


Article Figures & Tables
Figures
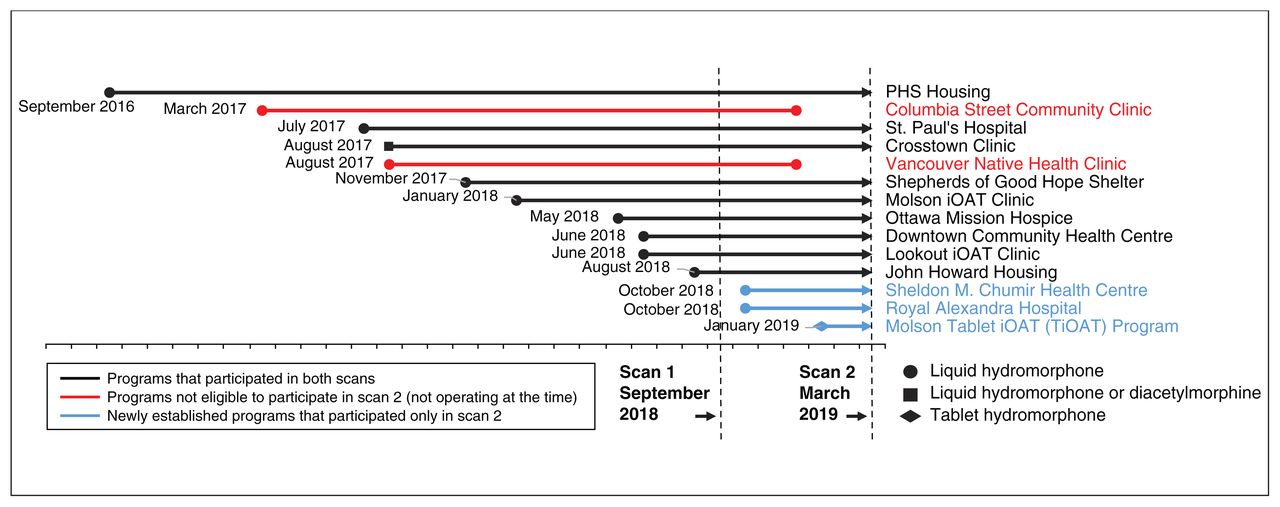
- Figure 1:
Timeline of injectable opioid agonist treatment (iOAT) program start and end dates (where applicable).
Tables
- Table 1:
Summary of service delivery models for injectable opioid agonist treatment by organization
Organization* Program City Province† Start date Service delivery model‡ PHS Community Services Society A: PHS Housing§ Vancouver BC Sept. 2016 Embedded and integrated; supported housing B: Columbia Street Community Clinic Vancouver BC Mar. 2017 Pharmacy based C: Molson iOAT Clinic Vancouver BC Jan. 2018 Embedded and integrated; overdose prevention site — separate entrance and injection space D: Molson Tablet iOAT Program Vancouver BC Jan. 2019 Embedded and integrated; overdose prevention site — shared entrance and injection space Providence Health Care E: St. Paul’s Hospital Vancouver BC July 2017¶ Hospital based; inpatient within ward setting F: Crosstown Clinic** Vancouver BC Aug. 2017 Comprehensive and dedicated; standalone clinic Vancouver Native Health Society G: Vancouver Native Health Clinic Vancouver BC Aug. 2017 Pharmacy based Vancouver Coastal Health H: Downtown Community Health Centre Vancouver BC June 2018 Embedded and integrated; community health centre — shared entrance, separate injection space Fraser Health I: Lookout iOAT Clinic Surrey BC June 2018 Embedded and integrated; community health centre — separate entrance and injection space Ottawa Inner City Health J: Shepherds of Good Hope Shelter Ottawa ON Nov. 2017 Embedded and integrated; shelter K: Ottawa Mission Hospice Ottawa ON May 2018 Embedded and integrated; hospice L: John Howard Housing Ottawa ON Aug. 2018 Embedded and integrated; supported housing Alberta Health Services (N: in partnership with Inner City Health and Wellness) M: Sheldon M. Chumir Health Centre Calgary AB Oct. 2018 Comprehensive and dedicated; colocated with community health centre N: Royal Alexandra Hospital Edmonton AB Oct. 2018 Hospital based; inpatient (and outpatient temporarily until community clinic opens) via hospital supervised consumption site Note: AB = Alberta, BC = British Columbia, iOAT = injectable opioid agonist treatment, ON = Ontario, PHS = Portland Hotel Society.
↵* Regional health authorities and community not-for-profit organizations, commonly with an operational or funding partnership.
↵† Canadian provinces reporting iOAT programs as of Mar. 1, 2019, were BC, ON and AB.
↵‡ Based on diverse pharmacy partnerships for dispensing, including private and health authority facilities located onsite, in the community or in a hospital.
↵§ PHS operates 3 supported housing units in which iOAT has been offered as of Mar. 1, 2019; this housing program is implemented at all units by the same staff members.
↵¶ Start date represents initiation of formal prescribing within the hospital using preprinted orders; iOAT was prescribed earlier using other methods.
↵** Site of 2 iOAT clinical trials running between 2005 and 2014; start date refers to the date on which new clients (other than participants in the clinical trials) began receiving iOAT.
- Table 2:
Summary of clinical and operational characteristics of injectable opioid agonist treatment programs
Program Hours* Core onsite staff† iOAT‡ Capacity (no. of clients); scan No. of available daily doses; scan Dose access structure;§ scan Scan 1 (Sept. 2018) Scan 2 (Mar. 2019) Scan 1 (Sept. 2018) Scan 2 (Mar. 2019) Scan 1 (Sept. 2018) Scan 2 (Mar. 2019) A: PHS Housing 6–7 Nurses, mental health workers (depending on housing unit) HDM 6 6 2 2 Open Open B: Columbia Street Community Clinic 6.75¶ Nurses, peer support workers, pharmacists, pharmacist technicians HDM 65¶ – 2 – Open – C: Molson iOAT Clinic 7 Nurses, mental health workers, peer support workers HDM 30 60 2 2 Open Open D: Molson Tablet iOAT Program 9 Nurses, mental health workers, peer support workers tHDM – 60 – 5 – Open E: St. Paul’s Hospital 24 All inpatient service staff HDM No limit No limit ** ** ** ** F: Crosstown Clinic 13.5 Nurses, clinic assistants HDM
DAM130–145 130–145 3 3 Group Open G: Vancouver Native Health Clinic 6.75¶ Nurses, peer support workers, pharmacists, pharmacist technicians HDM 65¶ – 2 – Open – H: Downtown Community Health Centre 7 Nurses, physicians, nurse practitioners, community liaison workers, pharmacists, pharmacist technicians HDM 14 14 2 2 Open Open I: Lookout iOAT Clinic 10 Nurses, harm reduction workers, clinic coordinators HDM 50 50 2 2 Group Open J: Shepherds of Good Hope Shelter 24 Client care workers HDM 6 6 7 4–5 Open Open K: Ottawa Mission Hospice 24 Nurse coordinators HDM 8 8 7 4–5 Open Open L: John Howard Housing 24 Nurse coordinators HDM 21 21 7 4–5 Open Open M: Sheldon M. Chumir Health Centre 10.5 Nurses, peer support workers, clinic managers, office assistants HDM – 35 – 3 – Group N: Royal Alexandra Hospital 9 Nurses, physicians, peer support workers, addiction counsellors, office assistant HDM – 15 – 3 – Booking Note: DAM = diacetylmorphine, HDM = hydromorphone, iOAT = injectable opioid agonist treatment, tHDM = tablet hydromorphone.
↵* The approximate amount of time the program was available for clients per day (may include closure for staff breaks or handover sessions).
↵† Staff available during all opening hours and providing the foundation for day-to-day operations. Other staff (e.g., physician, psychiatrist, dietitian) were available at varying times.
↵‡ Available iOAT medications: liquid HDM, liquid DAM (medical heroin) and tHDM.
↵§ Several dose access structures were in use: open = clients attended any time, group = clients were allocated to a treatment group with specified times, booking = clients received individual appointments.
↵¶ The Columbia Street Community Clinic and the Vancouver Native Health Clinic shared a single community pharmacy partner for maintenance doses; these data represent the pharmacy characteristics only.
↵** As clinically indicated during acute care admission; iOAT dose administered directly by nursing staff.
- Table 3:
Summary of clients’ characteristics by injectable opioid agonist treatment program, with national-level tallies
Program Total no. of client starts; scan No. of active clients;* scan No. on wait list; scan Age, yr, mean (range) No. of clients; scan; gender Scan 1 (Sept. 2018) Scan 2 (Mar. 2019) Scan 1 (Sept. 2018) Scan 2 (Mar. 2019) Scan 1 (Sept. 2018) Scan 2 (Mar. 2019) Scan 1 (Sept. 2018) Scan 2 (Mar. 2019) Scan 1 (Sept. 2018) Scan 2 (Mar. 2019) F M T† F M T† A–D: All PHS programs‡§ 286 312 67 119 0 112 ‡ ‡ ‡ ‡ ‡ ‡ ‡ ‡ tHDM – 60 E: St. Paul’s Hospital‡ ‡ ‡ 8 8 0 0 ‡ ‡ 2 6 0 2 6 0 F: Crosstown Clinic 259 291 126 125 345 400 44 (21–69) 44 (21–69) 31 94 1 39 85 1 DAM 106 107 G: Vancouver Native Health Clinic 10 – 1 – 0 – 53 (53) – 0 1 0 – – – H: Downtown Community Health Centre 7 18 4 11 0 0 51 (36–68) 48 (36–68) 1 3 0 4 7 0 I: Lookout iOAT Clinic 37 77 22 18 0 0 45 (30–61) 44 (27–62) 4 18 0 4 14 0 J–L: All Ottawa Inner City Health programs‡ 26 29 22 22 ≥ 55 ≥ 75 40 (25–57) 43 (25–57) 11 11 0 12 10 0 M: Sheldon M. Chumir Health Centre – 45 – 22 – 0 – 35 (22–48) – – – 4 18 0 N: Royal Alexandra Hospital – 9 – 6 – 0 – 44 (29–64) – – – 3 3 0 National-level tallies 625 781 250 331 ≥ 400 ≥ 587 47 (21–69) 43 (21–69) 49 133 1 68 143 1 Note: DAM = diacetylmorphine, F= female, iOAT = injectable opioid agonist treatment, M = male, T = transgender or nonbinary, tHDM = tablet hydromorphone.
↵* Clients receiving at least 1 dose of iOAT in the 7 days before the scan reference date. All numbers represent clients receiving liquid hydromorphone except where programs provided DAM or tHDM (tablet iOAT) in addition to liquid hydromorphone; in these cases, the number of active clients receiving DAM and tHDM is reported underneath the total number of active clients, to indicate the size of these specific client groups.
↵† There was variable reporting for this gender category across sites.
↵‡ Data not available or data stratified by program not available where more than 1 program was operated by a single organization.
↵§ Age and gender data available only at follow-up for the 312 client starts: mean age 41 (20–73) yr, 230 men (74%), 77 women (25%), 5 transgender or nonbinary people (2%).
- Table 4:
Frequency with which barriers and facilitators of injectable opioid agonist programs for ongoing service delivery were reported
Barriers No. (%) of programs Facilitators No. (%) of programs Limited program capacity 7 (50) Client-centred care (e.g., responsive to client goals and needs) 13 (93) Pharmacy operations (e.g., dispensing delays, inadequate missed dose or dose adjustment protocols, lack of community pharmacy partner options for maintenance doses or syringe preparation) 6 (43) Relationships with clients (e.g., rapport, trust, sense of community, client involvement in care plan) 10 (71) Lack of diacetylmorphine access (i.e., medical heroin) 5 (36) Access to ancillary services (e.g., other health and social services to provide wraparound care) 7 (50) Strength of available medication too low (e.g., only 10 mg/mL in Ontario) 5 (36) Strong relationship with community partners (e.g., overdose outreach team, other health services such as primary care, community iOAT service providers) 7 (50) Physical space restrictions 5 (36) Low-barrier access (e.g., service in supported housing) 6 (43) Inadequate staff coverage or capacity 4 (29) Harm reduction approach 5 (36) Issues associated with oral OAT provision (e.g., none onsite, lack of access to preferred medication) 4 (29) Rapid and simple process for new starts (e.g., same day) 5 (36) Issues associated with management of stimulant use (e.g., ongoing concurrent use, presence of fentanyl and carfentanil in stimulants) 4 (29) Peer workers to support engagement and clinical flow 5 (36) Inadequate ancillary services and facilities (e.g., lack of community housing and counselling support) 4 (29) Active client follow-up to support engagement 4 (29) Challenges with continuity of care (e.g., from community to jail, prison or acute care; from acute care to community) 4 (29) Pharmacy relationship (e.g., onsite pharmacy, strong partnership with community pharmacy dispensing iOAT) 4 (29) Treatment induction issues (e.g., lag time between eligibility approval and first dose, inadequate titration protocols, prolonged wait times for split doses) 3 (21) Housing First approach (e.g., shelter into housing) 2 (14) Limited opening hours 3 (21) Well-trained and knowledgeable nursing staff 2 (14) Issues associated with group allocation as dose access structure (e.g., access barrier for clients, management challenges for staff) 3 (21) Multiple physician prescribers to provide adequate cover for assessments, dose adjustments and oral OAT 1 Inadequate client records or tracking (e.g., paper-based records, lack of monitoring and active follow-up to support engagement) 2 (14) Access to diacetylmorphine (i.e., medical heroin) 1 Challenges associated with engaging clients (e.g., clinical adherence, following rules and responsibilities of service) 2 (14) Regular communication within a multidisciplinary team 1 Lack of programming for specific groups: females, youth, Indigenous people (e.g., female-only sessions) 1 Onsite provision of all medications prescribed to client 1 Lack of access to brand-name medications (i.e., access to generic hydromorphone only) 1 Establishment of a provincial reference number for hydromorphone dispensing within electronic system 1 Note: Barriers and facilitators are reported only once when: a) reported in baseline and follow-up; b) barriers/facilitators fall within the same theme for the same program.
Participants reported barriers and facilitators in response to open-ended questions. iOAT = injectable opioid agonist treatment, OAT = opioid agonist treatment.
In this issue

{kind=link}
Article tools





