


Abstract
Background: Diabetic eye complications are the leading cause of visual loss among working-aged people. Pharmacy-based teleophthalmology has emerged as a possible alternative to in-person examination that may facilitate compliance with evidence-based recommendations and reduce barriers to specialized eye care. The objective of this study was to estimate the cost-effectiveness of mobile teleophthalmology screening compared with in-person examination (primary care) for the diabetic population residing in semiurban areas of southwestern Ontario.
Methods: A decision tree was constructed to compare in-person examination (comparator program) versus pharmacy-based teleophthalmology (intervention program). The economic model was designed to identify patients with more than minimal diabetic retinopathy, manifested by at least 1 microaneurysm at examination (modified Airlie House classification grade of ≥ 20). Cost-effectiveness was assessed as cost per case detected (true-positive result) and cost per case correctly diagnosed (including true-positive and true-negative results).
Results: The cost per case detected was $510 with in-person examination and $478 with teleophthalmology, and the cost per case correctly diagnosed was $107 and $102 respectively. The incremental cost-effectiveness ratio was $314 per additional case detected and $73 per additional case correctly diagnosed. Use of pharmacologic dilation and health care specialists' fees were the most important cost drivers.
Interpretation: The study showed that a compound teleophthalmology program in a semiurban community would be more effective but more costly than in-person examination. The findings raise the question of whether the benefits of pharmacy-based teleophthalmology in semiurban areas, where in-person examination is still available, are equivalent to those observed in remote communities. Further study is needed to investigate the impact of this program on the prevention of severe vision loss and quality of life in a semiurban setting.
Diabetic retinopathy is a sight-threatening complication in patients with diabetes mellitus that is usually asymptomatic in the early stages.1 Effective treatment exists, with over 50% of patients experiencing reduction of severe vision loss if they receive treatment after timely diagnosis.2
About 50% of patients with diabetes do not receive eye examinations as recommended by the American Academy of Ophthalmology.3 This results in lost opportunities to prevent severe vision loss by means of timely treatment delivery.4 In addition to nonmodifiable factors, limited availability of eye care specialists, travelling difficulties and time constraints also contribute to nonadherence, especially in nonurban areas.5,6
Pharmacy-based teleophthalmology has emerged as a possible alternative to in-person examinations that may facilitate compliance with evidence-based recommendations and reduce barriers to specialized eye care.7,8 In a pharmacy-based teleophthalmology program, retinal digital images are captured in a local pharmacy and are securely transmitted electronically to a specialized reading centre, where photographs are graded by an eye specialist.9 Patients with signs of diabetic retinopathy can then be referred to an eye care professional for comprehensive assessment.10 Thus, the workload of routine eye examination is transferred to other (presumably less expensive) settings, optimizing the use of specialized eye care services. In addition, this approach eliminates unnecessary travelling for patients and eye care professionals, and it may improve the consistency of community-based eye care delivery without geographic constraints.11
The cost-effectiveness of new technologies should be explored before implementation in specific settings to facilitate estimation of the eventual costs as well as the potential benefits compared with alternative strategies.12 The objective of this study was to estimate the cost-effectiveness of mobile teleophthalmology screening compared with in-person examination (primary care) for the diabetic population residing in semiurban areas of southwestern Ontario. Because such areas have limited specialized eye care and diabetic care, a pharmacy-based teleophthalmology program may be of benefit.13 Our primary interest was to assess the additional cost per case, from the health care system perspective, of any cases of diabetic retinopathy detected annually with pharmacy-based teleophthalmology. Unlike previous investigators,14-17 we considered a more realistic scenario in which the teleophthalmology program would not entirely replace in-person examination and also accounted for the effects of performing examination with and without pupil dilation with this technology. We studied both type 1 and type 2 diabetes, using weighted averages between groups when appropriate.
Methods
Study setting
The economic analysis was designed for the southwestern Ontario context, specifically semiurban areas of the Erie-St. Clair Local Health Integration Network. As of 2011, the census subdivision contemplated in this study (Chatham-Kent) reported a total of 103 671 inhabitants (population density 14.2 people per square kilometre), of whom 10 354 were over 20 years old and had type 1 or type 2 diabetes.18 We did not chose an explicitly urban model (e.g., Toronto) based on the assumption that in-person examinations would be relatively easy to access in such a setting. An explicitly rural model (e.g., Canada's far north) was not chosen because teleophthalmology may be the only alternative in such locations. There is true equipoise in understanding the cost-effectiveness of a teleophthalmology program in a semiurban context such as the Erie-St. Clair or equivalent Local Health Integration Network.
