


Abstract
Background: Medical education affects learner well-being. We explored the breadth and depth of interventions to improve the well-being of medical learners in Canada.
Methods: We searched MEDLINE, EMBASE, CINAHL and PsycINFO from inception to July 11, 2020, using the Arksey–O’Malley, 5-stage, scoping review method. We included interventions to improve well-being across 5 wellness domains (i.e., social, mental, physical, intellectual, occupational) for medical learners in Canada, grouped as undergraduate or graduate nonmedical (i.e., health sciences) students, undergraduate medical students or postgraduate medical students (i.e., residents). We categorized interventions as targeting the individual (learner), program (i.e., in which learners are enrolled) or system (i.e., higher education or health care) levels.
Results: Of 1753 studies identified, we included 65 interventions that aimed to improve well-being in 10 202 medical learners, published from 1972 through 2020; 52 (80%) were uncontrolled trials. The median year for intervention implementation was 2010 (range 1971–2018) and the median length was 3 months (range 1 h–48 mo). Most (n = 34, 52%) interventions were implemented with undergraduate medical students. Two interventions included only undergraduate, nonmedical students; none included graduate nonmedical students. Most studies (n = 51, 78%) targeted intellectual well-being, followed by occupational (n = 32, 49%) and social (n = 17, 26%) well-being. Among 19 interventions implemented for individuals, 14 (74%) were for medical students; of the 27 program-level interventions, 17 (63%) were for resident physicians. Most (n = 58, 89%) interventions reported positive well-being outcomes.
Interpretation: Many Canadian medical schools address intellectual, occupational and social well-being by targeting interventions at medical learners. Important emphasis on the mental and physical well-being of medical learners in Canada warrants further exploration.
Concerns exist about the impact of medical education on learner well-being.1–4 Programs housed within medical schools often address intellectual and occupational well-being, focusing specifically on skills related to learning and working;5,6 however, well-being is a multidimensional construct. Social, mental, and physical well-being have been shown to be negatively affected during undergraduate medical education,7 with increased prevalence of burnout in residency.8,9 Poor well-being can affect medical learners across the spectrum of programs, including undergraduate health sciences.10
The Canadian Federation of Medical Students aims to “train healthier physicians to maximize the productivity and quality of health care services for Canadians.”11 Their strategic directions for 2020–2022 include developing health promoting communities, promoting a positive culture in medical education that prioritizes learner well-being, increasing collaboration within the medical community and optimizing student resources. Despite the growing literature as universities implement services to address the well-being of medical learners, earlier reviews on this topic have not evaluated interventions in Canadian medical schools and have found it difficult to define medical learner well-being.12,13
The Wellness Innovation Scholarship for Health Professions Education and Health Sciences (WISHES) laboratory at the University of Calgary is taking a holistic approach to medical learner well-being.14 Based on Nussbaum’s human capabilities approach15 and acknowledging that well-being is multidimensional, 16 WISHES focuses on measurable outcomes within the domains of mental, physical, occupational, social, and intellectual well-being for individual learners and teachers, health professions education and training programs, and the intersection of the higher education system and the health care system.17
We conducted a scoping review that builds on previous literature and uses the WISHES holistic approach to well-being to explore the breadth and depth of interventions that aim to ultimately improve well-being among medical learners in Canada.
Methods
Study design
Based on Joanna Briggs Institute’s Review Manual18 and the Arksey–O’Malley methodological framework,19 we used 5 steps for our review: identifying the research question, identifying relevant studies, study selection, charting the data, and collating, summarizing and reporting results.
Identifying the research question
Our primary research question was “What is the breadth and depth of interventions aimed to improve well-being among Canadian medical learners?” We included any intervention that aimed to improve well-being of medical learners in Canada, with any comparator or outcome.
Identifying relevant studies
We searched MEDLINE, EMBASE, CINAHL and PsycINFO from inception to July 11, 2020. We developed search strategies with an experienced medical librarian (D.L.L.), which combined synonyms and subject headings from 3 concepts: medical learners in Canada, well-being and interventions. We also searched review databases to identify review articles to screen reference lists for studies missed in our initial search. One author (S.J.M.) conducted all searches and reviewed reference lists. The complete MEDLINE search strategy is provided in Appendix 1, Supplemental Table 1, available at www.cmajopen.ca/content/9/3/E765/suppl/DC1.
