


Abstract
Background: European studies have shown that nonfasting remnant cholesterol can be a strong predictor of cardiovascular disease risk and may contribute to identifying residual risk; however, Canadian data are lacking on nonfasting remnant cholesterol. In this study, we aimed to determine the relation between nonfasting remnant cholesterol, low-density lipoprotein (LDL) cholesterol and cardiovascular disease among people in Alberta.
Methods: In this retrospective analysis, we used data from Alberta’s Tomorrow Project, a large prospective cohort that enrolled Albertans aged 35–69 years (2000–2015). Participants with consent to data linkage, with complete nonfasting lipid data and without existing cardiovascular disease were included. The nonfasting remnant cholesterol and LDL cholesterol relation with a composite cardiovascular disease outcome of major incident cardiovascular diagnoses, ascertained by linking to Alberta Health databases, was determined by multivariable logistic regression, adjusting for age, sex, statin use, comorbidities, and LDL cholesterol or remnant cholesterol.
Results: The final sample of 13 988 participants was 69.4% female, and the mean age was 61.8 (standard deviation [SD] 9.7) years. Follow-up time was approximately 15 years. Mean remnant cholesterol was significantly higher among individuals with versus without cardiovascular disease (0.87 [SD 0.40] mmol/L v. 0.78 [SD 0.38] mmol/L, standardized mean difference [SMD] −0.24), and mean LDL cholesterol was significantly lower (2.69 [SD 0.93] mmol/L v. 2.88 [SD 0.84] mmol/L, SMD 0.21). The odds of incident composite cardiovascular disease were significantly increased per mmol/L increase in remnant cholesterol (adjusted odds ratio [OR] 1.48, 95% confidence interval [CI] 1.27–1.73) but significantly decreased per mmol/L increase in LDL cholesterol (adjusted OR 0.73, 95% CI 0.68–0.79).
Interpretation: In this large Albertan cohort of predominantly older females, nonfasting remnant cholesterol had a positive relation with cardiovascular disease incidence, whereas LDL cholesterol did not. These findings support the clinical utility of measuring non-fasting remnant cholesterol to detect cardiovascular disease risk.
In Canada, the primary lipid-screening measure for cardiovascular disease is fasting low-density lipoprotein (LDL) cholesterol.1 Despite fasting LDL cholesterol being a central screening and treatment target for dyslipidemia, substantial proportions of the population receiving statin therapy (including those with insulin resistance and diabetes) retain considerable residual cardiovascular disease risk.2 Nonfasting remnant cholesterol has emerged as a marker of cardiovascular disease risk.3
Nonfasting remnant cholesterol originates from both the liver (very-low-density lipoprotein remnants) and intestine (chylomicron remnants) and can be readily calculated using existing lipid panel criteria from samples drawn during the nonfasting state.4 Longitudinal data from Europe have shown that a nonfasting lipid profile deviates only minimally from a fasting lipid profile.5,6 Circulating nonfasting remnant cholesterol has also been shown to be a strong, independent predictor of cardiovascular disease risk in European populations.4,5 Indeed, Varbo and colleagues reported that risk of ischemic heart disease was 2.8 times greater for every 1 mmol/L increase in nonfasting remnant cholesterol.4 Nonfasting lipid assessment has been added to lipid screening guidelines in Europe and, more recently, to Canadian and American guidelines. 1,7,8 However, whereas key data on nonfasting remnant cholesterol have been published in Europe, an important void exists in North America. In 2012, Sidhu and Naugler determined nonfasting lipid values using community laboratory data in a cohort in Alberta to characterize the effect of fasting time on plasma lipid subclasses, which was found to be minimal. 9 The authors were unable to analyze the effect on cardiovascular disease.9 More recently, Lawler and colleagues used an Ontario-based population with atherosclerotic cardiovascular disease to report on the association of hypertriglyceridemia with atherosclerotic cardiovascular disease. This study calculated remnant cholesterol but did not contrast the atherosclerotic cardiovascular disease risk relation with remnant cholesterol values.10 Currently, the lack of Canadian data regarding nonfasting remnant cholesterol, its normative range in the population and its association with cardiovascular disease limits its clinical utility in Canada.
