


Abstract
Background: A growing number of migrants experience precarious housing situations worldwide, but little is known about their health and housing experiences. The objective of this study was to understand the enablers and barriers of accessing fundamental health and social services for migrants in precarious housing situations.
Methods: We conducted a systematic review of qualitative studies. We searched the databases of MEDLINE, PsycINFO, CINAHL, Scopus, Web of Science, Social Sciences, Canadian Business & Current Affairs and Sociological Abstracts for articles published between Jan. 1, 2007, and Feb. 9, 2020. We selected studies and extracted data in duplicate, and used a framework synthesis approach, the Bierman model for migration, to guide our analysis of the experiences of migrant populations experiencing homelessness or vulnerable housing in high-income countries. We critically appraised the quality of included studies using the Critical Appraisal Skills Programme checklist and assessed confidence in key findings using the Grading of Recommendations Assessment, Development and Evaluation Confidence in the Evidence from Reviews of Qualitative Research (GRADE-CERQual) approach.
Results: We identified 1039 articles, and 18 met our inclusion criteria. The studies focused on migrants from Asia and Africa who resettled in Canada, Australia, the United States, the United Kingdom and other European countries. Poor access to housing services was related to unsafe housing, facing a family separation, insufficient income assistance, immigration status, limited employment opportunities and lack of language skills. Enablers to accessing appropriate housing services included finding an advocate and adopting survival and coping strategies.
Interpretation: Migrants experiencing homelessness and vulnerable housing often struggle to access health and social services; migrants may have limited proficiency with the local language, limited access to safe housing and income support, and ongoing family insecurities. Public health leaders could develop outreach programs that address access and discrimination barriers.
PROSPERO Registration: CRD42018071568
Worldwide, more than 272 million people are classified as “international migrants”.1 Migrant populations include refugees, asylum seekers, displaced persons and immigrants who move from their country of residence to another.2,3 Literature suggests that homelessness may be prevalent among migrants to different countries.4–6 Within North America, evidence highlights a substantial movement of undocumented migrants from the United States into Canada.7
Refugees and other migrants who are precariously housed may couch surf, or live in motels and other short-term rentals. When these options fail, they turn to temporary homeless shelters.8,9 In contrast to government-assisted refugee shelters, homeless shelters lack language and cultural food resources, and other health, education and employment resettlement infrastructure.8 Forced displacement and marginalization can create additional challenges in securing safe and stable housing for migrants,10 with many experiencing homelessness at some point in their resettlement process. The magnitude of visible or hidden migrant homelessness is largely unknown and what little evidence exists is of low quality, which limits the development of policies, programs and services that address homelessness among migrants.
Field research suggests that the risk of migrant homelessness increases with cuts to social programs, persistent health issues, poverty, lack of affordable housing, unrecognized education credentials, unemployment, delays in obtaining work permits, deinstitutionalization and lack of discharge planning.11 Mobile migrants are also at risk for frostbite, infectious diseases, soft-tissue infections, traumatic injuries and chronic illnesses (e.g., diabetes, cardiovascular disease).12,13 Furthermore, migrants may suffer from common mental illnesses, including posttraumatic stress disorder and depression.14 Migrant populations may also struggle with food insecurity and impaired access to health and social services.15–17
The objective of this systematic review was to understand the enablers and barriers of accessing fundamental health and social services for migrants who found themselves in precarious housing situations.
Methods
Study design
We conducted a systematic review according to a registered protocol (PROSPERO CRD42018071568; Appendix 1, available at www.cmajopen.ca/content/9/2/E681/suppl/DC1).19 We reported our findings according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guideline.20
Search strategy
With the assistance of an information scientist librarian, we developed a search strategy using a combination of subject headings and keywords, including “migrant,” “refugee,” “asylum seeker,” “homeless,” “unsheltered” and “street.” The primary search strategy is presented in Appendix 2, available at www.cmajopen.ca/content/9/2/E681/suppl/DC1. We used this strategy, and its translated versions, to systematically search the databases of MEDLINE, PsycINFO, CINAHL, Scopus, Web of Science, Social Sciences, Canadian Business & Current Affairs and Sociological Abstracts for relevant studies from 2007 to Feb. 9, 2020. We did not apply any filters or language restrictions. We did not systematically search for additional studies in reference lists or grey literature.