Categorization of well-being domains21
Our inclusion criteria were that studies from any publication year be primary research of interventions (e.g., mentoring, or educational interventions) for medical learners in Canada that aimed to improve well-being. We excluded studies if they were not primary research (e.g., editorials) or did not report any outcome from an intervention aimed to improve well-being. We defined a medical learner as an individual registered in an academic institution whose program is housed in a Canadian medical school and pertains to research or treatment of diseases and injuries or relating to medicine (i.e., undergraduate medical student, postgraduate medical student [resident physician], undergraduate nonmedical [health sciences] student, graduate science [MSc or PhD] student).20 We defined an intervention as any randomized or nonrandomized experimental study. We included studies if well-being was 1 component of a multicomponent intervention (e.g., education intervention to address intellectual well-being, not just clinical skills). We selected domains of well-being (i.e., social, mental, physical, intellectual, occupational)14 for our scoping review based on a needs assessment performed among medical learners at a Canadian medical institution; we validated operational definitions for domains.21
We used broad inclusion criteria (inclusive of all medical learners) to explore the breadth and depth of well-being support among medical learners as they transition through their studies into a health care profession. Understanding the comprehensiveness of well-being support throughout the academic trajectory will benefit efforts to develop effective interventions for students as they transition through medical education.22
Study selection
Three authors (S.J.M., K.W., M.A.) reviewed titles and abstracts, independently and in duplicate, after achieving 100% agreement on a pilot test of 50 random studies. The same authors reviewed the full text of selected articles, independently and in duplicate; we included articles in the final review if both reviewers agreed on inclusion. A fourth author (A.K.) resolved disagreements.
Charting the data
Independently and in duplicate, we (S.J.M., K.W., M.A., A.K.) charted data for included studies using a data collection sheet that was developed and piloted by the review team, resolving discrepancies through discussion. We collected information on document characteristics (e.g., year, geographic location), study characteristics (e.g., medical school, time frame), learner group, intervention domains (i.e., social, mental, physical, intellectual, occupational), level of intervention (i.e., individual, program, system), outcomes (e.g., assessment measures, themes or theories), limitations and conclusions.
Data analysis
We synthesized findings descriptively (Table 1) and categorized the level of intervention as targeted to the individual (i.e., the individual learner or group of individual learners), program (i.e., the program in which the learner is enrolled) or system (i.e., the academic institution or health care system in which learners learn or work). We recorded the primary level for each intervention. We categorized outcomes within 5 validated domains of well-being21 that represent part of the multidimensional construct of well-being: social (e.g., equity, diversity), mental (e.g., mindfulness, emotions), physical (e.g., exercise, nutrition), intellectual (e.g., tools, education) and occupational (e.g., research, resident rotation). Multiple outcomes (within multiple domains) could be recorded for each intervention.
We (S.J.M., K.W., M.A., A.K.) synthesized results from included qualitative studies using thematic synthesis for reviews on health research.23,24 We developed discrete themes that represented findings reported in primary studies, and considered these themes to generate new interpretive constructs, explanations or hypotheses.25 We integrated our qualitative and quantitative findings by using qualitative results to interrogate quantitative results, to identify research gaps and to synthesize lines of inquiry.26
We classified reported outcomes for each well-being domain as statistically significant if p < 0.05. We calculated descriptive statistics using STATA IC15 (StataCorp).
Ethics approval
We did not require ethics approval as all data were available in published records.
Results
Of 1753 relevant studies identified, we included 65 interventions that aimed to improved medical learner well-being (Figure 1). Characteristics of included studies are in Appendix 2, Supplemental Table 2, available at www.cmajopen.ca/content/9/3/E765/suppl/DC1.27–91

Study flow diagram.
