


Abstract
Background: Health care delivery shifted rapidly during the COVID-19 pandemic, whereby virtual consultations replaced many face-to-face interactions. We sought to gather patient perspectives on their experiences with virtual surgical consultation, the advantages and disadvantages of this delivery method and their overall satisfaction with virtual appointments.
Methods: We conducted a patient-oriented, cross-sectional study. Adult patients (age > 18 yr) who had a virtual consultation with a participating general surgeon in Saskatoon, Saskatchewan, from April to May 2020 were eligible. We conducted telephone interviews using open- and close-ended questions. We used thematic analysis to determine themes from the qualitative data. As research team members, 2 patient partners were involved in identifying priorities, developing the research question, designing research methods, analyzing data and disseminating findings. We analyzed and presented quantitative data descriptively.
Results: We interviewed 45 participants from 7 general surgery practices; the average age was 62 years. Most participants lived outside Saskatoon and had virtual follow-up appointments. The 3 themes related to advantages of virtual consultations were convenience, cost savings and decreased exposure to pathogens. The 4 themes related to their disadvantages were that they were not as personal, the surgeon was not able to perform a physical examination, and there were issues with scheduling and issues with technology. Most participants were satisfied with the care they received (n = 41) and would be willing to use virtual consultation in the future (n = 31).
Interpretation: We found that virtual consultations are an effective and efficient way to deliver surgical care but are not appropriate for every situation and cannot completely replace face-to-face interactions. Our study identified the advantages and disadvantages of virtual surgical consultation to help better guide the delivery of virtual care in the future.
Plain language summary: During the COVID-19 pandemic, doctors started meeting with their patients by phone or video instead of in person. We asked 45 people what they thought about their phone or video visit with their surgeon. Most people were happy with their visit and thought they got the same level of care as they would in person. Many people liked that they could be at home and that they did not have to spend money on travel or to take time off work. People also felt safer because they did not have to risk catching COVID-19 at their doctor’s office. Some people were concerned about how visits were scheduled and that the surgeon could not examine them after surgery. People did not like these types of visits when the surgeon had to deliver bad news. Many people preferred phone or video appointments and would be willing to have these types of visits again.
Over the past decade, virtual consultation has become an increasingly popular resource in the medical world1 and has expanded to encompass many different clinical areas of medicine, including specialist consultation.2,3 In March 2020, the delivery of health care shifted rapidly to a virtual format.4–8 Virtual appointments are now being used in almost every context of surgical care, including initial consultation, imaging and pathology follow-up, as well as postoperative care.2,3 The Saskatchewan Medical Association introduced temporary billing codes for virtual consultation in the spring of 2020, which have since been replaced by permanent ones.9 Virtual consultation (including both telephone and video appointments) has the ability to reduce many of the barriers that patients experience when trying to access medical services and allows them to receive the care they need from the safety of their homes.10 Although there have been concerns about virtual care not being appropriate for all situations, initial studies have shown that virtual consultation for surgical services can be equally as effective as in-person appointments for patient outcomes and patient satisfaction.2,3,11–13
Virtual care is especially relevant given Canada’s geography, as rural populations often have no readily available specialist services, and patients are required to travel many hours for consultations and follow-up appointments.14–16 We have seen a rapid implementation of virtual services across the provinces, with more than one-third of all medical appointments in Canada in 2021 being performed virtually.15,17 The federal government has also committed a substantial amount of money to help accelerate the implementation of virtual services.15,18 The goal of our research was to analyze the initial implementation of virtual surgical consultation in Saskatoon, Saskatchewan, in the context of the COVID-19 pandemic. We sought to gather patient perspectives on their experiences with virtual surgical consultation, the advantages and disadvantages of this delivery method and their overall satisfaction with virtual appointments.