Decision-tree model
We constructed a decision tree using TreeAge Pro Suite 2013 to compare primary care examination (comparator program) versus pharmacy-based teleophthalmology (intervention program) (Appendix 1, available at www.cmajopen.ca/content/4/1/E95/suppl/DC1). In the analytical framework, we assumed that the pharmacy-based teleophthalmology program coexisted along with the reference program, increasing the volume of diabetic retinopathy examinations, but did not entirely replace in-person examination. This assumption aligns with the purpose of the teleophthalmology program to complement existing eye care services. To account for the coexistence of these 2 programs in the model we combined the screening rates of teleophthalmology and in-person examination into the teleophthalmology arm. Details of these calculations can be found in Appendix 2 (available at www.cmajopen.ca/content/4/1/E95/suppl/DC1).
Because we were interested in the potential ability of pharmacy-based teleophthalmology to strengthen screening coverage for diabetic retinopathy at a reasonable cost in the general population, our analysis was restricted to the correct detection of diabetic retinopathy cases (true-positive result), as opposed to incorporating treatment effects and disease progression into the model. The model was tailored for a mixed cohort of adults with type 1 or type 2 diabetes from the Chatham-Kent region, where 83% of residents are over 15 years old and 22.5% have diabetes. Hence, our target population consisted of 10 375 potential users. Although 3.7% of the area population is of Aboriginal ethnicity, we assumed these residents would not be reached by our program.19 Such a population would receive the most benefit from a teleophthalmology program culturally tailored to their communities and directed specifically to reserves, as opposed to a municipal pharmacy-based program.14 The outcome of interest was the detection of any diabetic retinopathy, manifested by at least 1 microaneurysm.3 We adopted a health care system perspective where consequences and direct costs pertaining to either program were included based on a 12-month time frame.
Interventions
Pharmacy-based teleophthalmology program
A general teleophthalmology program for diabetic retinopathy screening has 4 components: image acquisition, image review and evaluation, patient care supervision, and image and data storage.20 At minimum, it requires a specialized digital retinal camera, secure image storage and transmission software, and a specialized centre with the capacity of receiving and evaluating the digital images.7 Personnel can assume several roles, including image acquisition technician, image evaluation specialist, general program coordinator and medical care supervisor. The versatility of the system and camera portability facilitate its implementation in nonmedical settings, where it is more likely to reach unscreened people with diabetes.21 Pharmacies in particular are considered a strategic place to implement a teleophthalmology program, as people with diabetes visit pharmacies regularly to pick up medications.22
Once the person is informed about the procedure, retinal images are obtained with a digital retinal camera by a trained photography technician.23 The data are then securely transferred to a reading centre for assessment by an eye specialist or a certified reader. The entire process is supervised by a teleophthalmology coordinator.9 The findings are reported to the primary care physician with the recommendation for referral.24 Unreadable images are considered positive findings, and these patients must be referred for a comprehensive evaluation.25
Our economic model was designed for the evaluation of a pharmacy-based teleophthalmology screening program, used to identify patients with no (or minimal) diabetic retinopathy and those with more than minimal diabetic retinopathy.26 In this economic model, we considered the introduction of a part-time mobile retinal unit, operating 1 week per month on a rotational basis among regional pharmacies. We included 5 municipalities: Chatham, Wallaceburg, Blenheim, Tilbury and Ridgetown. The unit would be moved across these municipalities according to the manufacturer's specifications via a rented van (Appendix 3, available at www.cmajopen.ca/content/4/1/E95/suppl/DC1). The patient's clinical history would be noted by the program coordinator, and 45° digital photographs of both eyes would be obtained by an ophthalmic photographer; pharmacologic pupil dilation with tropicamide or phenylephrine, administered by the program coordinator, would be optional. Readable digital images would be sent electronically to the reading centre for assessment by a retina specialist. Patients with positive findings would be referred to a retina specialist for diagnostic confirmation with angiography and optical coherence tomography, which are considered the dual gold standard for diabetic retinopathy diagnosis.27 Similarly, patients with unclear fundus photographs would be referred for in-person examination by a retina specialist.25
In-person examination (primary care)
The primary care screening was defined as a fundus examination with pupil dilation performed by a primary care eye specialist (optometrist or ophthalmologist). Patients with positive results would be referred to a retina specialist for a comprehensive eye examination with angiography and optical coherence tomography.