The 65 included studies27–91 were published between 1973 and 2020, and were conducted most frequently at University of Toronto (n = 16, 25%) or McGill University (n = 8, 12%) with undergraduate (n = 34, 52%) or postgraduate medical education students (n = 31, 48%) (Figure 2). Figure 3 illustrates the cumulative number of published studies on interventions. Among 44 studies that reported implementation year, the median was 2010 (range 1971–2018). The median intervention duration, reported from 47 studies, was 3 months (range 1 h–48 mo). Most studies (n = 52, 80%) were uncontrolled trials, of which half were implemented with undergraduate medical students (n = 26). We included 16 qualitative studies; most (n = 9) were conducted with undergraduate medical students. Resident physicians were commonly from family medicine (n = 6) and pediatrics (n = 6), which included pediatric subspecialties (n = 2); generalist practice was more broadly defined (n = 4).

Medical schools and learners represented among included studies.

Cumulative number of published studies on interventions for medical learner well-being.
Fifty-one (78%) interventions targeted intellectual (e.g., clinical skills modules46) well-being and 32 (49%) targeted occupational well-being (e.g., resident rotation bundle47); 23 (35%) targeted both domains (e.g., specialty exploration and discovery programs92). Among 19 interventions for individuals, most (n = 14) were for medical students. Program interventions (n = 27) were primarily for resident physicians (n = 17). Medical students and residents were represented similarly in system interventions (undergraduate, n = 9; postgraduate, n = 10). Two system interventions were for undergraduate health sciences students. Few studies (n = 2) incorporated formal mentorship programs in their intervention as a method to promote learner well-being. Only 3 studies considered barriers or stigma among medical learners to accessing appropriate mental health services.
Quantitative studies
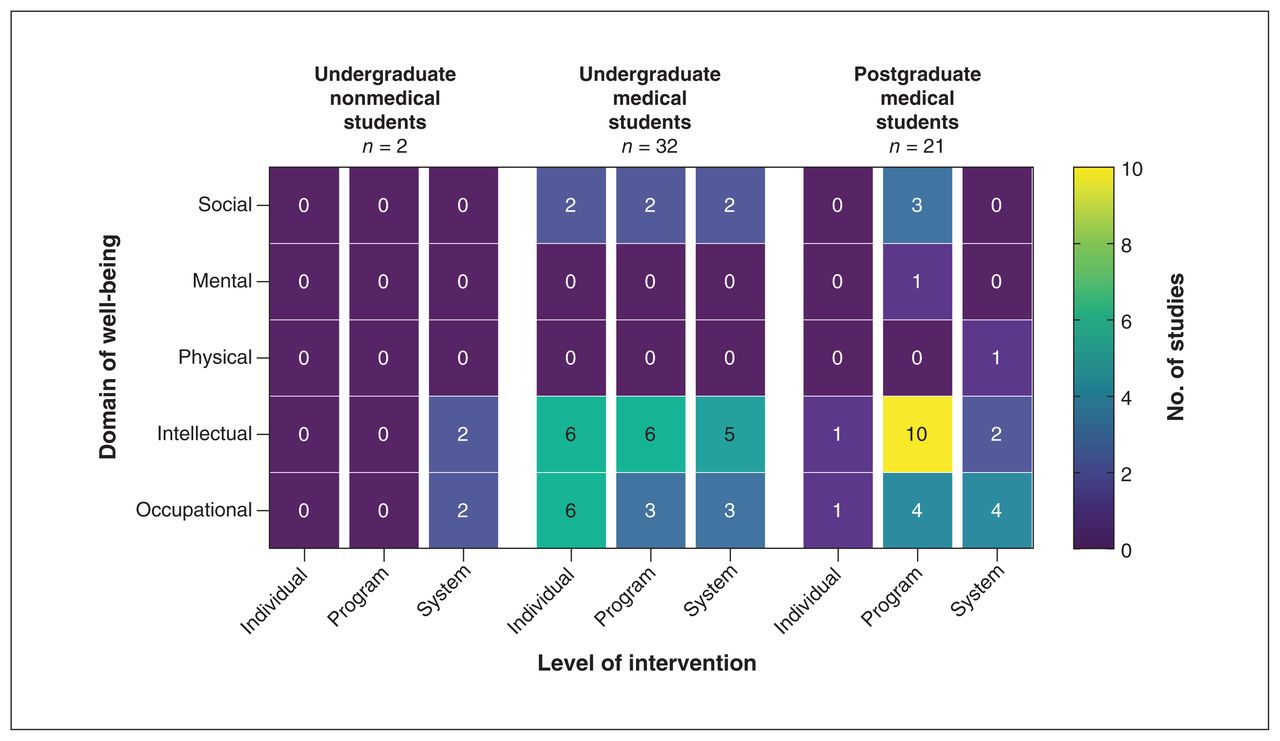
Quantitative outcomes are reported in Appendix 3, Supplemental Table 3, available at www.cmajopen.ca/content/9/3/E765/suppl/DC1. Statistical evaluation of interventions was explored extensively (n = 41, 63%), namely evaluating perceptions of well-being pre- and postintervention, satisfaction with the intervention, and determining attitudes and agreement regarding use of interventions. Figure 4 illustrates the number of studies that reported a significantly positive effect of interventions by well-being domain, level of intervention and learner group. In Appendix 4, available at www.cmajopen.ca/content/9/3/E765/suppl/DC1, we provide summaries on assessment tools used to measure outcomes within well-being domains, as well as a summary of statistical findings.