We originally searched bibliographical databases from the date of their inception; however, we soon recognized that evidence published since 2007 represents a reflection of a scholarly evolution in the field of migration and global health research, characterized by an exponential increase in the rate of research articles published in peer-reviewed journals.18 As a result, we decided to deviate from protocol and restrict the date of publication from 2007 onward at the full-text screening phase of the review.
Eligibility criteria
We included studies in our systematic review if they used a qualitative or mixed method design and were published between 2007 and 2020, in any language. We focused on studies whose participants were refugees, asylum seekers or undocumented migrants who were presently residing in high-income countries, as defined by the World Bank.21 We restricted our studies to high-income settings, given the relative homogeneity in how migrants integrate into the labour market22 and the similar challenges they face when accessing health and social welfare services.23,24 We included studies that reported on the barriers and facilitators that migrants face when accessing housing or shelter, and their health and well-being. Full inclusion and exclusion criteria, and a detailed description of study populations, interventions, controls and outcomes can be found in Appendix 3, available at www.cmajopen.ca/content/9/2/E681/suppl/DC1.
Study selection and data collection
Four team members (H.K., C.M., A.S., Q.A.) screened and selected titles, abstracts and full-text articles, independently and in duplicate. At the full-text screening stage, we limited articles to those published between Jan. 1, 2007, and Feb. 9, 2020, as noted earlier. All conflicts were resolved through discussion or by consulting a third reviewer (K.P.).
After study selection, we developed a standardized data extraction sheet that included study methodology, participant characteristics and contextual findings, including labour market conditions, immigration policies, social networks, neighbourhood characteristics, discrimination, income, education and language. We piloted the data extraction form to ensure relevancy (H.K., G.K.). Five reviewers (H.K., G.K., O.M., A.S., Q.A.) extracted data independently and in duplicate, and any conflicts were resolved with the help of a third reviewer (K.P.).
Data analysis
We assessed the methodological quality of included articles using the Critical Appraisal Skills Programme checklist for qualitative studies25 (H.K., G.M., O.M., A.S.) (Appendix 4, available at www.cmajopen.ca/content/9/2/E681/suppl/DC1). We used the best-fit framework method as a systematic and flexible approach to analyzing the qualitative data.26–28 Framework analysis is a 5-stage process that includes familiarization with the data, identifying a thematic framework, indexing (applying the framework), charting and mapping, and interpretation.29 We selected the Bierman model for migrant health as our framework.30 The Bierman model is a conceptual framework that considers the intersection of social determinants of health, gender equity, racial and ethnic disparities in health, and the migration experience.31
One reviewer (H.K.) coded the data into the domains of the Bierman model using a matrix spreadsheet to facilitate analysis; a second reviewer (K.P.) verified the coding. The review team (H.K., O.M., A.S., K.P.) identified and interpreted key findings through discussion with the review team. For the purposes of this review, we defined a review finding as an analytic output from our qualitative evidence synthesis that describes a phenomenon or an aspect of a phenomenon, based on data (participant quotations or author observation) from primary studies.32
We used the Grading of Recommendations Assessment, Development and Evaluation Confidence in the Evidence from Reviews of Qualitative Research (GRADE-CERQual) approach.33,34 This approach evaluates findings on 4 criteria: methodological limitations of included studies supporting a review finding, the relevance of included studies to the review question, the coherence of the review finding and the adequacy of the data contributing to a review finding (Table 1).
Components of GRADE-CERQual assessments33
Ethics approval
Ethics approval was not required for this study.
Results
Our search initially identified 1039 unique articles; however, after the initial removal of duplicates, we found 754 additional duplicate citations. We further screened articles to exclude low-income countries, and study populations and designs that did not meet inclusion criteria. We included 18 studies in our analysis (Figure 1).
