highlighted the risk of a “post-antibiotic” era1 and have described antimicrobial resistance as “a global crisis that risks reversing a century of progress in health.”2 With the annual excess costs of antimicrobial resistance to Canada’s health care system estimated at $1.4 billion, the Council of Canadian Academies has deemed it to be a “looming public health threat and potential economic disaster.”3 Canada’s response has focused on tackling both the resistant bacteria — through surveillance and drug innovation programs — and curbing the use of antimicrobials across the spectrum of human and animal use.4
Particular attention has been paid to improving the stewardship behaviour of prescribers and patients alike. With up to 90% of antibiotics prescribed in the community rather than in acute care settings,5 interventions aimed at improving stewardship have been launched by Canada’s Choosing Wisely program6 and endorsed by the College of Family Physicians of Canada.7 This includes the Using Antibiotics Wisely program,5,6 introduced as a pan-Canadian initiative in 2018. The effects of these prescriber- and patient-focused education campaigns have been studied at the national and provincial levels.8 The literature describes modest decreases in overall antibiotic prescribing volume and recommends interventions beyond education,9 calling for an examination of not just the volume, but also the quality, of prescribing practices.10 As an example, a recent study suggested no significant changes in antibiotic prescribing patterns in community settings after the introduction of the Using Antibiotics Wisely campaign.10 The low uptake of stewardship recommendations among family physicians and the persistence of nonindicated antibiotic prescriptions11 suggest that a focus on appropriateness in community-based antibiotic prescribing12 is a necessary next step in developing effective policy and programming to improve stewardship.
Drawing on the administrative billing and drug dispensing data available from the provincial data custodian, we assessed the appropriateness of outpatient antibiotic prescribing for Alberta’s adult population. The assessment we describe here is important given the large variations that have been observed between regions.13 We also wished to improve comparative understandings of how a publicly funded single payer14,15 and private primary care systems12 perform.
Methods
Setting, data sources and study cohort
Alberta has a population of about 4 million.16 The province’s single health authority, Alberta Health Services, provides care in 5 geographic areas called health zones. The zones were created in 2009 and enable local decision-making in a fully centralized health care system. The zones respond to local conditions and act as integration points in province-wide health care programming (for more information, see https://www.albertahealthservices.ca/ahs-map-ahs-zones.pdf). The vast majority of community-based family physicians in the province operate independently of Alberta Health Services and bill the Ministry of Health directly on a fee-for-service basis as independent contractors. Primary health care policy in the province specifically seeks to attach patients to family physicians as part of delivering the Patient Medical Home care model.17
To assess the appropriateness of community-based antibiotic prescribing in Alberta, we linked the diagnosis codes from the clinical modification of the International Classification of Diseases, 9th Revision (ICD-9-CM), as used for billing purposes by community-based physicians, to drug dispensing records, as maintained in the province’s Pharmaceutical Information Network (PIN). The PIN system is a Web-enabled application that draws basic patient demographic data from a provincially held registry; prescriber data from family doctors’ electronic medical records and provincial registries; dispenser data and notes from community pharmacy systems; and drug information from national and private data banks.18
Our study cohort was composed of all adult (age 18–65 yr) Alberta residents who filled at least 1 antibiotic prescription written by a community-based physician between Apr. 1, 2017, and Mar. 6, 2020. We did not include children under the age of 18 years in our analysis, owing to data privacy and research ethics considerations. Likewise, we excluded adults aged 66 or older to facilitate comparisons with similar studies, such as that by Chua and colleagues.12 Our end date coincides with the first reported COVID-19 case in Alberta, a pandemic that brought unprecedented upheaval to the province’s primary care operations and prescribing practices.19–21 Our definition of community-based physician is based on Alberta Health Services’ categories and includes providers registered by the province’s Ministry of Health as working in community and family medicine, general practice, generalist mental health, geriatric medicine and occupational medicine. Our use of rural versus urban residence is based on Alberta Health Services’ official urban–rural continuum, which includes 7 distinct categories (metro, urban, moderate metro influence, moderate urban influence, rural, rural remote, and large rural centres and surrounding areas). The continuum was defined through the application of multiple criteria, including population density, local industry and distance from major urban centres (for more information, see https://open.alberta.ca/publications/official-standard-geographic-areas).