Identification and calculation of model probabilities
Probabilities used in the base-case model are shown in Table 1. We calculated the prevalence of any diabetic retinopathy (22.5%) using public reports from the Public Health Agency of Canada and the National Coalition for Vision Health.29,30 The screening rate with the reference program (P(ref)) was considered to mirror the eye examination rate after diagnosis of diabetes in Ontario (51.1%).28 After the introduction of the new screening intervention, the patient could choose between 2 screening alternatives - in-person examination or teleophthalmology - or no screening. To include these preferences, we used a formula that incorporates the overall screening rate in the teleophthalmology arm as a compound of both in-person and teleophthalmology examination rates, according to patient preference (Appendix 2).
We obtained estimates of the diagnostic performance of teleophthalmology (e.g., sensitivity and specificity) from a recent meta-analysis32 that reported separately the summary results according to diagnostic threshold. We also used these data to estimate the proportion of unreadable images with teleophthalmology with and without pupil dilation. We obtained the proportion of examinations with pupil dilation from a study that used pharmacy-based teleophthalmology for diabetic retinopathy screening across Canadian provinces.33 We assumed that pupil dilation with tropicamide or phenylephrine would be performed by the program coordinator at the patient's discretion.
Calculation of model costs
Data sources for estimates of costs included published literature, market prices, vendor's quotations, official government reports and administrative information from St. Joseph's Healthcare, London, Ont. Only direct costs were incorporated into the model and are presented in 2013 Canadian dollars. Cost information is provided in Table 2. We obtained costs related to equipment and maintenance directly from the vendor, assuming a 5-year lifespan. Capital costs were annualized at a 5% discount rate per year, corresponding to the rate for 2014 Ontario government bonds. We obtained fuel costs from the Ontario Ministry of Energy website.35 Costs of recruitment through local diabetic associations and pharmacists were assumed to be equivalent to the cost of reaching patients with diabetes for in-person examination. We calculated pharmacy overhead costs from the annual Pharmacy Trends reports,36 which provide information on annual operating expenses per square foot among Canadian pharmacies.
To calculate labour costs, we conducted a literature search of economic studies on diabetic retinopathy screening that reported information on average minutes of labour cost per patient for obtaining and/or assessing eye photographs, which varied between 5 and 15 minutes.15 In-person consultation fees for major eye examination were obtained from the Ontario Ministry of Health and Long-Term Care Schedule of Benefits of Physician Services.37 The ophthalmic reader fee was based on the teleconsultation fee provided by the Alberta Healthcare Insurance Plan for pediatrics and related subspecialties (code 03.05JJ).38 We assumed that an Ontario teleconsultation fee for diabetic retinopathy assessment would resemble that of Alberta for teleconsultation in pediatric specialties.
Cost-effectiveness evaluation
We analyzed 2 measures of cost-effectiveness: cases of any diabetic retinopathy detected (true-positive result) and cases correctly diagnosed (including true-positive and true-negative results). We defined a case of diabetic retinopathy as any disease beyond very mild nonproliferative diabetic retinopathy, corresponding to a modified Airlie House classification grade of ≥ 20.26 We calculated cost-effectiveness as total cost divided by number of cases detected (or number of cases correctly diagnosed). Thus, the incremental cost-effectiveness ratio (ICER) was calculated as the extra cost needed to identify an additional case of diabetic retinopathy or an additional case correctly diagnosed after the implementation of pharmacy-based teleophthalmology.
Deterministic sensitivity analysis
Variables considered as potential drivers of the model were included in sensitivity analysis and were assigned plausible ranges based on 95% confidence intervals or upper and lower 25% limits around the base-case value. For simplicity, we limited the reporting of sensitivity analyses to the cost per case detected per year.
We conducted one-way sensitivity analyses for most variables. Those considered for one-way sensitivity analysis are listed in Table 1 (model probabilities) and Table 3 (model costs). We conducted a two-way sensitivity analysis to estimate the joint influence of screening volume and patient preference on the cost-effectiveness of pharmacy-based teleophthalmology. We also performed a multiway sensitivity analysis, in which model variables were varied simultaneously to generate extreme scenarios.