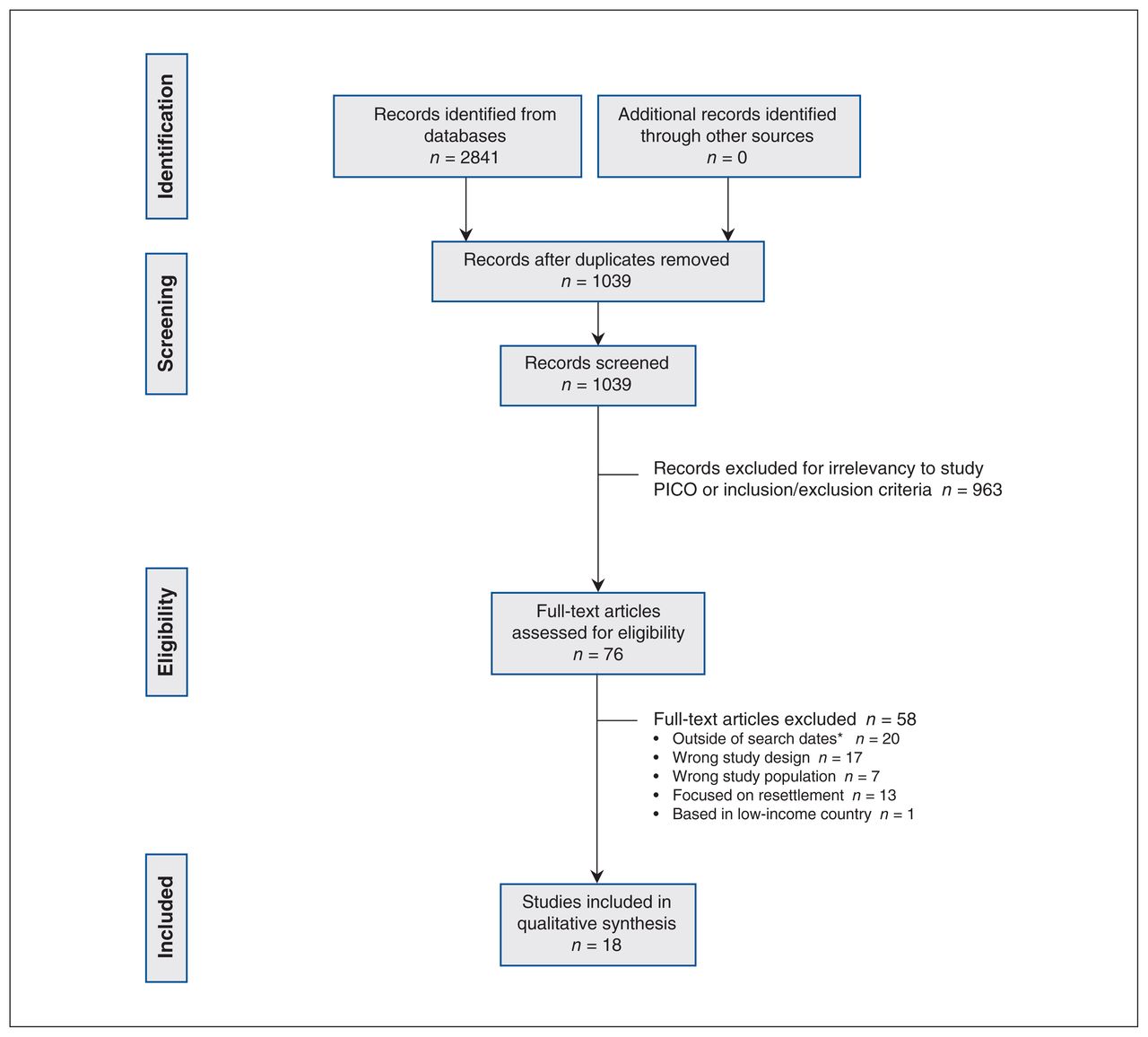
Flow chart based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines.
Note: PICO = population, intervention, comparison, outcomes. *We originally searched bibliographical databases from the date of their inception; however, we soon recognized that evidence published since 2007 represents scholarly evolution in the field of migration and global health research.18 As a result, we deviated from protocol and restricted date of publication from 2007 onward at the full-text screening phase of the review.