Methods
Study design and setting
We conducted a patient-oriented, cross-sectional study using telephone interviews that took place from April to December 2020 in Saskatoon, Saskatchewan.19,20 Saskatoon, the largest city in Saskatchewan, houses roughly one-quarter of the total population.21 Three academic hospitals provide surgical services from which we drew our study sample.
Our study team included 2 patient partners (H.D., B.M.) who had previous experience with patient-oriented projects, as well as personal experience with virtual surgical consultations. Our study team had previous experience with qualitative research (G.G., T.C., M.A., K.I., H.D.) and with virtual consultation from a provider perspective (G.G., K.I.). We reported our study using the Guidance for Reporting Involvement of Patients and the Public (GRIPP2) and the Consolidated Criteria for Reporting Qualitative Research (COREQ).22,23
Participants and recruitment
All 17 general surgeons who were involved with the acute care surgery service in Saskatoon were contacted via email from a study author (K.I.) in March 2020 to invite patients for the study. Any patient older than 18 years who had a telephone or video appointment with one of the participating surgeons between April and May 2020 was eligible to participate. Patients who did not consent to take part were excluded. Surgeons initially asked participants during their appointment if a research team member could follow-up with them. Participants were then recruited via email or telephone by the surgeons’ medical office assistants or the student researcher (K.I.). Those who agreed to participate gave verbal consent before the interview. We recruited and conducted interviews between April and December 2020.
Data source and collection
With our patient partners (K.I., H.D., B.M., G.G.), we developed a brief, semistructured interview guide, adapted from the literature (Appendix 1, available at www.cmajopen.ca/content/10/4/E1008/suppl/DC1).12 The guide contained both open- (n = 8) and close-ended (n = 5) questions. Close-ended questions were mostly binary and pertained to satisfaction. We included probing questions with the open-ended questions and allowed participants to expand on advantages and disadvantages. All interviews occurred via telephone (K.I.). We also informally collected demographic information for descriptive statistics after obtaining consent, before starting the interview (K.I., M.A.).
Patient engagement
Our research team used the Saskatchewan Centre for Patient-Oriented Research (SCPOR) Patient-Oriented Research Level of Engagement Tool (PORLET) to guide our engagement with patient partners.24 We recruited 2 patient partners (B.M., H.D.) through SCPOR’s patient and researcher connection site.25 Researchers and patient partners identified virtual surgical consultation as a priority for the study. The patient partners were part of all 7 team meetings held over video conference, from the research proposal stage to completion of the manuscript. Patient partners codeveloped recruitment methods and interview questions, and undertook qualitative analysis by identifying themes and contributing to interpretation. They helped write, edit and review the manuscript, and advocated for findings to be integrated into surgical practice by copresenting at research conferences.
Data analysis
All interviews were audio-recorded and then transcribed by the Canadian Hub for Applied and Social Research.26 We uploaded transcripts to NVivo version 12 for coding and analysis. We ceased interviews when no new themes were being identified and performed a retrospective analysis to ensure data saturation.27 The research team coded the interview data from the open-ended questions (K.I., H.D., B.M., M.A.), which we then sorted into relevant groupings as overarching themes and subthemes using a thematic analysis approach (K.I., H.D., B.M., T.C., M.A.).28–30 We then categorized the main themes into advantages and disadvantages using a deductive approach based on our research question.31 Regular team meetings were held throughout the analysis process for discussion and peer debriefing.30
We conducted a descriptive statistical analysis of the responses to close-ended questions (K.I., M.A.).
Ethics approval
This study was approved by the University of Saskatchewan Behavioural Research Ethics Board (BehID-1827).
Results
Of the 17 invited surgeons, 12 agreed to participate; however, only 7 provided patients for the study, as the other 5 did not schedule virtual consultations during the study period. The remaining 5 surgeons either did not reply or did not provide patient contacts. Subspecialties of participating surgeons included colorectal surgery, hepatobiliary surgery, surgical oncology, and acute care and trauma; these surgeons’ practices represented all 3 academic hospitals. Sixty patients were contacted to participate and 45 consented to an interview. We conducted all interviews via telephone. Interviews ranged from 2 to 8 (mean 4) minutes, not including project description or consent. Demographic and appointment information is summarized in Table 1.
Participant demographic and appointment information
The interview contained several close-ended questions pertaining to overall satisfaction with the virtual consultation method, preference for appointment type and future willingness to use a virtual platform (Table 2). Many participants were satisfied with the virtual consultation process (91%) and stated they would use it again in the future (70%). However, given the choice, less than half of participants would prefer a virtual consultation (38%) and many said it would depend on the circumstances (38%). Most participants felt that their care was not compromised in any way by a virtual appointment (87%). Only 2 patients reported concerns about privacy of information.
Summary of close-ended question responses
Table 3 outlines how most participants were satisfied and would be willing to use virtual consultation in the future regardless of their age, sex, how far they lived from Saskatoon or whether their appointment was an initial consult or follow-up.
Overall satisfaction and future willingness to use virtual consultation based on participant age, sex, location and appointment type
Themes
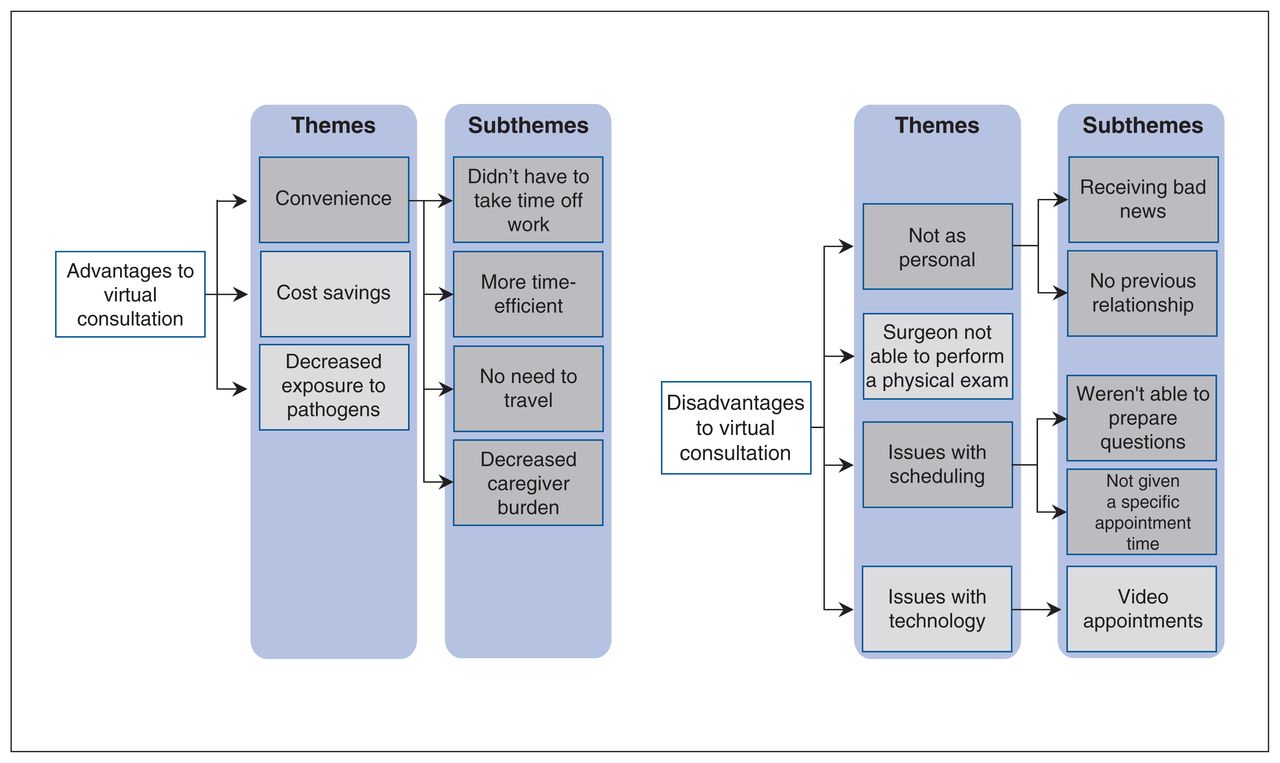
The results from the analysis of the open-ended interview responses are described in Figure 1. We categorized 3 main themes as advantages to virtual consultation, namely convenience, cost savings and decreased exposure to pathogens. Under disadvantages to virtual consultation, we identified 4 main themes, namely that it was not as personal, the surgeon was not able to perform a physical examination, and there were issues with scheduling and issues with technology (Appendix 2, available at www.cmajopen.ca/content/10/4/E1008/suppl/DC1).