The purpose of this study was to calculate nonfasting remnant cholesterol in the Alberta’s Tomorrow Project (ATP) large prospective cohort and compare the levels of remnant cholesterol and LDL cholesterol in those with and without incident cardiovascular disease. We hypothesized that both nonfasting remnant cholesterol and LDL cholesterol would yield strong positive relations with incidence of cardiovascular disease.
Methods
The present study is a retrospective analysis of ATP, a longitudinal cohort developed to study the etiology of cancer and chronic disease in Canada.11 Phase 1 enrolment of participants (aged 35–69 yr) occurred between 2000 and 2008. Phase 2 enrolment occurred between 2009 and 2015 when ATP merged with the national Canadian Partnership for Tomorrow’s Health, for a total ATP cohort of 52 769 participants who provided their consent for administrative data linkage.12 Participants completed enrolment (for new participants) and follow-up (for existing participants) health and lifestyle surveys from 2000 to 2015, which collected information about demographic characteristics, personal and family health history, and lifestyle behaviours (Appendix 1, available at www.cmajopen.ca/content/11/4/E645/suppl/DC1). Participants were also invited to attend a study centre between 2008 and 2015 to provide blood samples and physical measurements. At enrolment, participants were asked for consent for use of their data and samples for research purposes and to link with administrative health databases. Recruitment and enrolment data for ATP are described in further detail elsewhere.11–14 The present study was reported using the Strengthening the Reporting of Observational Studies in Epidemiology statement for cohort studies.15
Participants
The present analysis included a subset of ATP participants who provided blood samples at a study visit and which had been processed at the time of data linkage (i.e., blood samples had undergone lipid analysis), and those who consented to follow-up through administrative health data linkage and provided their personal health number. Those who had missing date of blood draw variables, incomplete lipid panel data, calculated remnant cholesterol and LDL cholesterol of 0 mmol/L or less, triglycerides of 4.5 mmol/L or greater, and prevalent cardiovascular disease were excluded. Prevalent cardiovascular disease was determined through linkage to administrative health data and defined as relevant cardiovascular disease diagnoses or procedures (see “Variables and outcomes” section) within 6 months of ATP enrolment.
Data sources
Health and lifestyle survey data from 2001 to 2015 were used to obtain participant characteristics, including age and sex. Details on data coding may be found on the ATP website (https://myatpresearch.ca/data-dictionaries/). At the time of collection in the study centres (2008–2015), nonfasting blood samples (~50 mL) were drawn and separated into plasma and serum for storage at −80°C in the ATP biobank12,13 (Appendix 1). In 2017–2020, 0.5 mL of serum from every participant who had provided a blood sample underwent lipid panel analysis (including high-density lipoprotein [HDL] cholesterol, triglycerides and total cholesterol) by Calgary Laboratory Services, an accredited clinical laboratory providing medical diagnostic laboratory services in Alberta. Serum HDL cholesterol, triglycerides and total cholesterol were directly measured, and LDL cholesterol, non-HDL cholesterol and non-fasting remnant cholesterol were calculated using the Friedewald formula (for LDL cholesterol) or as residual from total cholesterol (for non-HDL cholesterol and remnant cholesterol) (Appendix 1).5
Cardiovascular disease outcomes (described in “Variables and outcomes” section), statin drug use and other comorbidity data were obtained via data linkage using participant personal health numbers from Alberta Health, including physician claims, Discharge Abstract Database, emergency department, Pharmaceutical Information Network and Alberta Blue Cross data sets from 2000 to 2015. Statin use, identified by Anatomical Therapeutic Chemical coding, was obtained from Alberta Blue Cross and Alberta’s Pharmaceutical Information Network data sets, which capture all statin use irrespective of age or formulary status. Statin users were considered to be participants who were prescribed a statin before diagnosis of cardiovascular disease. The Elixhauser Comorbidity Index was generated based on 30 different identified comorbid conditions within the physician claims, Discharge Abstract Database and emergency department data sets. There were no overlapping conditions between the index and incident cardiovascular disease outcomes (Appendix 2, available at www.cmajopen.ca/content/11/4/E645/suppl/DC1).16,17
Variables and outcomes
Remnant cholesterol and LDL cholesterol concentration of nonfasting blood samples were the primary explanatory variables in the present analysis. Covariates used in adjusted models included age and sex (self-reported from ATP survey data sets12), statin use and the Elixhauser Comorbidity Index (described in the “Data sources” section).
Individual-level information on cardiovascular disease and related medical procedures was obtained from ATP personal linked health care data, including data from physician claims and the Discharge Abstract Database. Cases of cardiovascular disease were identified by the International Statistical Classification of Diseases and Related Health Problems codes, and procedures were identified by the Canadian Classification of Diagnostic, Therapeutic, and Surgical Procedures codes, using the definitions of the Alberta Diabetes Surveillance System (Appendix 2).18 Incidence was defined as occurring in those without prevalent cardiovascular disease (i.e., cardiovascular disease diagnosis or procedures [percutaneous coronary intervention and coronary artery bypass graft] before or within 6 months of enrolment to ATP, or within 1 year of linkage to Alberta Health data). Incident composite cardiovascular disease was the primary outcome and was an aggregate of cardiovascular disease diagnoses, including ischemic heart disease, myocardial infarction, angina, heart failure, transient ischemic attack and acute ischemic stroke, similar to the definition used by Clair and colleagues.19 Where participant numbers allowed, these diagnoses analyzed either individually or aggregated by similar diagnosis were considered as secondary outcomes. For example, myocardial infarction and angina were aggregated as acute coronary syndrome, and transient ischemic attack and acute ischemic stroke as stroke.
Statistical analysis
Data were analyzed using Stata/SE version 16.1 (StataCorp). We calculated means and standard deviations (SDs) for descriptive statistics of continuous variables. Baseline means for participants with and without incident cardiovascular disease were compared using standardized difference. We used univariable logistic regression to determine the unadjusted odds ratios (ORs) and confidence intervals (CIs) for the association between nonfasting lipids (remnant cholesterol and LDL cholesterol) as both continuous and categorical (quartile) explanatory variables, and incident cardiovascular disease. To further explore this relation, we used multivariable logistic regression to determine the adjusted ORs and 95% CIs and for the relations between remnant cholesterol and LDL cholesterol variables and cardiovascular disease outcomes. We used 2 adjusted models (1 for continuous and 1 for categorical lipid variables), and each included remnant cholesterol, LDL cholesterol, age, sex, statin use and Elixhauser Comorbidity Index. These models were stratified in turn by sex and statin use. In addition, we used univariable and multivariable Cox proportional hazard regression models (1 for continuous and 1 for categorical lipid variables) including remnant cholesterol, LDL cholesterol, age, sex, statin use and Elixhauser Comorbidity Index to determine the relation between remnant cholesterol, LDL cholesterol and the primary cardiovascular disease outcome, while adjusting for follow-up time. We considered a p value less than 0.05 statistically significant.
In an exploratory analysis, we assessed the relation between nonfasting lipids and prevalent cardiovascular disease. Analyses were similar to those completed for incident cardiovascular disease.
Ethics approval
The former Alberta Cancer Board Research Ethics Committee and the University of Calgary Conjoint Health Research Ethics Board approved the recruitment and data collection for ATP.14 The present analysis of nonfasting lipids in the ATP cohort and linkage to Alberta Health administrative data was approved by the University of Alberta Research Ethics Board (Pro00073641 and Pro00058561, respectively).