Study characteristics
Eight studies focused specifically on refugees,6,35–41 and the remaining 10 studies considered the broader migrant populations, including immigrants, newcomers or refugees.42–51 Resettlement countries included Canada (n = 9), Australia (n = 4), Belgium (n = 1), Denmark (n = 1), Norway (n = 1), the United Kingdom (n = 1) and the US (n = 1). All included studies followed a naturalistic inquiry approach, except for 3 that had a comparison group.45,48,49 The characteristics of included studies and the methodological quality of studies are found in Table 2.
Characteristics of included studies
The Bierman model (Appendix 5, available at www.cmajopen.ca/content/9/2/E681/suppl/DC1) provided conceptual categories that we used to map and characterize our qualitative findings. In doing so, we identified 8 distinct findings from the included studies, summarized in Table 3. The confidence in the findings ranged from very low to moderate, with 4 of the findings being of moderate confidence. Appendix 6, available at www.cmajopen.ca/content/9/2/E681/suppl/DC1, provides a detailed description of the findings. Of note, several factors from within the Bierman model had limited data available during the extraction process, including political environment, education and other factors.
Summary of findings
Barriers to accessing housing services
Interpersonal racism
Two common barriers to accessing stable and secure housing for migrants were discrimination and stigmatization, often based on race, gender, socioeconomic status, language of origin, housing situation, trauma history and number of children (GRADE-CERQual confidence level: low).6,39,46,47 For example, one migrant stated, “Every time I would call an advert[isement], I would call asking for a house and they would ask, ‘Oh, you have an accent. Where do you come from?’ When I told them I am from Africa, well, the apartment was taken.”47
Mental health concerns
The combined impact of the past trauma experienced by migrants and their vulnerable housing situations contributed to mental health concerns,6,36,39,40,50 often resulting in sleep problems, loss of appetite and anxiety (GRADE-CERQual confidence level: moderate).37 For example, 1 study reported a migrant feeling “seriously stressed” about his homeless status, affecting his mental health.6
Poor access to services
Refugees and other migrants are often unaware of support services and find them difficult to access and navigate (GRADE-CERQual confidence level: moderate).48,51 For example, one migrant in the UK stated, “We are going every time to social services. [Asking] Where is [private housing provider]? Where is Refugee Council? We didn’t know nothing.”38 Another stated, “It was just presumed that I knew where to go, that I understood the system.”40 Furthermore, migrants who were unfamiliar with services would not access emergency or transitional accommodation. Some migrants did not identify as homeless, and would not seek out services.40
Unsafe housing
Refugees and other migrants perceived the housing options available to them as unsafe, poorly managed and unaffordable. Furthermore, housing programs were often described as strict, controlling, substandard, and in some cases, dangerous, especially by younger populations (GRADE-CERQual confidence level: high).35,38–40,48 In one UK study, several of the respondents described the weaknesses in the National Asylum Support Services housing system as poor quality, overcrowded and lacking effective orientation and services.38
Facing family conflict and intercultural tensions
Several vulnerably housed refugees expressed difficulties learning a new culture, and parents also struggled with the ability of their children to balance a new culture and the culture of their country of origin (GRADE-CERQual confidence level: low).40 At times, parents considered their child’s acquisition of the English language, Western fashion or new social life as abandonment of their traditional cultural beliefs and values (GRADE-CERQual confidence level: low).39 The tension between 2 different cultures often resulted in conflicts and tensions in family support systems (GRADE-CERQual confidence level: low).39
Insufficient income assistance
Refugees and other migrants reported strained finances and inadequate financial support that led to difficulty meeting basic needs, housing insecurity and food instability (GRADE-CERQual confidence level: low).40,45–48 In one study, nearly all of the respondents had had trouble finding a new place to live because accommodation was too expensive.47
Impact of immigration status
Compared with status migrants, nonstatus migrants faced substantial barriers, such as limited rights to welfare, prohibition from taking up paid employment and rejection from shelter access (GRADE-CERQual confidence level: low).36,38,45,51 Ravnbøl and colleagues51 discussed how Danish law prevented migrants from registering as workers in the European Union, and because they did not have a Danish social security number, no one would hire them or rent them a place to live.