Targeted antibiotics and identifying antibiotic prescription dispensations
We reviewed prescribing data for the 40 most common antibiotic agents appearing on Alberta’s drug formulary, based on a 2019 analysis of the province’s antibiotic prescribing patterns by the College of Physicians and Surgeons of Alberta.22 We cross-referenced the active ingredients in these 40 agents against the Government of Canada’s national Drug Product Database, using Drug Identifier Numbers.23 From the 40 antibiotic agents, we identified 368 different individual drug products licensed for use in Canada (Appendix 1, Table S1, available at www.cmajopen.ca/content/11/4/E579/suppl/DC1).
Identifying appropriateness of antibiotic prescribing with ICD-9-CM diagnosis codes
Following an approach used in previous studies,24–27 Chua and colleagues12 developed a classification scheme that is applicable to a broad range of ICD-9-CM and International Classification of Diseases, 10th Revision administrative data sets. Their classification scheme is based on consensus reached between subject matter experts in antibiotic overuse and administrative data. It classifies each of the 17 553 diagnosis codes in the 2015 version of the ICD-9-CM as “always” if the associated condition is always or almost always an indication for antibiotic treatment, “sometimes” if the condition is a potential indication for antibiotic treatment, and “never” if the condition is almost never an indication for antibiotic treatment. Examples of these code assignments include “always” for ICD-9-CM code 486, labelled as “Pneumonia, organism unspecified;” “sometimes” for ICD-9-CM code 382.9, labelled as “Unspecified otitis media;” and “never” for ICD-9-CM code 466, labelled as “Acute bronchitis and bronchiolitis.”
Appendix 2 (available at www.cmajopen.ca/content/11/4/E579/suppl/DC1) lists all the ICD-9-CM codes and their classifications deployed to determine the appropriateness of antibiotic prescribing in this study. To facilitate comparison at scale with the study by Chua and colleagues,12 we chose to follow their scheme.
Categorizing prescription appropriateness based on billing codes
As Alberta’s PIN system does not report the indication that prompted a prescription or dispensation of a drug, we used ICD-9-CM codes submitted to the provincial payer by community-based prescribers to infer that indication. We followed the approach used in a range of administrative data–based studies examining diagnosis codes on billing claims that occurred in close temporal proximity to the dispensing of a prescribed drug.12,25,28 We applied this classification scheme to all ICD-9-CM billing codes generated during a “look-back” period that began 3 days before the day the antibiotic was dispensed and ended on the day the prescription was filled. We excluded all prescriptions marked as “refills” in the PIN data table. However, if a single patient was given antibiotics on multiple days during the look-back window, regardless of whether these antibiotics were the same or different drugs, these were included as separate dispensing events as long as they were not marked as “refills” in the PIN system.
We then assigned the prescribing of each dispensed antibiotic to 1 of 4 mutually exclusive categories: “appropriate” if at least 1 “always” diagnosis code was present on a claim on the day the prescription was filled or during the look-back period; “potentially appropriate” if at least 1 “sometimes” diagnosis code and no “always” diagnosis codes was present during the look-back period; “inappropriate” if associated only with “never” diagnosis codes; or “not associated” if there were no claims and therefore no diagnosis codes generated. Although prescribing appropriateness can be used in relation to initiation, duration or selection of antibiotic treatment, for our study’s purposes, we focused exclusively on appropriateness of initiation of antibiotic treatment (Figure 1).

Three-day look-back period for associating antibiotic dispensations with diagnosis codes, and example claims-based categorizations of dispensations.
Statistical analysis
We reported categoric variables with count and percentage. Tables were stratified by patient gender and health zone. We reported patient demographic data per patient, and appropriateness data per prescription. We performed frequency ranking to determine the antibiotics most commonly prescribed and the most frequent ICD-9-CM diagnoses associated with antibiotic prescriptions.
Sensitivity analysis
For our sensitivity analyses, we looked for a change in the proportions of dispensations assigned to each appropriateness category if we truncated or extended the duration of our look-back period. Specifically, in addition to our standard 3-day look-back period, we also examined diagnosis codes only on the same day as dispensations, as well as codes occurring in the 7 days before dispensations.