Results
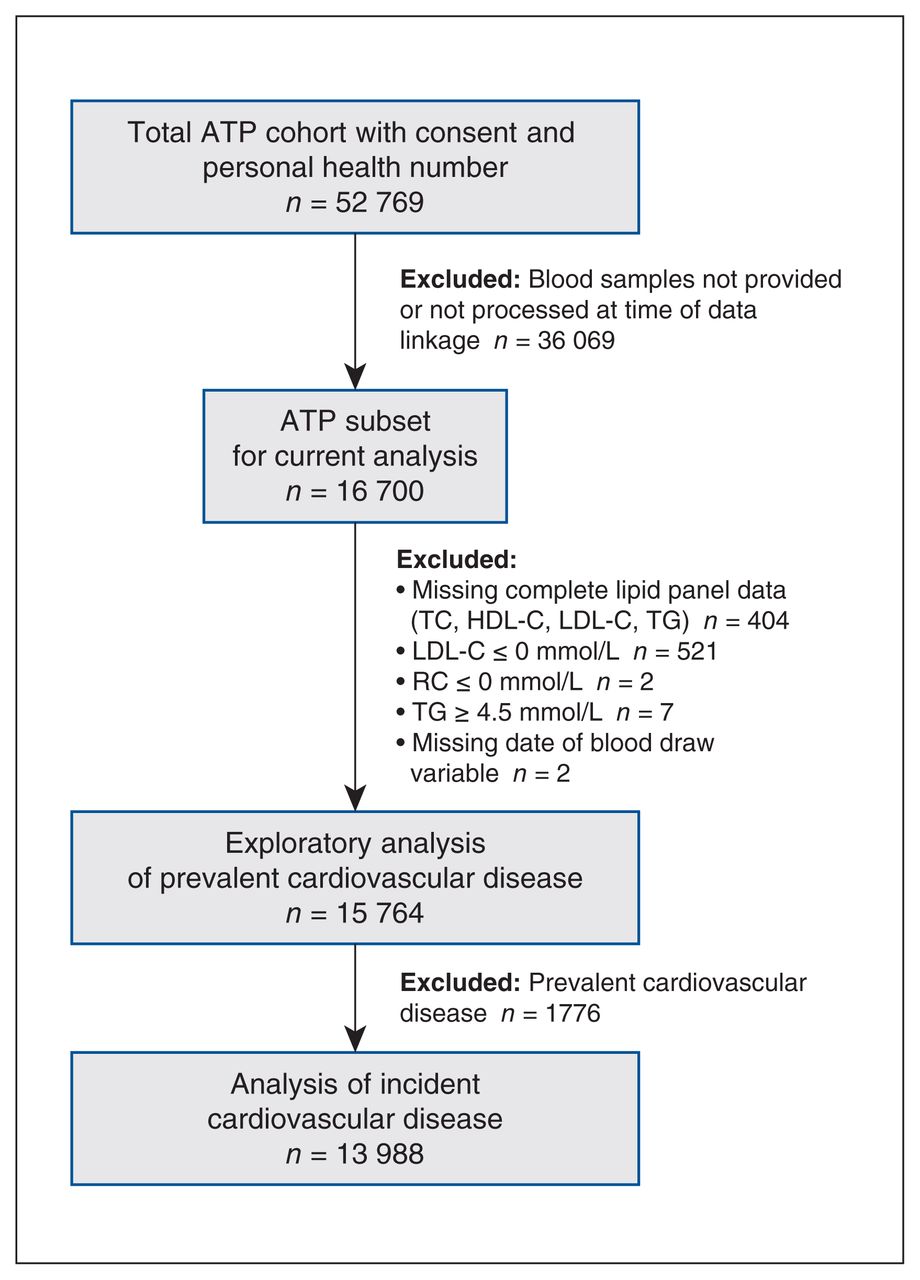
The sample used in the analysis of incident cardiovascular disease included 13 988 of the 52 769 in the ATP cohort (Figure 1). The mean age was 61.8 years, 69.4% were female and 18.9% were taking statins (Table 1). Few clinical differences were observed between included and excluded participants (Appendix 3, Supplemental Table 1, available at www.cmajopen.ca/content/11/4/E645/suppl/DC1). There were 1156 participants with incident cardiovascular disease over the course of nearly 15 years of follow-up (Table 1). Statin use increased with quartiles of remnant cholesterol, but was highest in quartile 1 of LDL cholesterol (Figure 2). The group with incident cardiovascular disease was on average older and had a greater proportion of statin users, but had lower Elixhauser Comorbidity Index scores and a lower proportion of females than the group without incident cardiovascular disease (Table 1).

Flow diagram of Alberta’s Tomorrow Project (ATP) participant selection. Note: HDL-C = high-density lipoprotein cholesterol, LDL-C = low-density lipoprotein cholesterol, RC = remnant cholesterol, TC = total cholesterol, TG = triglycerides.
Baseline cohort characteristics and nonfasting lipid panel

Percentage of incident composite cardiovascular disease (CVD) diagnoses and statin users by quartile of nonfasting remnant cholesterol (RC) (A) and low-density lipoprotein cholesterol (LDL-C) (B). Green bars = cardiovascular disease; blue dots = statin users. Categorical lipid variables were used in the regressions; however, the figure shows quartiles plotted at the mean lipid value for each quartile. Note: Q = quartile. Figure created using GraphPad Prism version 9.3.1.
Individuals with incident cardiovascular disease had higher mean nonfasting remnant cholesterol and triglycerides but lower LDL cholesterol, HDL cholesterol, total cholesterol and non-HDL cholesterol than those without cardiovascular disease (Table 1). Similar results for the primary lipids of interest were seen for prevalent cardiovascular disease (Appendix 3, Supplemental Table 2).
Unadjusted and adjusted odds ratios of cardiovascular disease incidence per mmol/L increase of nonfasting remnant cholesterol and low-density lipoprotein cholesterol
Composite cardiovascular disease incidence per mmol/L increase of nonfasting remnant cholesterol and LDL cholesterol
After covariate adjustment, participants had 1.48 (95% CI 1.27–1.73) times the odds of incident composite cardiovascular disease per mmol/L increase of remnant cholesterol. In contrast, participants had 0.73 (95% CI 0.68–0.79) times the odds of incident composite cardiovascular disease per mmol/L increase in LDL cholesterol (Table 2; Figure 3; Appendix 3, Supplemental Table 3). The ability of remnant cholesterol to identify increased risk of cardiovascular disease remained greater than that of LDL cholesterol when the latter was not adjusted for in the statistical model, and vice versa (Appendix 3, Supplemental Table 4). Results from the Cox regression were similar, and few differences were seen by sex and statin use (Appendix 3, Supplemental Tables 5–7).
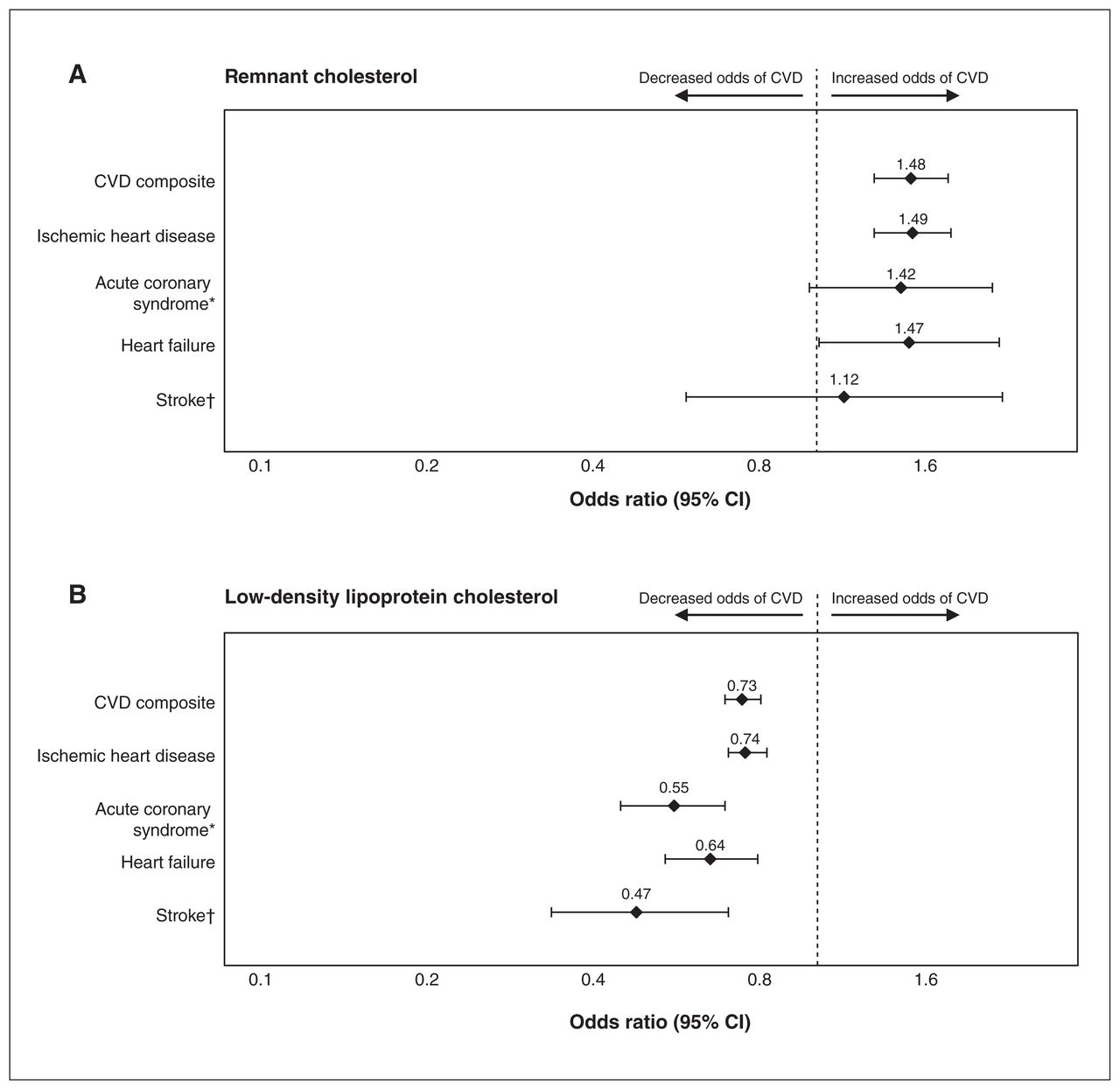
Odds ratios and 95% confidence intervals (CIs) for cardiovascular disease (CVD) incidence per mmol/L increase of nonfasting remnant cholesterol (A) and low-density lipoprotein cholesterol (B) on a logarithmic scale. Adjusted model for (A) and (B) included sex, age, Elixhauser Comorbidity Index, statin use, remnant cholesterol and low-density lipoprotein cholesterol. *Aggregate of myocardial infarction and angina. †Aggregate of acute ischemic stroke and transient ischemic attack.
Unadjusted and adjusted odds ratios of composite cardiovascular disease incidence by quartile of nonfasting remnant cholesterol and low-density lipoprotein cholesterol
Composite cardiovascular disease incidence by quartile of nonfasting remnant cholesterol and LDL cholesterol
Quartiles 3 and 4 of nonfasting remnant cholesterol were significantly associated with increased adjusted odds of incident composite cardiovascular disease in comparison to quartile 1 (adjusted OR 1.38 [95% CI 1.15–1.67] and adjusted OR 1.46 [95% CI 1.22–1.76], respectively). Individuals with nonfasting LDL cholesterol in quartiles 2–4 had adjusted ORs of 0.63 (95% CI 0.53–0.75), 0.52 (95% CI 0.44–0.63) and 0.52 (95% CI 0.43–0.62), respectively, of incident composite cardiovascular disease compared with those in quartile 1 (Table 3; Appendix 3, Supplemental Table 8).
Few differences were seen by sex and statin use, and results from the Cox regression were similar (Appendix 3, Supplemental Tables 9–11).
Association between nonfasting remnant cholesterol, LDL cholesterol and secondary outcomes
Despite attenuation of significance, the adjusted relation of both nonfasting remnant cholesterol and LDL cholesterol with secondary outcomes of incident cardiovascular disease generally followed similar trends to that of the composite cardiovascular disease outcome, regardless of sex or statin use (Table 2; Figure 3; Appendix 3, Supplemental Tables 6 and 7).
The relations of continuous and categorical variables with primary and secondary outcomes of prevalent cardiovascular disease were generally similar to those from incident cardiovascular disease outcomes, regardless of sex or statin use (Appendix 3, Supplemental Tables 12–18).
Interpretation
The current study demonstrates a relation of nonfasting remnant cholesterol with cardiovascular disease in a large population in Alberta. Although the absolute difference in mean lipids between those with and without cardiovascular disease was not large, remnant cholesterol (but not LDL cholesterol) was associated with increasing odds of cardiovascular disease incidence. The frequency of statin users increased with remnant cholesterol quartiles and did not appear to influence diagnoses of cardiovascular disease.