Results
Base-case analysis
Considering a population of 10 354 patients with diabetes with a compliance rate of 56.2%, the teleophthalmology program would correctly detect an additional 136 cases, and an additional 688 cases would be correctly diagnosed, compared with in-person examination only (Table 4). The cost per case detected was $510.00 with in-person examination and $478.30 with teleophthalmology, and the cost per case correctly diagnosed was $107.00 and $102.00 respectively. The ICER was $314.10 per additional case detected and $73.24 per additional case correctly diagnosed (Table 5). In both instances the programs were nondominant; hence, teleophthalmology was always more costly but was more effective than in-person examination alone (Figure 1).
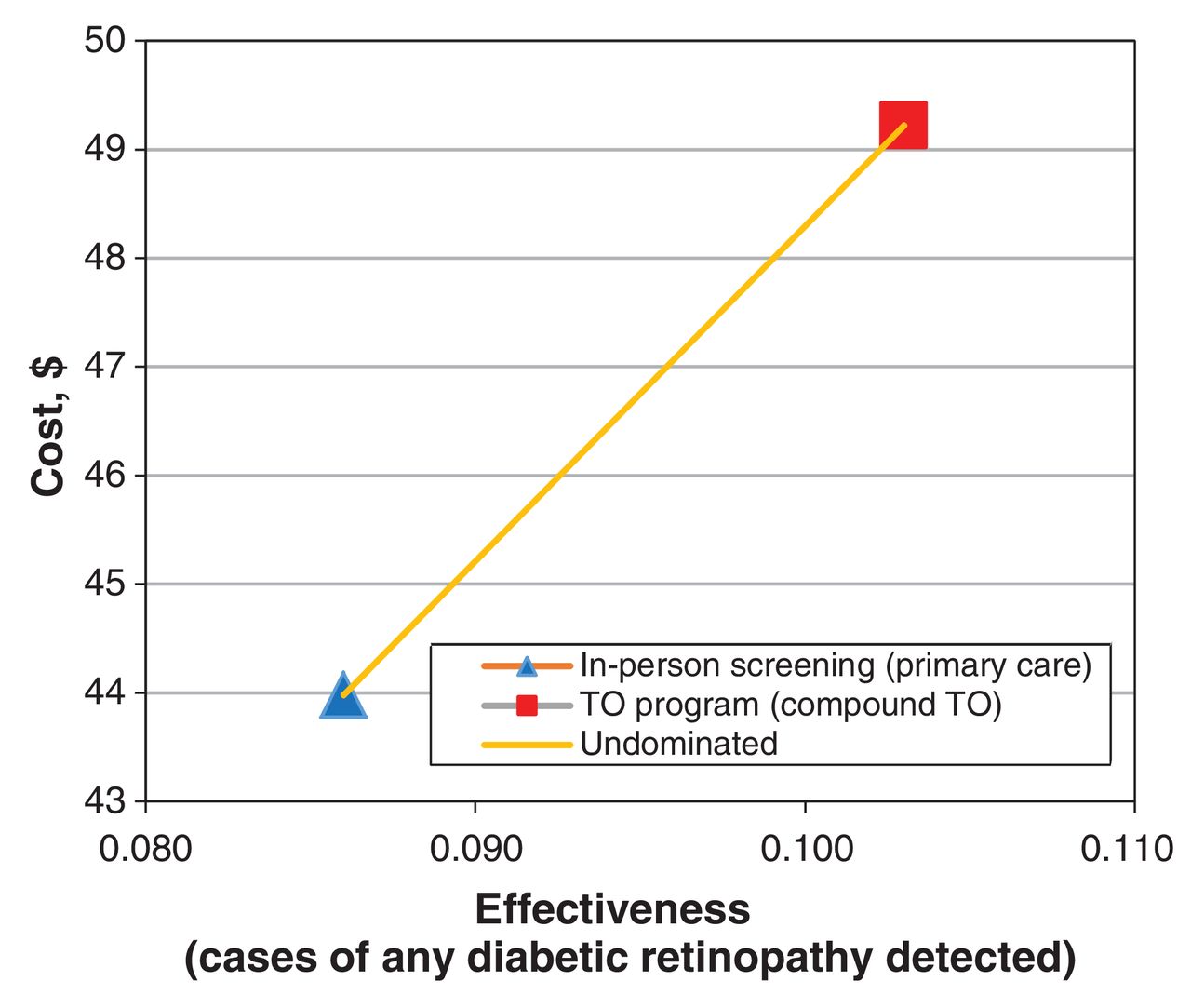
Cost-effectiveness plane. In-person examination versus introduction of pharmacy-based teleophthalmology (TO).
Sensitivity analyses
The model was stable with regard to sensitivity, specificity and prevalence variations (Table 6). Health care specialists' fees played a significant role in the cost-effectiveness of both screening programs. Other influential variables in the teleophthalmology program included the proportion of unreadable images (without pupil dilation) and the grader fee: telescreening examinations without pupil dilation showed a higher rate of unreadable images than screening with pupil dilation, which affected the incremental cost-effectiveness of the program.
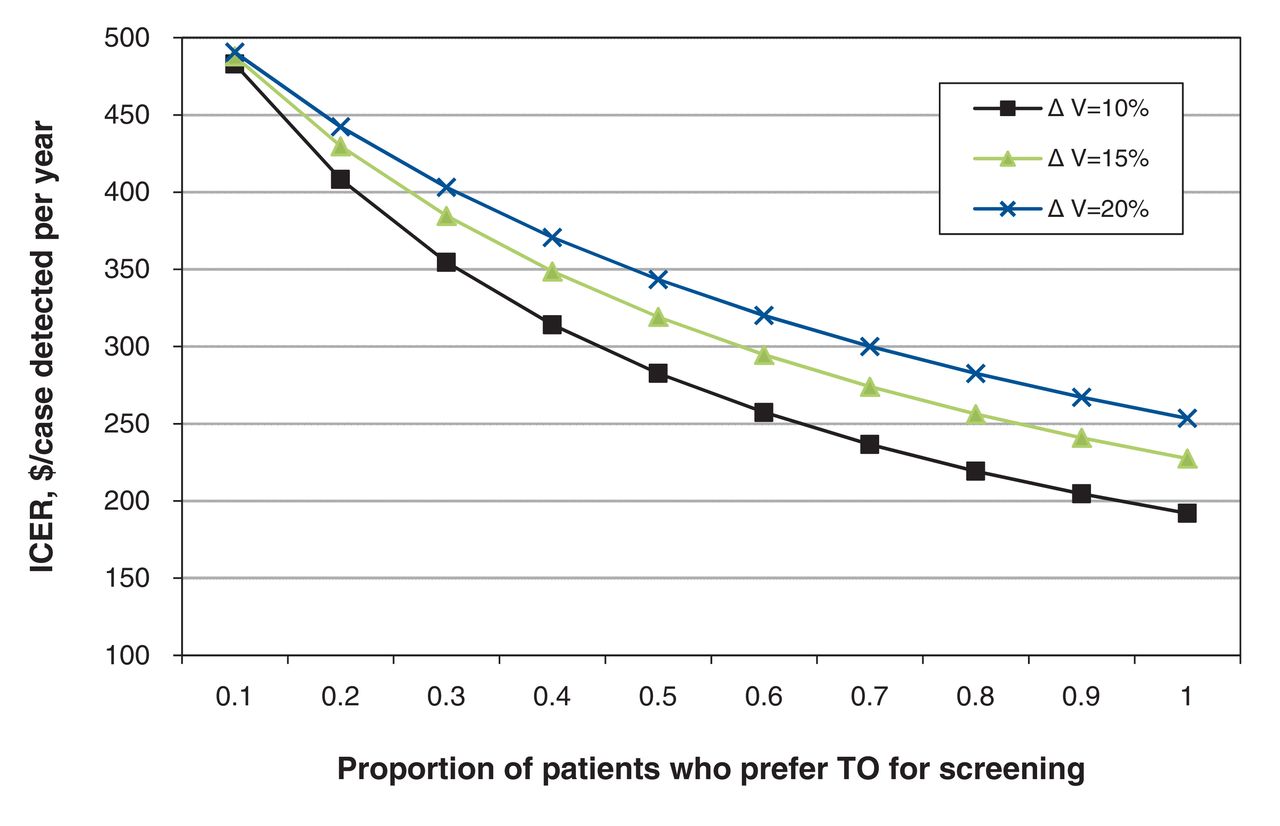
On two-way sensitivity analysis, teleophthalmology remained nondominant in all combinations of screening volume and patient preference (Figure 2). The lowest ICER was achieved when all patients preferred teleophthalmology ($192 per additional case detected per year).

Two-way sensitivity analysis. Influence of patient preference for pharmacy-based teleophthalmology (TO) and increased patient compliance after introduction of TO on the incremental cost-effectiveness ratio (ICER). ∆ V = volume increase of screened patients after introduction of TO.
On multiway analysis, in the best-case scenario, teleophthalmology dominated, at $367.60 per case detected per year, being less costly and more effective than in-person examination ($575.10 per case detected per year). In the worst-case scenario, teleophthalmology remained undominated, although the ICER was 4 times higher ($1393 per additional case detected per year) than the base-case value.
Interpretation
The detection of diabetic retinopathy by means of teleophthalmology has proven to be a cost-effective alternative in isolated communities, generating savings through lower transportation and personnel costs.5,6 In our study, in the Chatham-Kent context, a teleophthalmology program would be more effective than in-person examination, detecting 15% more cases of any diabetic retinopathy at $314.10 per additional case. However, it would also be more expensive.
Sensitivity analyses showed an important influence of health care specialists' fees for in-person examination and interpretation of retinal images. As expected, the ICER increased as the fee of retinal image readers increased up to 15% of its base-case value. When the in-person examination cost reached $78 per patient, teleophthalmology become less costly and more effective, dominating over in-person examination.
James and colleagues39 assessed the cost-effectiveness of systematic photographic screening versus opportunistic eye examination in the United Kingdom. Adjusted to 2013 Canadian dollars, the incremental cost per additional case of diabetic retinopathy detected was $83, which the authors regarded as cost-effective. In comparison, the ICER of teleophthalmology in our study of $314 may be too high to consider its implementation in a semiurban context. However, if an exclusive use of teleophthalmology is assumed, the ICER would be reduced to $192 per case detected, almost half of the base-case value and closer to the acceptable cost-effectiveness estimate reported by James and colleagues.39 Other investigators have reported teleophthalmology to be highly cost-effective or even dominant at the base-case analysis.16,17 However, comparisons of our results with those of prior studies are not straightforward owing to differences in effectiveness outcomes, model assumptions and especially geographic settings.
Limitations
Telescreening examinations without pupil dilation showed a higher rate of unreadable images than screening with pupil dilation, which affected the incremental cost-effectiveness of the program. Although pupil dilation may improve image quality and lower costs, it may prevent patients from accepting eye screening at the pharmacy.40
Our analysis did not look at the "downstream" analysis of diabetic retinopathy treatment (after screening) and results based on teleophthalmology versus usual care. Thus, our economic evaluation addressed only the cost per case detected, rather than the incremental cost per case of clinically relevant visual deterioration prevented, which remains to be determined.
Conclusion
The implementation of teleophthalmology would be more expensive in a semiurban community than in a context where the teleophthalmology program is assumed to be exclusive, as would be the case for isolated rural communities. If stakeholders are interested in investing in a teleophthalmology program in a semiurban context, a comprehensive discussion about potential strategies to reduce screening costs would be in order.
Our findings raise the question of whether the benefits of pharmacy-based teleophthalmology in semiurban areas, where in-person examination is still available, are equivalent to those observed in remote communities. Further study is needed to investigate the impact of this program on the prevention of severe vision loss and quality of life in a semiurban setting.
In summary, our findings show that a compound teleophthalmology program in a semiurban community would be more effective but more costly than in-person examination. Use of pharmacologic dilation and health care specialists' fees were the most important cost drivers and should be carefully considered during program design.
Supplemental information
For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/4/1/E95/suppl/DC1
Footnotes
Competing interests: None declared.
Contributors: Andrea Coronado and William Hodge contributed to the concept and design of the study. Andrea Coronado acquired and analyzed the data, and Andrea Coronado and William Hodge were involved in the interpretation of the data. Andrea Coronado drafted the article, and Gregory Zaric, Janet Martin, Monali Malvankar-Mehta, Francie Si and William Hodge critically revised the manuscript for intellectual content. All of the authors gave final approval of the version to be published and agreed to act as guarantors of the work.
Funding: This work was funded by a grant from the Academic Medical Organization of Southwestern Ontario Innovation Fund (grant no. INN12-010) and an Ontario Graduate Scholarship awarded to Andrea Coronado.
References
- Copyright 2016, 8872147 Canada Inc.
In this issue

{kind=link}
{kind=link}
Article tools