Ethics approval
The study was approved by the Conjoint Health Research Ethics Board, University of Calgary.
Results
Study population
Using the criteria outlined in the selection of our patient cohort, we identified 1 351 193 patients and 5577 providers. Of the 1 351 193 patients, 794 869 (58.8%) were registered as female and 556 323 (41.2%) as male (Table 1). In total, 503 001 patients (37.2%) were aged 18–34 years, 475 198 (35.2%) were aged 35–50 years, and 372 994 (27.6%) were aged 51–65 years. A total of 1 105 339 patients (81.8%) were registered as living in urban areas and 230 171 (17.0%) as living in rural locations; 15 683 patients (1.2%) were not classified along the urban–rural spectrum.
Demographic characteristics of Albertan adults who filled at least 1 antibiotic prescription written by a community-based physician between Apr. 1, 2017, and Mar. 6, 2020
Of the 1 351 193 patients, 1 306 944 (96.7%) contributed data across the full 3 years of the study period, 31 701 (2.3%) contributed to 2 years of data, and 12 548 (0.9%) contributed to 1 year of data.
Antibiotic prescription dispensations
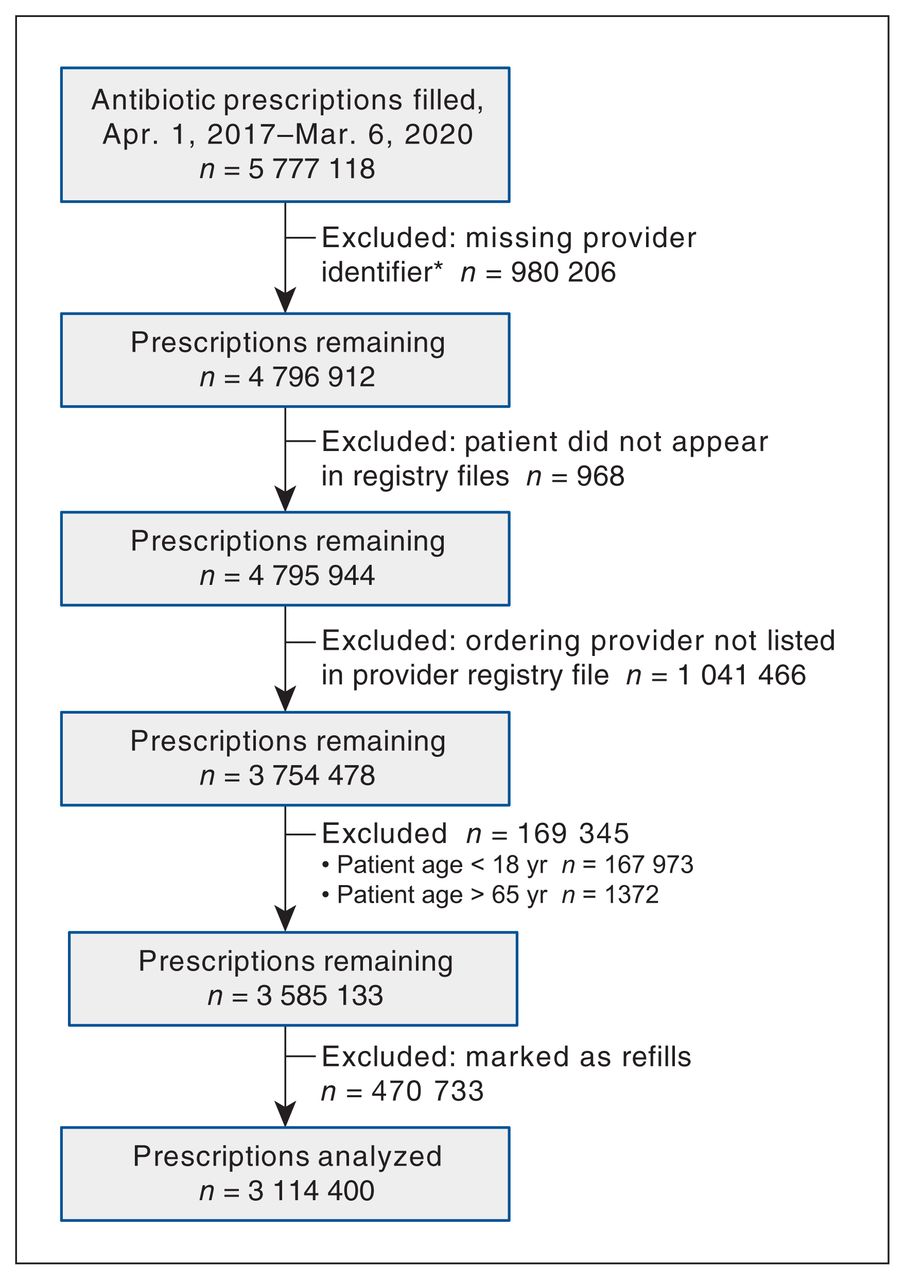
Over the study period, 5 777 118 prescriptions were filled for all 368 licensed antibiotic drug products. After exclusions, 3 114 400 prescriptions remained for analysis (Figure 2).