A US study has shown that nonfasting triglyceride levels have a stronger positive association with cardiovascular disease than fasting triglyceride levels.20 A recent study from Ontario, Canada, showed that hypertriglyceridemia was positively associated with cardiovascular disease events under conditions of pre-existing atherosclerotic cardiovascular disease (possibly, as noted by the authors, owing to cholesterol content of triglyceride-rich lipoproteins).10 The median remnant cholesterol value for those with atherosclerotic cardiovascular disease was 0.6 (interquartile range [IQR] 0.4–0.8) mmol/L,10 which is lower than that observed in the present study (mean 0.78 [SD 0.38] mmol/L). The authors were unable to verify fasting or nonfasting status of the participants; therefore, one explanation for this could be a higher proportion of sampling in the fasted state, relative to sampling in the nonfasted state for the present cohort. In contrast, 3 large European cohort studies in Copenhagen have previously demonstrated a causal relation between nonfasting remnant cholesterol and cardiovascular disease.4,21 The nonfasting remnant cholesterol values in the ATP cohort were indeed comparable to values from these Copenhagen cohorts (which ranged from median 0.6 [IQR 0.4–0.9] mmol/L to 0.7 [IQR 0.5–1.0] mmol/L).4 However, the Copenhagen cohorts also observed a positive relation of LDL cholesterol with cardiovascular disease risk, contrary to the current analysis. We note the time frame of blood sampling in the Copenhagen cohorts was 1991–2009, and the time frame for ATP was 2008–2015, which could affect this relation. Finally, a recent study by Castañer and colleagues found no relation between LDL cholesterol and cardiovascular disease in a high-risk cohort from Spain.22
In the present study, we observed an inverse relation between LDL cholesterol and cardiovascular disease incidence. The highest number of statin users was observed in association with the lowest quartile of LDL cholesterol and the highest number of cardiovascular disease diagnoses. It has been reported that certain high-risk populations, such as those with diabetes, are often at elevated risk of cardiovascular disease despite lowering LDL cholesterol through statin use (this is termed residual risk).23 These results also align with studies in humans and rodent models with dyslipidemia showing that statins, which reduce cholesterol synthesis in the liver, may also induce an upregulation of absorption and secretion of cholesterol in the intestine.24,25 Thus, it is likely that a subpopulation of statin users who remained at high risk of cardiovascular disease, despite lower LDL cholesterol levels, drove the inverse relation observed in the present analysis. Factors such as statin compliance, dose and strength were not available for use in this analysis and may be sources of residual confounding. However, this relation is not unique to the ATP cohort. Of note, Danish general population studies have observed null relations between nonfasting LDL particle concentration, LDL cholesterol concentration and cardiovascular outcomes.26,27 Several high-risk cohorts from Germany, China and Spain have also demonstrated null and inverse relations between fasting or nonfasting LDL cholesterol concentration and cardiovascular outcomes.22,28–30
Currently, there are few standard pharmacologic therapies to reduce nonfasting remnant cholesterol or hypertriglyceridemia. Statins tend to have a mixed or null effect on triglycerides and triglyceride-rich lipoproteins, and therefore may not influence nonfasting remnant cholesterol per se.31 The outcomes of the Reduction of Cardiovascular Events with Icosapent Ethyl–Intervention Trial suggest additional benefit of triglyceride lowering to patients with already well-controlled LDL cholesterol.32 Alternatively, in statin-treated individuals with high LDL cholesterol, ezetimibe is recommended to further reduce cardiovascular disease risk.1,33 For those who are statin intolerant, other drugs such as bempedoic acid are being investigated.34
We postulate that adding nonfasting remnant cholesterol to the management of atherosclerotic cardiovascular disease risk may further benefit these populations with elevated risk of residual cardiovascular disease. Future work will need to delineate the predictive power of nonfasting remnant cholesterol, explore its utility as a novel or adjunct marker of cardiovascular disease risk in Canada, and validate the relation between remnant cholesterol and cardiovascular disease in other samples of Canadian populations. It will be important to determine normative reference values of nonfasting remnant cholesterol that can be used by physicians in Canada. Given similarities between the distribution range of remnant cholesterol in both Canada and Europe, it may be possible to consider the utility of European reference values for practice in Canada.5
Limitations
This study used a calculated estimate of remnant cholesterol. However, it closely correlates with nonfasting triglycerides and measured remnant cholesterol (R2 = 0.93 and 0.86, respectively), and recent studies have shown that calculated remnant cholesterol values can be adopted in a clinical setting for prognostic, predictive and therapeutic purposes.31,35 In future, there may be more reliable, cost-effective options available for direct measurement of remnant cholesterol, such as using nuclear magnetic resonance.36 In the meantime, a calculated measurement can be used in a nonfasting/ambulatory care context, which may provide additional options for clinicians at point of care.
Longitudinal studies by their nature make use of older data; although the data have been collected over many years, the clinical practice for cholesterol management has not changed and the results presented here are still applicable in today’s practice. The use of administrative data also has inherent limitations, including reliance on human reporting by health professionals leading to possible measurement error. However, errors were likely nondifferential based on remnant cholesterol levels and, if anything, would present a bias toward a null OR. Similarly, although a large proportion of ATP participants were excluded from the present analysis, there were few clinical differences compared with those included (Appendix 3, Supplemental Table 1), and any differences would not present a true selection bias as the calculation of remnant cholesterol had no bearing on the diagnosis of cardiovascular disease.
Logistic regression models do not account for differential follow-up time, which is a potential limitation of the present analysis. However, using a method such as Cox regression generates results that are more difficult to interpret in clinical settings, and when primary outcome analyses were repeated with Cox regression (Appendix 3, Supplemental Tables 5 and 11), the results were similar. Furthermore, because remnant cholesterol is a relatively new area of study, less is known about which factors to adjust for in analyses and there may be some residual confounding. Another limitation is the smaller case numbers for secondary outcomes, which likely drove the loss of significance due to reduced statistical power.
Although the ATP cohort provides some unique insights into the relation of remnant cholesterol and cardiovascular disease, it is composed primarily of older females, and findings may not be generalizable to the overall Canadian population. Indeed, differences have been found between the ATP cohort and the general population.12 Older women represent a group at high absolute risk for cardiovascular disease, due in part to perimenopausal changes in lipid levels,37 and are an important group in which to study this relation; however, measures of relative risk as presented in this analysis are likely not greatly affected.
Conclusion
Although generalization of these results to the overall Canadian population may be premature, the data from this cohort suggest that nonfasting remnant cholesterol is significantly associated with increased risk of cardiovascular disease. Nonfasting remnant cholesterol may be a useful adjunct target for reduction of cardiovascular disease risk, especially in the context of well-controlled LDL cholesterol and high statin use.
Acknowledgements
Alberta’s Tomorrow Project is only possible because of the commitment of its research participants, its staff and its funders: Alberta Health, Alberta Cancer Foundation, Canadian Partnership Against Cancer and Health Canada, and substantial in-kind funding from Alberta Health Services.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Olivia Weaver analyzed and interpreted data from Alberta’s Tomorrow Project (ATP) and wrote the final version of the manuscript. Jacqueline Krysa analyzed and interpreted data from ATP and contributed to the original study design. Ming Ye and Dean Eurich acquired data from ATP and provided data linkage for cardiovascular disease outcome analysis. Dean Eurich contributed to the original study design and data interpretation. All coauthors contributed to revising the manuscript. Spencer Proctor was the inceptor of the work and contributed to the study design and its interpretation. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: Jacqueline Krysa received the Alberta Diabetes Institute Graduate Student Fellowship, and Spencer Proctor received a Pilot Study Grant from the Alberta Diabetes Institute. Indirect funding contributions were also provided by Women and Children’s Health Research Institute and Alberta Health Services — Health Outcomes Improvement Fund.
Data sharing: Access to ATP data for research purposes may be granted on approval of request submitted to Alberta’s Tomorrow Project. Further details to access ATP data is available from www.myATP.ca or by email to ATP.Research{at}ahs.ca.
Disclaimer: The views expressed herein represent the views of the authors and not of Alberta’s Tomorrow Project or any of its funders. This study is based in part on data provided by Alberta Health. The interpretation and conclusions contained herein are those of the researchers and do not necessarily represent the views of the Government of Alberta. Neither the government nor Alberta Health express any opinion in relation to this study.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/4/E645/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools