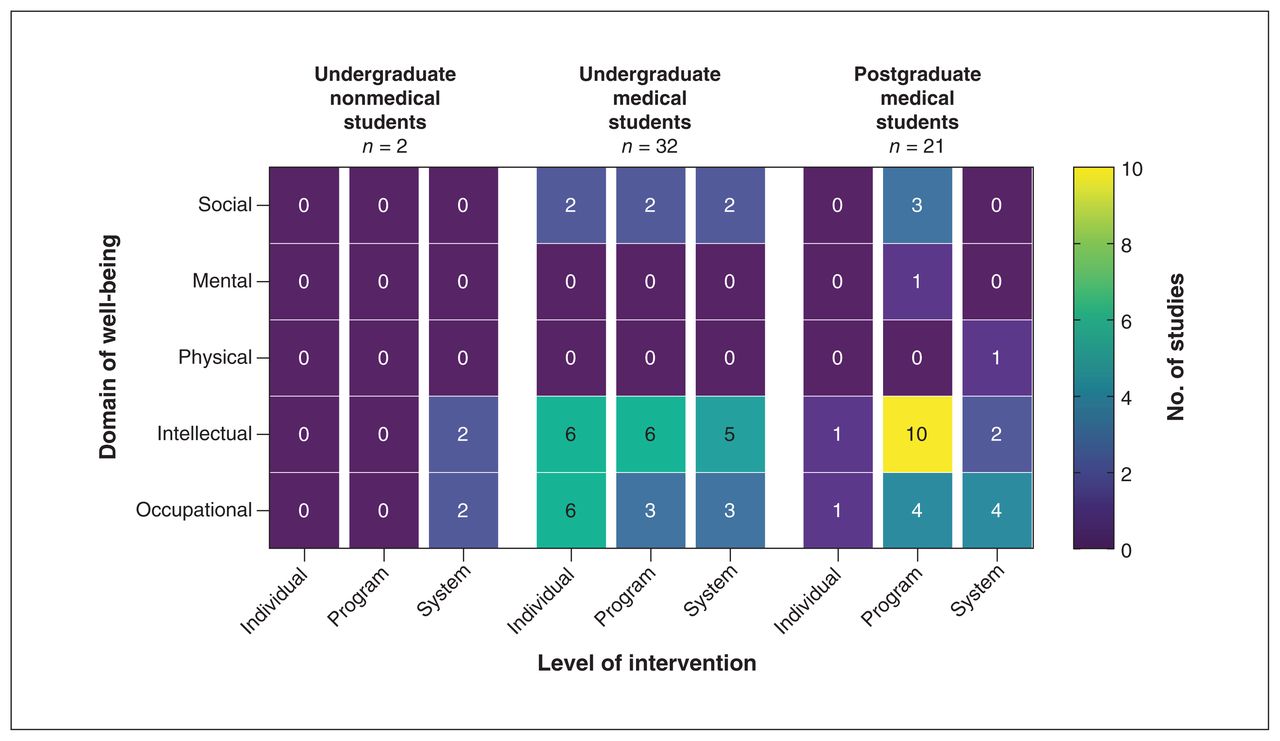
Number of studies that reported significantly positive effects of well-being interventions by well-being domain, level of intervention and type of learner. Note: One level of intervention was recorded from each included study. More than one well-being domain could be recorded from a single study.
Qualitative studies
Sixteen studies explored well-being qualitatively. Most (n = 12) focused on promoting and understanding intellectual well-being in medical education (Table 2). Five qualitative studies reported favourable outcomes; 3 studies concluded that formal audit is needed34,79,77 and 2 studies uncovered shortcomings related to postgraduate education content (i.e., intellectual, occupational well-being)84 and undergraduate medical education leadership (i.e., social, intellectual well-being).33
A key finding was that well-being among learners is a multidimensional construct that includes 4 components: genuine sense of personal fulfillment and gratification in medical education, grounded understanding of requirements for medical education programs, enhanced peer cohesion and functionality, and promoting cognitive flexibility to strengthen knowledge for diverse perspectives. Three conditions were identified as predicting and promoting well-being: effective coping and emotional regulation through individual strategies, individual and program affirmation of the role of being a learner in a medical school, and systems that favour attributing meaning to being a learner. Qualitative studies provided insight into catalyzing the shift from reducing manifestations of distress to proactively optimizing well-being.
Interpretation
We conducted a scoping review of published interventions conducted in Canadian medical schools to improve the well-being of medical learners. Our review shows that many Canadian medical schools address intellectual, occupational and social well-being through interventions targeted to individual medical learners and their respective programs, within the medical education system. The well-being of graduate students in health sciences programs does not appear to have been addressed through targeted interventions. Across all medical learners in Canada, mental and physical well-being is an important area that requires further exploration.
Few included studies used formal faculty adviser or mentor programs as a method to promote social well-being. Mentorship is an interactive process to encourage learning and development, grounded in social learning principles,93,94 that has been used extensively in medical schools in the United States.12 Academic mentors model the importance of key components of social well-being — inclusion, diversity and professionalism — in medical education.95 Formal mentorship programs that are integrated with curricular content can be used to offer career guidance to graduate science researchers, 96,97 or to develop clinical skills among medical students98 and resident physicians.99 Mentorship programs for social well-being report high satisfaction,100,101 career promotion,102 improved clinical performance103 and patient safety.104 We encourage Canadian medical schools to consider social well-being among their medical learners.
Barriers to mental health treatment for medical learners are common105,106 and important to recognize for effective mental health interventions.107,108 Learners with mental health disorders and symptoms are often undiagnosed and undertreated. 109 We found a gap in increasing access and reducing stigma around mental health interventions within Canadian medical schools. In 2019, Wilkes and colleagues surveyed 69 undergraduate medical students and reported that 83% of students considered medical education a source of stress, and 70% met criteria for exhaustion; however, only 36% of students reported seeing a mental health professional to address mental health concerns.110 There is a need for formal programs focused on mental well-being, inclusive of increasing awareness, reducing stigma and improving access to mental health services. Although such programs are associated with lower depression and suicidal ideation rates in the United States, the effectiveness of this approach in Canadian medical schools is unknown.111
We found a scarcity of interventions aimed to improve the physical well-being of medical learners.112 Physical well-being does not have comparable widespread acceptance as an aspect of physician well-being.113,114 Adherence to various dimensions of physical well-being is low among undergraduate medical education students.115 In an online cross-sectional survey of fourth-year medical students at the University of British Columbia, Holtz and colleagues showed that those who perceived exercise counselling to be highly important to clinical practice participated in daily physical activity.116 Although it may be hubristic to suggest interventions to improve learner physical well-being will improve patient outcomes, 117 we contend that encouraging physical well-being should be a core component in developing competent and professional future physicians.118
Many interventions in Canadian medical schools promote collectives of learners to encourage a collaborative state of mind rather than peer-to-peer competition. All but 2 Canadian medical schools have adopted a pass/fail grading system for medical education.119 A pass/fail system has been shown to improve intellectual well-being,120 enhancing teamwork among learners121 without negative impact on academic performance.122 Pass/fail grading systems, complemented by standards-based evaluations, are a step along the continuum to recognizing learners as professionals, enhancing intellectual well-being and preparing medical students for life as enduring learners.123,124 Further, many studies reported that medical learners have higher satisfaction and greater achievement of knowledge-related outcomes when skills are taught in condensed workshops, ranging from 2 hours,59 to 5 days,41 to 2 weeks.51 More research is needed to understand massed versus dispersed learning to maximize intellectual well-being.
Occupational well-being is an increasingly researched area in Canadian medical schools, particularly in resident trainees. 125 Compared with physicians, residents in Canada have a 48% increased risk of burnout, 95% increased risk of depression and 72% increased risk of suicidal thoughts.126 Residency programs play a predominant role in the occupational well-being of residents; medical leaders have stressed the need for universities to make occupational well-being a core competency of medicine by redesigning medical programs.127 We found many interventions that aimed to improve occupational well-being at the program and system level by addressing culture, learning and work environments; however, more research is needed to ensure that efficacious interventions are effectively implemented in a contextually adaptive manner to respond to individual learner needs.
We suggest 3 key directions when considering future interventions. First, positive psychological outcomes are important,128 given that positive psychological adaptations evolve to meet the demands of stressful experiences.129,130 Highly resilient individuals are known to cultivate positive adaptations proactively;131,132 it is unknown whether or not positive psychological adaptations are by-products of interventions or whether they improve coping. Future interventions for improved mental well-being should consider the aggregate of negative and positive mental well-being outcomes.
Second, the well-being of graduate science education students in Canada has not been considered widely. Scientific research is an important element in graduate science education programs, and learners conducting scientific research may face unique well-being challenges.133,134 In Canada, the integrative MD-PhD program is a popular approach for training physician-scientists,135 representing a substantial investment of institutional, federal and societal resources.136 Medical schools might consider interventions for all learners conducting scientific medical research to augment their success as future investigators.
Lastly, process evaluation is needed to assess the implementation of interventions and outcomes over time. Though most studies reported positive improvements, it is possible that interventions were not reliably delivered or consistently adhered to.137 As others have mentioned,12 we suggest that intervention evaluations include the study of sequential phases of implementation to determine synergies among well-being domains associated with improvement in learner well-being. Interventions may have adverse effects that should be weighed against potential benefits,138 and success during one stage of training may not be helpful during the next stage of training.139
Limitations
The protocol for our review was not registered; we included only primary studies and did not search grey literature, which may fill gaps we identified or report interventions with negative outcomes. Our definition of medical learner is not a validated definition.20 We categorized studies based on 5 domains of well-being, but there may be other well-being domains related to medical learning (e.g., spirituality).140 We found authors nearly exclusively reported successes and few failures, which suggests positive publication bias. Given the multidimensional constructs of interventions, it was not possible to determine specific components of interventions associated with more favourable outcomes. The lack of a universal definition for learner well-being added complexity to study selection, but our broad inclusion criteria allowed us to produce a comprehensive summary of literature. Our review was limited to medical learners in Canada and the included studies did not report on subpopulations of learners (e.g., Indigenous students, international students). We were unable to comment on different race and ethnocultural factors influencing the learning experience.141
Conclusion
Interventions to improve the well-being of medical learners in Canadian medical schools vary. Many Canadian medical schools have addressed intellectual, occupational and social well-being through interventions targeted to individual medical learners, their medical learning programs or the educational or health care systems. The well-being of graduate students in health sciences programs does not appear to have been addressed through targeted interventions. Across all medical learners in Canada, mental and physical well-being is an important area for further exploration. Comprehensive and inclusive interventions aimed to improve well-being for medical learners in Canada are needed.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Stephana Moss and Aliya Kassam conceived and designed the study. All authors contributed to data acquisition, analysis and interpretation. Stephana Moss and Aliya Kassam drafted the manuscript, which all authors critically revised. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was funded by the Office of Postgraduate Medical Education and supported by the Office of the Senior Associate Dean of Education at the Cumming School of Medicine.
Data sharing: All data presented are available in the published record.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/9/3/E765/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2021 CMA Joule Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools