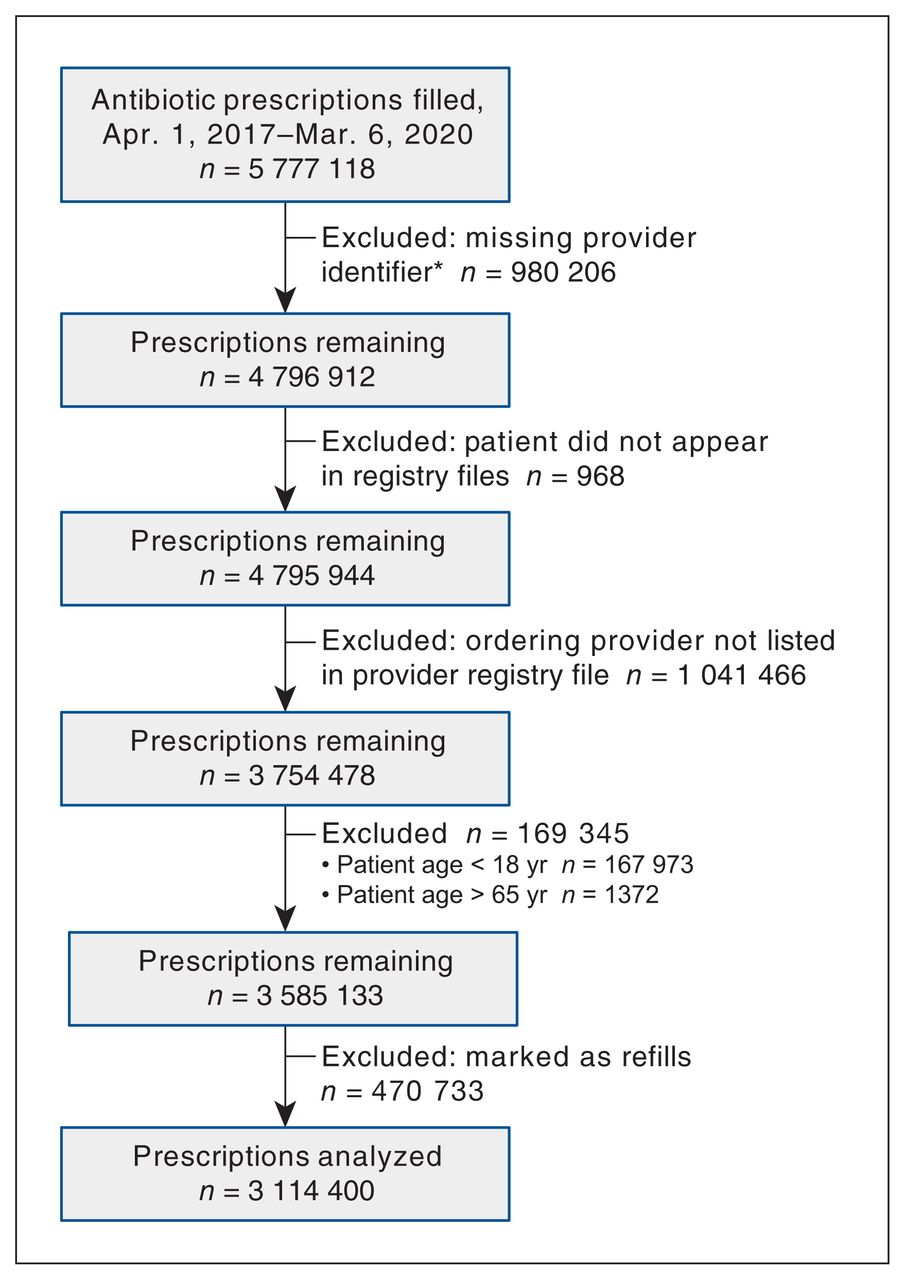
Flow chart showing identification of antibiotic prescriptions for analysis. *Random product of the data collection and maintenance routines of the Pharmaceutical Information Network system.
A total of 297 antibiotic drug products representing 51 unique antibiotic drugs were recorded as dispensed during the study period in the data set. Appendix 1, Tables S2 and S3 show the frequency at which various antibiotic prescriptions were dispensed, listing them from most to least common by World Health Organization anatomic therapeutic chemical designation (Table S2) and by drug identification number (Table S3). The most commonly filled antibiotic prescriptions were for amoxicillin (525 817 [16.9%]), azithromycin (334 553 [10.7%]) and cefalexin (301 548 [9.7%]). Based on ICD-9-CM codes, the 3 most frequent diagnoses that resulted in antibiotic prescribing were acute sinusitis (6.8%) (code 461), acute bronchitis and bronchiolitis (5.6%) (code 466) and cystitis (5.6%) (code 595).
With the 3-day look-back scenario, the distribution of dispensations showed a rapid decline after the day of the provider visit, with 2 583 653 dispensations (83.0%) recorded on the same day as the visit, 492 872 dispensations (15.8%) on days 1–3 of the look-back period and 254 473 dispensations (8.2%) on days 4–7 beyond this look-back period. The precipitous decline of dispensations after the day as recorded visits suggests that few dispensations were missed by setting the look-back window at 3 days.
Appropriateness of prescriptions
Of the 3 114 400 prescriptions, 253 038 (8.1%) were “always appropriate,” 1 168 131 (37.5%) were “potentially appropriate,” 1 219 709 (39.2%) were “never appropriate,” and 473 522 (15.2%) were not associated with an ICD-9-CM billing code (Appendix 1, Table S4). The most common antibiotics associated with dispensations classified as never appropriate were amoxicillin (223 067 [18.3%]), azithromycin (190 852 [15.6%]) and clarithromycin (106 745 [8.8%]).
The appropriateness of prescribing by gender, age and urban versus rural residence is shown in Table 2, Table 3 and Table 4, respectively. Nearly 40% of dispensed prescriptions were inappropriate, with older men receiving never appropriate prescriptions at a higher rate than women and younger people (Tables 2 and 3). Patients in the Edmonton zone received more never appropriate prescriptions than those in the province’s other health zones (Table 4 ).
Proportion of antibiotic prescriptions in each appropriateness category, by patient gender
Proportion of antibiotic prescriptions in each appropriateness category, by patient age
Proportion of antibiotic prescriptions in each appropriateness category, by health zone
Frequency of antibiotic prescriptions based on appropriateness
For the 253 038 antibiotic prescription dispenses labelled as always appropriate, the 3 most frequent diagnoses were “Acute cystitis” (ICD-9-CM code 595.0) (91 505 [36.2%]), “Urinary tract infection, site not specified” (code 599.0) (52 742 [20.8%]) and “Pneumonia, organism unspecified” (code 486) (19 124 [7.6%]). For the 1 168 131 dispensations identified as potentially appropriate, the 3 most frequent diagnoses were “Acute sinusitis” (code 461) (234 579 [20.1%]), “Acute pharyngitis” (code 462) (133 496 [11.4%]) and “Other cellulitis and abscess” (code 682) (127 898 [10.9%]). Finally, for the 1 219 709 dispensations labelled as never appropriate, the 3 most frequent diagnoses were “Acute upper respiratory infections of multiple or unspecified sites” (code 465) (147 252 [12.1%]), “Acute bronchitis and bronchiolitis” (code 466) (181 683 [14.9%]) and “General symptoms” (code 780) (114 102 [9.4%]).
Sensitivity analysis
The distribution among categories of appropriateness of antibiotic dispensations did not change substantially when we used a longer look-back period of 7 days or when we linked dispensations exclusively with same-day physician visits. With a 7-day look-back period, the proportion of prescriptions classified as never appropriate increased slightly, to 40.3%. When we used a same-day look-back period, the proportion of dispensations not associated with a recent diagnosis code increased to 24.5%, likely owing to processing or entry delays between the PIN and billing databases. However, in all instances, including our standard 3-day look-back period, the proportions of “potentially appropriate” and “never appropriate” dispensations remained within 2 percentage points of one another, and dispensations labelled “never appropriate” always accounted for the greatest proportion. Appendix 1, Table S4 shows the distribution of appropriateness for each of the 3 look-back periods.
Interpretation
This paper contributes to a growing literature on the definition and rate of appropriate antibiotic prescribing in the community.13,29 Whereas a previous Canadian study was smaller in scale and suggested relatively high levels of appropriateness, 29 our study provides a large-scale provincial-level analysis of appropriateness of community-based antibiotic prescribing, reporting on nearly 3 years of data from more than 5500 physicians practising across Alberta.
We used a previously validated, comprehensive classification scheme12 to determine the rates of appropriate antibiotic prescribing for adults in community settings by physicians in Alberta from 2017 to early 2020. Our study assessed 3.11 million antibiotic prescriptions dispensed to 1.35 million adult patients covered by Alberta’s single-payer health insurance system. Of the prescriptions dispensed, 253 038 (8.1%) were “always appropriate,” 1 168 131 (37.5%) were “potentially appropriate,” 1 219 709 (39.2%) were “never appropriate,” and 473 522 (15.2%) were not associated with an ICD-9-CM billing code.
Recent findings have suggested that more than 56% of patients receiving orally administered antibiotics in Alberta were prescribed them by community-based providers.22 We found that nearly 40% of these dispensations were inappropriate. This raises questions about the effectiveness of current antibiotic stewardship efforts. Our data also suggest that adult Albertans are more likely to receive antibiotics inappropriately than counterpart US patients, with Alberta having a substantially higher proportion of dispensations labelled “inappropriate” than a privately insured US cohort, 23.2%.12 Comparative policy and quality-improvement research initiatives are required to understand the potential mechanisms behind the lower proportion of inappropriate antibiotic dispensations in the United States. Our findings suggest that local variation in prescribing is a key feature in efforts to improve stewardship.
The proportion of inappropriate antibiotic dispensations we report here, 39.2%, may be assumed to be even higher, as our classification scheme erred toward assuming appropriateness of dispensations.12 The 2 diagnoses most commonly associated with “potentially appropriate” prescribing were acute sinusitis (14.8%) and acute pharyngitis (9.4%), both of which have been shown to have high rates of inappropriate or non–guideline adherent prescribing in primary care.30 In addition, with such a high proportion of inappropriate antibiotic prescriptions overall, it is likely that many of the dispensations identified as refills — which were excluded from analysis but accounted for about 13% of the total prescriptions in our data set — represent refills of previously inappropriate prescriptions. Even if the original prescription was appropriate, the refills may have been for conditions that do not require prolonged courses of antibiotics.
Beyond further comparative research to understand the organizational, payment and quality-improvement structures of jurisdictions where inappropriate prescribing is less prevalent, novel stewardship approaches such as restrictions on community-based antibiotic prescribing and audit programs to increase provider accountability may warrant consideration.
It is important to acknowledge that, although the number of inappropriate prescriptions in our study was high, the most frequently prescribed antimicrobials — amoxicillin, azithromycin and cefalexin — are relatively narrow-spectrum, targeted-type antibiotics, as opposed to the use of fluoroquinolones or amoxicillin–clavulanate.
Our results diverge from findings of other studies indicating that women are prescribed antibiotics more frequently than men31 but not necessarily more inappropriately. 32 Our data suggest that, although a higher proportion of women than men received antibiotic prescriptions, a higher proportion of men than women received “never appropriate” prescriptions. However, this difference may be explained in part by the fact that cystitis — a diagnosis categorized in this study as an “always appropriate” condition — is more common in women than in men.33,34
Taken together, the variations in antibiotic prescribing we report here strongly support the need to not only establish the extent to which other provincial systems have similar or varying proportions of inappropriate dispensations, but also address Alberta’s particular stewardship policy requirements considering these findings. Similarly, more research needs to be done on the role patient sex and gender play in cases in which a patient receives an inappropriate prescription.
Limitations
Our analyses relied on aggregated administrative data sets that are not designed to be linked together or intended for purposes of research data collection. Limitations and errors in data collection, processing and maintenance meant that portions of our data sets had to be excluded in order to complete our analyses. Over our 3-year look-back window, missing data accounted for 981 147 dispensations (about 17% of the total dispensations). This rate of missing data is in line with previous research in which Alberta’s patient and provider registries and PIN databases during this period were used.35
Diagnosis codes assigned by clinicians for billing purposes may not fully represent patient conditions or provider experiences in the clinical setting. Clinicians may neglect to code the actual condition for which they are prescribing antibiotics or use inappropriate codes to justify antibiotic prescribing. Large numbers of prescriptions for antibiotics in the outpatient setting lack a properly documented indication, even in patient medical charts.36 For example, in our study, one of the most frequent ICD-9-CM diagnostic codes associated with dispensations labelled as never appropriate was 780 (“General symptoms”), which suggests that these are very high-level codes used for administrative billing purposes, rather than for specific conditions or actual diagnoses given to a patient by a provider in the context of routine care. More validation is needed to assess the reliability of diagnostic codes in reflecting the underlying reasons for antibiotic prescriptions.
We excluded children younger than 18 years from data analysis for privacy, data quality and ethical reasons. As a result, we were not able to compare antibiotic prescribing rates and appropriateness between children and adults. Furthermore, our findings are applicable only to adults aged 18–65 years.
Our assessment of inappropriate prescribing focused on inappropriate or unnecessary antibiotic drug dispensations and did not analyze inappropriate treatment durations or inappropriate selection of antibiotic agents. All 3 components are important targets of antimicrobial stewardship efforts, but our findings are restricted to inappropriate initiation of antibiotic treatment.
Conclusion
This study provides a large-scale analysis of the appropriateness of adult antibiotic prescribing by community-based providers in Alberta. It also shows the adaptability and applicability of a previously validated methodology for assessing appropriateness with the use of ICD-9-CM diagnosis codes by applying it in a Canadian context. This suggests that similar analyses could be conducted in other provinces to identify and compare trends in prescribing appropriateness, as well as monitor the relative effectiveness of stewardship policies and programs.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Myles Leslie is lead author, conceived of and designed the study, and led the data acquisition negotiations, with contributions from Raad Fadaak. Brendan Lethebe and Jessie Hart Szostakiwskyj analyzed the data. Myles Leslie drafted the manuscript, with contributions from Raad Fadaak, Brendan Lethebe and Jessie Hart Szostakiwskyj. All of the authors interpreted the data, revised the manuscript critically for important intellectual content, approved the final version to be published and agreed to be accountable for all aspects of the work.
Funding: This research is part of the Antimicrobial Resistance (AMR) – One Health Consortium, funded by the Major Innovation Fund program of the Ministry of Jobs, Economy and Innovation, Government of Alberta (grant RCP-19-003-MIF).
Data sharing: All data were obtained in pre-anonymized form from the Health Standards, Quality and Performance Division, Alberta Health, under ethics approval from the University of Calgary and cannot be shared in disaggregated form with others. Interested parties may submit a request to access these administrative data sets for research, planning, policy development or quality-improvement projects by visiting https://www.alberta.ca/health-research.aspx.
Disclaimer: This study is based in part on data provided by Alberta Health. The interpretation and conclusions contained herein are those of the researchers and do not necessarily represent the views of the Government of Alberta. Neither the government nor Alberta Health express any opinion in relation to this study.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/4/E579/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/.
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
Article tools