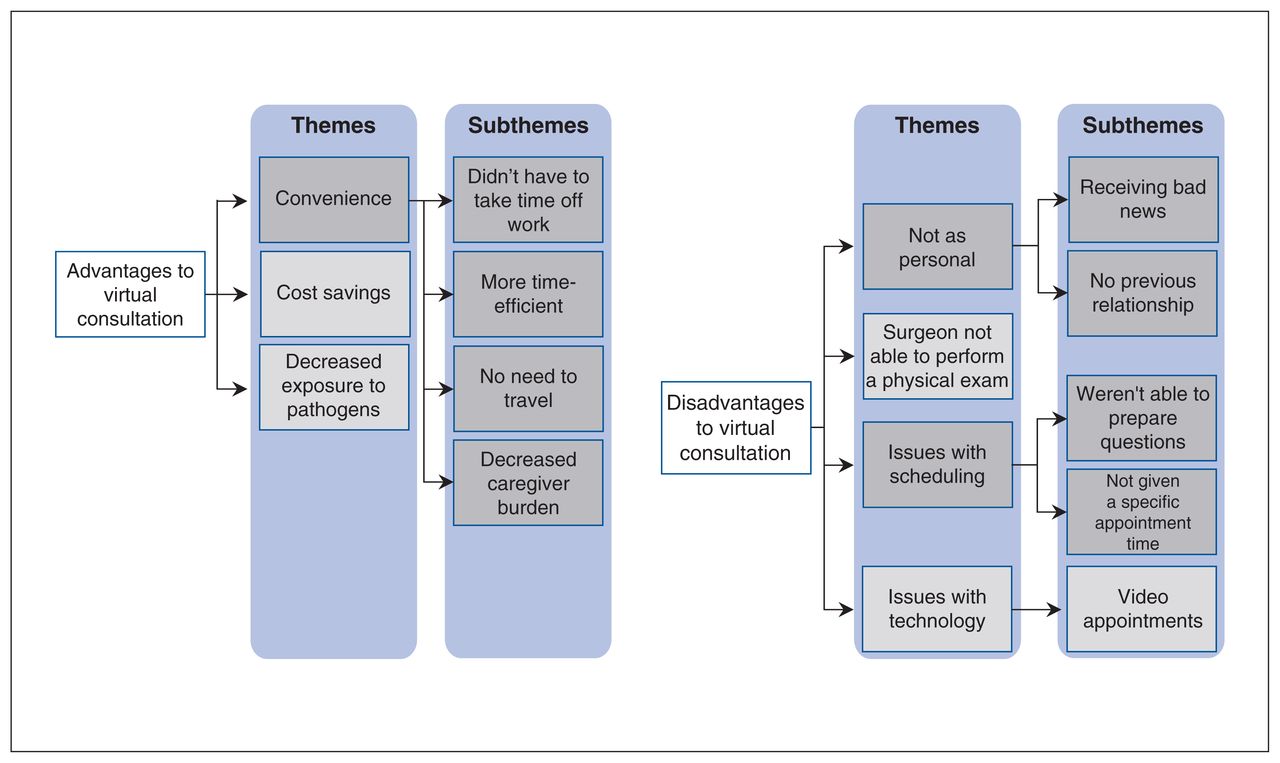
Themes and subthemes for patient perspectives on virtual consultation.
Convenience
Convenience was the most prominent theme identified, with 4 subthemes, namely that participants did not have to take time off work, that virtual consultation was more time-efficient, without the need to travel, and that virtual appointments decreased caregiver burden (Table 4).
Participant quotes related to the advantages of virtual surgical consultation
Cost savings
Saving money related to gas, lodging, parking and transportation was reported by many participants (Table 4).
Decreased exposure to pathogens
Exposure to viruses and other communicable diseases was a serious concern for participants, and doing the consultation remotely helped to avoid this exposure (Table 4).
Not as personal
Participants felt that they were not able to connect with their surgeon in the same way virtually as they could in person. With this, we identified subthemes of the disadvantage of receiving bad news virtually and difficulties for participants who had no previous relationship with the surgeon before meeting them virtually (Table 5).
Participant quotes related to the disadvantages of virtual surgical consultation
Surgeon not able to perform a physical examination
A major concern for participants was the inability of the surgeon to examine them physically or look at their wounds postoperatively (Table 5).
Issues with scheduling
Two subthemes under this theme were that participants often were not given a specific appointment time and were not prepared to ask questions via the virtual modality (Table 5).
Issues with technology
The main subtheme that arose from this theme was not being able to conduct video appointments (Table 5).
Interpretation
Our findings indicate that virtual surgical consultation is an acceptable alternative to in-person appointments but may not be appropriate for every situation. Most participants found virtual consultation to be more convenient as it saved time, money and the need to travel. It also decreased family and caregiver burden and reduced patients’ exposure to potential pathogens. Disadvantages of virtual consultation were that some participants found it less personal, and that it was not sufficient when a physical examination was required or if the patient was receiving bad news. There were also issues around scheduling appointments, and participants felt that they were not prepared to ask questions. Overall, participants were satisfied with the virtual consultation process and would be willing to use it for future surgical care.
The advantages of virtual consultation in this study were similar to those identified in other research.2,3,11 In particular, recent studies done have highlighted patients’ concerns regarding exposure to SARS-CoV-2.4–7 Conducting consultations virtually allows patients to adhere to travel restrictions, maintain social distancing measures and minimize risk of contracting the virus or other hospital-associated illness.5 Saskatchewan’s geographic distribution of health services requires many rural patients to travel long distances to receive specialist services.14 Participants appreciated not having to travel many hours, often during poor winter road conditions, to spend only a few minutes talking with their surgeon, a finding consistent with the literature.11–13 Similar to other studies,11,12 virtual consultation was considered more time-efficient for both the patient and the surgeon, and participants commented on shorter wait times for virtual versus in-person consultations. Virtual consultation was also described as negating barriers to accessing care such as travel and parking costs, as well as time off work to attend an in-person appointment. These were prominent themes for participants that lived both inside and outside of Saskatoon. Similar to other research, our study identified the ability of virtual consultation to alleviate caregiver burden for patients who require assistance attending in-person consultations.32
Virtual consultation may not be appropriate for all surgical appointments, and participants in our study identified several areas where this modality was limited. Patients preferred a set appointment time or a narrow time range for the appointment. Participants often noted they were only given a date for the appointment. If patients had an appointment time, they could prepare a list of questions and be in an appropriate setting to have a discussion. The inability to perform a physical examination is an obvious downside to virtual consultation, and this is well reported in the literature.33 Some research shows the use of video conference and smartphone technology to send photos could help to alleviate a portion of those concerns.4,5 Open communication is a vital part of developing relationships between patients and their medical providers, and the inability to rely on nonverbal cues and assess patients’ understanding of diagnoses and treatment options can make virtual consultation challenging.34 Participants often noted that the virtual consultations felt less personal, and participants found it more difficult if they had never met the surgeon previously. Interestingly, privacy of information was only a concern for 2 participants, although it has been documented in the literature.35
The increased use of virtual medical care calls for the need for a standardized approach.15,16 Currently in Saskatchewan, virtual care is not always delivered through a dedicated platform, and this leads to large variation in experiences.15,36,37 Virtual care can be a great tool to complement a complete patient care assessment and has a potential cost-saving benefit to the health care system.11 This raises the concept of a hybrid approach,38 whereby a virtual consultation is considered a component of the entire consultation process. This concept would require further research to determine its feasibility and effectiveness. The technological challenges related to video consultations is another area to be addressed, given that video appointments typically require more substantial infrastructure, increased user technical ability, a higher bandwidth Internet connection and a more formal approach on behalf of the surgeon.7,12,39 Our findings suggest that video consultations might be better received than phone consultations, and it is worth exploring how it might be used more frequently.39,40
Limitations
Because our sample had primarily telephone consultations with their surgeon (n = 41), it was difficult to assess the effectiveness of video consultation. All patients included in the study had already agreed to have a virtual appointment, resulting in possible selection bias. We were unable to interview participants from every surgical office in Saskatoon, and the offices provided us with the participants, contributing to potential sampling bias. In addition, some interviews took only a few minutes to complete, which could limit the quality of the qualitative data.41 Although the interview duration was short for a strictly qualitative method, most of the interview guide contained close-ended questions; we believe we were able to capture participants’ perspectives adequately in this time frame as our themes were consistent throughout interviews and with the literature. We examined surgical consultations only, and extrapolation of the findings may not be applicable to all medical specialties. We also did not clarify if follow-up appointments were for postoperative follow-up or for follow-up from other investigations, which would have a different clinical context and potentially different patient expectations. Participants were not specifically asked for suggestions for improvement.
Lessons learned from patient engagement
We were fortunate to have 2 patient partners that had substantial experience with the Saskatchewan health care system, as well as an interest in research and previous involvement in patient-oriented research projects. The patient partners contributed their personal experience with virtual consultation to help tailor the research project to address an area of health care they felt was important. Actively involving patient partners as full team members led to a research question that was relevant and could lead to system change in a timely manner. Open and frequent communication with the patient partners facilitated engagement and empowered their contributions to the research. As part of every team meeting, they helped to identify the concerns that would be most relevant to patients and ensured that the research was conducted in a patient-oriented manner with the goal of improving patient outcomes. We encouraged shared decision-making within our team and focused on relationship building.42 More specifically, the researchers made accommodations as needed to allow the patient partners to fully contribute, such as presenting data in visual formats, avoiding jargon, limiting the technological requirements and checking frequently to see if there was any way to make the process easier. By creating an environment that acknowledged the values, preferences and experiences of the patient partners, both were comfortable raising concerns and providing direction, resulting in a stronger research project that could lead to changes in health care with real value to patients.43 The patient partners repeatedly emphasized the importance of having our findings integrated into clinical practice and volunteered to copresent at upcoming research conferences.
Conclusion
Virtual consultation has the potential to deliver health care in a more convenient, cost-effective and timely manner, without compromising the quality of care. Overall, participants were satisfied with their virtual appointments, and many participants commented not only on their willingness, but their preference, to use virtual consultation for future surgical care. Virtual surgical consultation is a promising modality that requires ongoing study to optimize its delivery. It may not be perfect for every patient or every situation, but virtual consultation has many benefits, and we argue it should continue to be offered to patients in a postpandemic world.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: All of the authors contributed to the conception and design of the work, and the acquisition, analysis and interpretation of data. All of the authors drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: Supplemental funding for patient partners was provided through the Saskatchewan Centre for Patient-Oriented Research.
Data sharing: Data are available upon request to the corresponding author.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/10/4/E1008/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2022 CMA Impact Inc. or its licensors
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.