Lack of language skills impeding access
Limited language skills negatively affected accessibility to health and social services for migrants, such as housing programs (GRADE-CERQual confidence level: moderate).51 In a study by Couch and colleagues,39 a young migrant in a rooming house described the challenges of renting with limited English skills, “My English is a problem because I do not always understand the rules of renting a place and may get evicted because I do not understand the rules. Or sometimes notices are placed in the building for people to come together and I can’t be involved because I can’t read the sign.” Mostowska and colleagues considered language the most important resource for migrants to create and expand their social networks beyond their cultural community;43 limited language skills can worsen the feeling of being isolated from others (GRADE-CERQual confidence level: moderate).44
Limited employment opportunities
Difficulty obtaining employment was frequently reported among migrants as a barrier to stable and secure housing. Being denied work or meaningful opportunities can inhibit and affect migrants’ pride in being active citizens in their resettlement country, as well as affect their personal sense of accomplishment and meaning (GRADE-CERQual confidence level: moderate).37,39,47 Dreams of owning a house, studying or working as citizens of a new country were difficult to achieve: “I am so many steps away, miles away from having anything like the Australians have.”40 Some migrants noted limited personal, family and cultural resources that further exacerbated the ability to find stable and meaningful employment.
Enablers to accessing housing services
Finding an advocate
Refugees who sought a culturally familiar, community advocate were able to increase their social capital, which is recognized as the network of social relations that can provide people and groups with access to resources and support (GRADE-CERQual confidence level: high).39–41,47,48 Advocates included settlement counsellors and cultural brokers. These advocates were able to help refugees transition out of homelessness by providing social support, a place to stay and other resources.41,48 One study reported that when a pregnant woman was faced with impending homelessness, she scanned the public phone directory, looking for Sudanese names from her community.39 Similarly, another woman found assistance in housing after approaching a stranger on the street who spoke her first language.47
Adopting survival and coping strategies
Refugees and other migrants who faced insecure housing instability adopted survival and coping strategies that helped them to advocate for resources and develop a sense of belonging in their new community. The survival and coping strategies ranged from faith-based coping to coping using substance use (GRADE-CERQual confidence level: moderate).39–41,46,50
Interpretation
A comprehensive understanding of background characteristics that influence the health and well-being of patients is a prerequisite to delivering equitable health care.52,53 Two such characteristics that are hypothesized to increase vulnerability and decrease access to services are homelessness and migration status.4,54 We explored the best available qualitative evidence on the enablers and barriers of accessing fundamental health and social services for migrants who found themselves in precarious housing situations.
Our findings suggest that migrants experiencing homelessness often struggle to meet their housing and health needs and to access essential services because of interpersonal racism, limited proficiency with the local language, lack of financial stability and family tensions, leading to worsened mental health conditions. To overcome these barriers, migrants experiencing homelessness often resort to different coping strategies and rely on community advocates to increase their social capital. Even though implementing interpretation services can mitigate linguistic barriers and ensure the provision of equitable care for migrant patients,55,56 health care practitioners in Canada need to adopt a more holistic approach to providing care for these populations, one that addresses their housing situation and the barriers that further increase their housing instability and vulnerability, such as family tensions and financial instability.
Migrants described experiencing interpersonal racism when attempting to access health and social services. Xenophobia, racism, and attitudes and behaviours that lead to civic exclusion of others based on a foreign cultural or national identity are upstream factors that produce discrimination and poor health outcomes for migrants.57 Interpersonal incidents of racism are an attack on communities, rather than just individuals.58,59 Indeed, acts of racism are reflections of historical legacies of colonialism and domination,59 which reinforce disempowerment and structural violence. Structural violence describes the social structures that prevent individuals and entire populations from reaching their full potential.60 Structural violence continues to serve as a challenge to providing health care for marginalized populations,61,62 depriving patients of their right to receive equitable services, and increasing the social gradient of how beneficial such services tend to be.53 Even though discrimination has been found to sever trustworthy connections between the general homeless population and their health care providers,63 our findings suggest that this problem is further aggravated when patients who are homeless also have a migration history. In Canada, primary health care practitioners can effectively address their patients’ experiences of interpersonal racism by employing trauma-informed care in its core values and principles.64
Past trauma was found to worsen the mental health conditions of refugees and other migrants. The literature is abundant with evidence linking premigration and migration exposures of trauma and violence to the initiation or exacerbation of common mental health conditions, such as major depressive disorders, generalized anxiety and posttraumatic stress disorders.14,65 In Canada, the literature highlights a trend of limited access and uptake of mental health services by different migrant populations.66,67 With the scarcity of mental health screening initiatives,68 and the discontinuity of mental health care after resettlement,69 migrants find themselves in need of scaled-up mental health services that could be delivered in their communities.70
Moreover, homelessness after resettlement was a fundamental component that worsened many mental health conditions among migrants. This finding suggests that homelessness is not only the consequence of poor mental health, but also a predictor of poor mental health. Primary health care practitioners in Canada now have an evidence-based guideline to address homelessness as the root for many morbidities and to initiate care for patients experiencing homelessness, including migrants, using upstream and longitudinal interventions.71
It is important to develop and evaluate public health responses for migrants who are homeless or vulnerably housed, especially undocumented migrants. Advances in universal access to health services72 and social accountability in medical schools73 could be matched with policy changes to ensure health equity for homeless migrants. Public health could play a role in raising awareness of these priority populations and developing programs and policies that address access and discrimination barriers, such as antiracist housing policies, migrant-sensitive mental health supports in shelters and migrant-specific shelters. Indeed, public health research can deepen our understanding of the values, attitudes and perceptions of migrants regarding housing, and can have a role in improving outcomes of the social determinants of health.
We evaluated the enablers and barriers of accessing health and social services among a population with lived experience of homelessness. We followed systematic and transparent review methodology to ensure we identified the best available evidence on this phenomenon. As a result, we included studies of vulnerable migrants from diverse geographic regions around the world. Furthermore, we used the GRADE-CERQual methodology to rate the confidence in our findings.
Limitations
We did not use a Peer Review of Electronic Search Strategies (PRESS),74 which could have guided and improved the search strategy. We did not conduct a grey literature search, nor did we search any reference lists. A protocol deviation is also further detailed in Appendix 7, available at www.cmajopen.ca/content/9/2/E681/suppl/DC1. Furthermore, our findings are constrained to the data provided by the interviews and participants within the published primary studies. For example, most participants spoke English, and we recognize that language is an important additional barrier to resources.
Only a small number of participants were undocumented migrants, an important subgroup of this vulnerable population. More subgroup analyses, such as from youth or the recent Syrian refugees, would be important to better understand these specific populations in the future. Most included articles did not describe in detail the relationship between the researcher and the participant which, if not addressed appropriately, could introduce concerns of interviewer and social desirability biases and jeopardize the trustworthiness of qualitative evidence from primary studies. Lastly, we tried to ensure that our findings and considerations were applicable to the Canadian context, which required contextualization and judgments on the relevance of included studies conducted outside of Canada. This process, however, was not always feasible given reporting limitations on the primary-study level.
Conclusion
We highlighted the challenges that refugees and other migrants face after resettlement and when experiencing homelessness. Discrimination and xenophobia were recurrent themes described as both a cause and a consequence of unsafe and insecure housing. An important finding was the limited research available on undocumented migrants experiencing homelessness. Vulnerable housing was often linked to family separation, poor access to services and limited income and employment. Migrants may also face language, cultural and immigration status barriers, and they may benefit from field advocates and personal survival strategies. These findings warrant physician vigilance and public health responses.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Harneel Kaur and Kevin Pottie conceived and designed the work. All authors contributed to the acquisition, analysis and interpretation of data. Harneel Kaur, Ammar Saad, Olivia Magwood, Christine Mathew and Kevin Pottie drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Data sharing: The authors used publicly available data for the analysis in this study.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/9/2/E681/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2021 CMA Joule Inc. or its licensors
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- "Just a knife wound this week, nothing too painful": an ethnographic exploration of how homeless clients attending an urban primary care and addiction service view their own health and healthcare
- Soigner les refugies et les nouveaux arrivants a lere post-COVID-19: Revue des donnees probantes et conseils pour les MF et les professionnels de la sante
- Caring for refugees and newcomers in the post-COVID-19 era: Evidence review and guidance for FPs and health providers