


Abstract
Background: The advantage of coronary artery bypass grafting (CABG) over percutaneous coronary intervention (PCI), established in trials, may not be generalizable to populations in which the method of treatment determines the time to treatment. We sought to describe the methodology of a population-based observational study for assessing how changes in time to treatment may affect the comparative effectiveness of these 2 methods of coronary revascularization.
Methods: We propose a framework of causal mediation analysis to compare the outcomes of choosing CABG over PCI, if patients selected for either method waited the same amount of time had they undergone a PCI. We will include patients who underwent a first-time, nonurgent isolated CABG or single-session PCI for multivessel or left main coronary artery disease from January 2001 to December 2016, in British Columbia. We will use absolute risk difference as a measure of the total effect of choosing CABG over PCI and partition it into the direct effect of the treatment choice and the effect mediated by the treatment-specific timing.
Interpretation: Understanding how time to treatment mediates the relation between method of revascularization and outcomes will have implications for treatment selection, resource allocation and planning benchmarks. Findings on the benefits and risks of performing PCI or CABG within a certain time will guide multidisciplinary teams in determining the appropriate revascularization method for individual patients.
There has been debate about the appropriate treatment method for patients with multivessel or left main coronary artery disease who do not need emergency treatment.1–4 Recent clinical guidelines favour coronary artery bypass grafting (CABG) over percutaneous coronary intervention (PCI) for patients with the cardiac anatomy suitable for either procedure.5–8 This recommendation reflects findings from randomized controlled trials (RCTs) showing that CABG, relative to PCI, results in higher or similar survival, but fewer cardiac events and less need for repeat revascularizations. 9,10 However, the findings of RCTs in which the time from decision to treatment is the same for both procedures may not apply to populations in which the method of treatment determines the time to treatment, with times to CABG being longer than times to PCI.11,12 The therapeutic effect of revascularization can vary over time. Disease progression during an extended treatment delay is thought to increase disease severity and lead to incomplete revascularization.13,14 Factors that cause variation in time to treatment may also cause the comparative effectiveness of the 2 treatments to vary from one patient to another. As the clinical guidelines do not address the relative benefits of CABG when treatment is delayed,5,8 it is unclear whether patients will have better outcomes if they undergo PCI instead of CABG, given the uncertain timing of CABG.
We describe a conceptual framework to assess how changes in time to treatment may affect the comparative effectiveness of these 2 methods of coronary revascularization. We justify the use of a causal mediation analysis by showing the need to compare counterfactual scenarios to assess how the differences in outcomes would have changed if patients who received CABG had the same treatment time as patients who received PCI. This new evidence will make it easier to determine the appropriate care for patients and guide decisions about resource allocation.
Methods
We describe the framework for examining the effect of the changes in CABG treatment time on the difference in outcomes between CABG and PCI. We will use an observational study to assess the extent to which times to treatment mediate the comparative effectiveness of the 2 treatment methods. We will use the Strengthening the Reporting of Observational Studies in Epidemiology statement for reporting the results of our study.15
Study setting
The Canadian province of British Columbia has a population of about 4.6 million people and has publicly funded physician and hospital services.16 Cardiac Services BC, a provincial health authority program, is responsible for supporting timely access and quality of specialized cardiac care provided at 5 tertiary centres.17 The time frame will be between Jan. 1, 2001, and Dec. 31, 2016, when PCI with stents became standard practice. Before 2001, patients were mainly treated with balloon angioplasty, a technique associated with a high rate of repeat revascularization.18 The timing for PCI often coincides with the time of diagnostic catheterization regardless of the urgency of the treatment, whereas CABG is booked after and prioritized according to urgency.12,19
Conceptual framework
Box 1 describes the conceptual framework we will use for investigating the effect of changes in the time to treatment on the difference in outcomes of revascularization with CABG and PCI in patients with stable angina and complex coronary artery disease.
Conceptual framework for investigating the effect of changes in the time to treatment on differences in outcomes of revascularization with coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) in patients with stable angina and complex coronary artery disease
The premise of appropriate care is timely access to needed treatment.
CABG is thought to have better capacity for preventing cardiac events after initial revascularization.
When the cardiac anatomy is suitable for either CABG or PCI, the chosen method determines time to treatment.
The longer times to treatment for CABG may lessen the relative benefits of this procedure as established in clinical trials.
The appropriate choice of the revascularization method considers effectiveness of CABG compared with PCI by treatment timing.
The policy analysis speculates about outcomes if a patient having CABG were to have the same time to treatment as a patient having PCI.
Randomization by method and timing would fail to distinguish the effect of treatment from the effect of treatment-induced timing.
Mediation analysis partitions the overall effect of CABG compared with PCI into the effects from treatment and timing.
The concept of naturally occurring treatment times is fundamental to this mediation analysis.
The effects are obtained using the potential outcomes approach for hypothetical scenarios of treatment and timing.
The results of this study will facilitate the determination of appropriate care for patients and will guide resource allocation.
Note: CABG = coronary artery bypass grafting, PCI = percutaneous coronary intervention.
Evaluation problem
Our study will assess the difference in outcomes of 2 methods of coronary revascularization under the hypothetical scenario that patients selected for either method wait the same time as had they undergone PCI (Box 1). Determining this difference would require testing the same patient population twice, once with each method, yet doing so would be impossible in the RCT setting. Even if delaying necessary treatment were a true intervention, replacing the time to treatment induced by CABG selection with the time induced by PCI selection would not be equivalent to conducting an experiment in which intervention groups had a fixed time to treatment at the time of random assignment to CABG and PCI.20 To determine how long a patient having CABG would wait if treated with PCI instead, that patient must first be treated with PCI, and would then no longer be eligible for the CABG arm. However, we can imagine what would happen if CABG were performed in the time frame typical for PCI. We would consider 3 hypothetical scenarios, each applied to the entire study population (labelled A, B and C in Box 2), and would assess whether the relative benefit of CABG established by comparing scenarios A and B would change if scenarios A and C occurred instead. A comparison of scenarios A and B shows the effects of existing health care delivery,21 whereas comparing scenarios A and C provides insight into the implications of enabling access to CABG in a time frame typical of PCI.
Hypothetical scenarios considered in the mediation analysis
All patients undergo PCI with the naturally occurring timing of PCI.
All patients undergo CABG with the naturally occurring timing of CABG.
All patients undergo CABG but with the naturally occurring timing of PCI.
Note: CABG = coronary artery bypass grafting, PCI = percutaneous coronary intervention.
Appropriateness of timing
For cases in which the cardiac anatomy is suitable for either treatment, it is unclear whether it is appropriate to recommend CABG, which is likely to be delayed, if PCI can be performed earlier. Traditionally, appropriate care has been linked to the benefits and risks of the revascularization procedure.7 Doenst and colleagues3 have hypothesized that CABG has better capacity for preventing cardiac events after initial revascularization on the premise that PCI targets flow-limiting narrowing, whereas CABG restores flow beyond the narrowing.
Our concern is the benefits and risks associated with the time to treatment. We observe that a choice of the revascularization method will influence when the patient undergoes treatment, a mediating factor that affects outcomes by prolonging the patient’s exposure to narrowing in the coronary artery (Figure 1). Therefore, for coronary revascularization, the appropriateness of care should address the concern that some patients may not receive treatment when they would benefit most.11
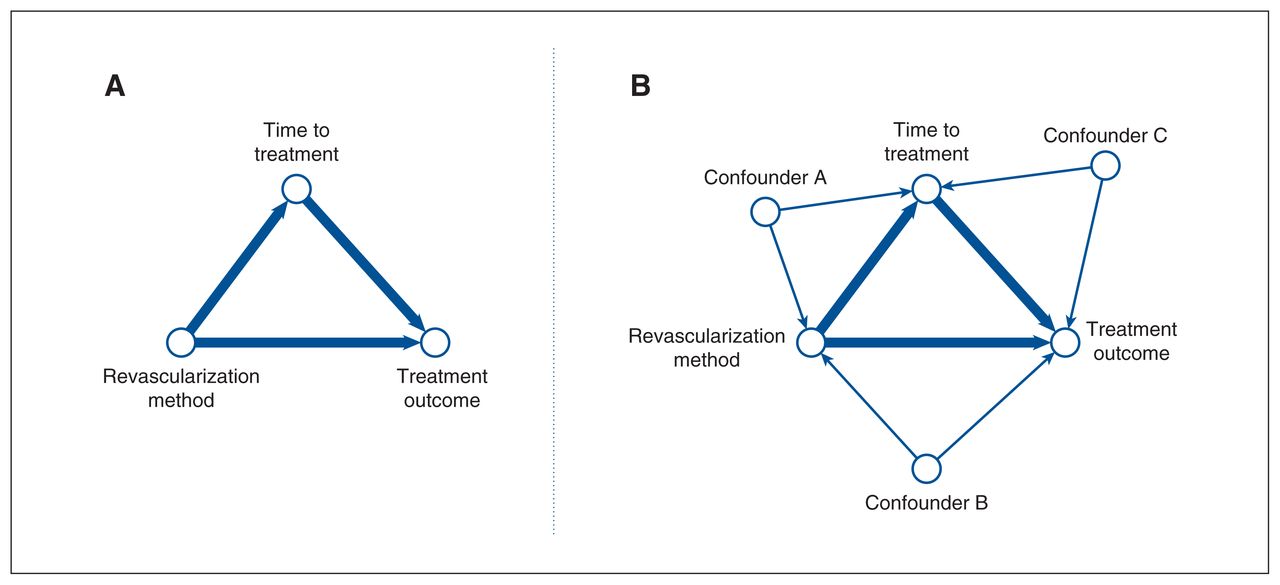
Basic mediation diagram (A): The total effect of the revascularization method on treatment outcome is produced through direct influence and through influence on timing of treatment, which in turn may influence outcomes. The revascularization methods have differential capacity for preventing cardiac events, and the choice of revascularization method determines the time to treatment, which is typically longer for coronary artery bypass grafting than for percutaneous coronary intervention; extended delays to initial treatment increase disease severity and lead to incomplete revascularization. Confounded mediation diagram (B): Confounders for treatment-outcome, treatment-timing and timing-outcome associations.
Study population
Patients with complex disease will be included in the study if the following conditions are met: patient underwent a first-time, nonurgent isolated CABG or single-session PCI procedure for multivessel or left main coronary artery disease; patient did not present with an acute coronary syndrome; clinical and treatment data for the patient were available in a dedicated, population-based registry; and patient survived the index revascularization. We define complex disease as considerable narrowing in the left main stem, with or without involvement of coronary arteries; in each of the 3 major coronary arteries (left anterior descending, left circumflex and right coronary); or, in 2 of the 3 major coronary arteries, with or without involvement of the proximal left anterior descending artery.7
A recent trial showed that only 60% of patients with previously untreated multivessel or left main disease were anatomically and clinically suitable for both PCI and CABG.22 Among the remaining 40%, some were suitable only for CABG because of high anatomic complexity, and the remainder were suitable only for PCI because of high operative risks. Therefore, we have excluded patients with complex anatomy from our study population, based on the score from the TAXUS Drug-Eluting Stent Versus Coronary Artery Bypass Surgery for the Treatment of Narrowed Arteries study, and patients with high operative risks, based on the Society of Thoracic Surgeons score.7 Patients undergoing staged PCI will also be excluded, to avoid misclassification with repeat revascularization.
We identified a study cohort of about 38 000 patients who would be available from a provincial patient registry for a 16-year period: 21 000 patients having PCI and 17 000 patients having CABG (Appendix 1, available at www.cmajopen.ca/content/10/4/E1052/suppl/DC1).
Data sources
We plan to use a population-based patient registry that records the times to treatment as they occurred naturally in cardiac care delivery in BC. The Cardiac Services BC registry12 captures information on all advanced cardiac procedures in the province, including diagnostic coronary angiography, PCI and cardiothoracic surgery.12 The registry contains information on patient characteristics, risk factors, urgency of revascularization, details of procedures, care setting and the dates of care process such as for diagnostic catheterization, booking request and the procedure itself at the point of care (Appendix 2, available at www.cmajopen.ca/content/10/4/E1052/suppl/DC1).
Death and major cardiac events are obtained by linkage to the Vital Statistics and Discharge Abstract Databases held by Population Data BC. The registry applies a validated and shared data merging methodology (to provincial administrative health data) to fill any missing data fields for clinical variables collected at the time of cardiac procedures.23,24
Outcomes and variables
Outcomes
We will use the standard set of long-term outcomes developed by the International Consortium for Health Outcomes Measurement.25 These outcomes include all-cause deaths, heart attack, stroke, heart failure and repeat revascularization during a 5-year period after initial revascularization.
Interventions
Three hypothetical scenarios related to the method and timing of revascularization define interventions as single-stage PCI with natural PCI timing, isolated CABG with natural CABG timing, and isolated CABG but with natural PCI timing. In the context of policy-making, the latter scenario can be arranged using appropriate resource allocation and scheduling guidelines. In the mediation analysis, we will create such a scenario by allowing the time to treatment to take on a natural value for PCI.
Mediator
The mediator (i.e., the time to treatment) will be the number of weeks between the date of the treatment decision and the treatment date. The booking request date will be used as a proxy for the treatment decision date. Our choice of time unit was guided by the rate of residual disease progression, whereby another atherosclerotic narrowing of a coronary artery may occur within several weeks of the initial revascularization.26,27
Statistical analysis
Mediation analysis
We propose to use causal mediation analysis to investigate how time to treatment might affect differences in outcomes between CABG and PCI.28 The purpose of mediation analysis is to partition the total effect of a treatment choice into the effect from solely the treatment method (direct effect) and the effect from treatment-induced timing (indirect effect) (Box 3).29 This partitioning will allow us to estimate the portion of the total effect attributable to the time to revascularization. This measure shows what would happen to the effect of choosing CABG if policy-makers were to remove its influence on time to treatment.
Partitioning the total effect of choosing CABG over PCI into natural direct and indirect effects29
E{Y1M1}: the average outcome after CABG with CABG timing
E{Y1M0}: the average outcome after CABG with PCI timing
E{Y0M0}: the average outcome after PCI with PCI timing
Total effect = E{Y1M1} – E{Y0M0} = E{Y1M1} – E{Y1M0} – E{Y0M0} + E{Y1M0}
Indirect effect = E{Y1M1} – E{Y1M0}
Direct effect = E{Y1M0} – E{Y0M0}
Note: CABG = coronary artery bypass grafting, PCI = percutaneous coronary intervention.
Similar to Weintraub and colleagues21 we aim to determine the outcomes that would be expected if all patients underwent PCI and if all patients underwent CABG within the time frame that naturally arises for each method, that is, not set to a fixed value by a randomized experiment. Then we pose a question: “What would be the outcomes of choosing CABG instead of PCI if the choice of treatment method had no influence on the time to treatment?” We are seeking to determine the difference in outcomes that would be expected if all patients were to undergo PCI and if all patients were to undergo CABG, both within the time to treatment typical for PCI.
Fundamental to this reasoning is the concept of the naturally occurring time to treatment. The time to treatment varies from patient to patient, influenced by factors both related and unrelated to the method of revascularization, which may also cause differences in the comparative effectiveness of the 2 treatments. We consider a counterfactual scenario in which all factors determining the time to revascularization with PCI remain in place, meaning the time to CABG would be the same if PCI had been chosen. We assume that the choice of revascularization method is not driven by the availability of resources between the surgical and catheterization services.
Effect measures
The effect measures of mediation analysis will be obtained using the Neyman model of potential outcomes of hypothetical interventions.29 We will estimate the total effect of CABG compared with PCI as the absolute risk difference in outcomes if all patients undergo CABG or PCI within the time to treatment typical for these procedures (Table 1). We will estimate the natural indirect effect of choosing CABG as the risk difference in outcomes if all patients undergo CABG within the time to treatment typical for CABG and within the time to treatment typical for PCI. We will estimate the natural direct effect of choosing CABG as the risk difference in outcomes if all patients undergo CABG and PCI within the time to treatment typical for PCI. Differences in outcomes will be reported as differences in marginal cumulative proportions measured using a cumulative incidence function to account for time to event and competing risk data.
The effect measures of mediation analysis
Adjustment variables
Causal attribution of variation in outcomes to changes in treatment and mediator could be achieved by conditioning on the factors that are sufficient to block all influences that may produce the treatment-outcome, treatment-mediator and mediator-outcome associations in the absence of causation (Figure 1). In this context, conditioning refers to stratification according to combinations of pretreatment factors, that is, factors observed before the treatment choice, and examination of the treatment-outcome association at different values of observed times to treatment in every stratum separately. We will use a set of pretreatment variables minimally necessary for adjustment using a causal diagram30 (Appendix 3, available at www.cmajopen.ca/content/10/4/E1052/suppl/DC1).
Should the effect of revascularization method truly vary with timing, we would be able to estimate the natural direct effect by stratifying confounders of the method-timing association and taking a population average of effects observed within each stratum over observed times to treatment.31
Sample size
We anticipate a study cohort of about 38 000 patients: 21 000 patients having PCI and 17 000 patients having CABG, (Appendix 1). Serruys and colleagues32 reported that the 1-year proportions of patients who had repeat revascularization, stroke, myocardial infarction or death from any cause were 5.9%, 2.2%, 3.3% and 3.5%, respectively, after CABG, and 13.5%, 0.6%, 4.8% and 4.4%, respectively, after PCI. We assume that these proportions would be higher at 5 years. Using these figures, we project a total of 3838 repeat revascularizations, 500 strokes, 1569 myocardial infarctions, and 1519 deaths from any cause in our study.
Sufficient numbers of patients and events are available for developing a model for predicting the risks of repeat revascularization, stroke, myocardial infarction and death from any cause in this population-based study. Sample size requirements are derived from the outcome proportion, the number of events relative to the number of predictor parameters and the expected predictive performance of the model.33 We assume the above-mentioned 1-year outcome proportions. The maximum number of predictor parameters is assumed to be 25, given our experience with the number of variables in a minimal adjustment set. We assume that the model will explain 15% of the maximum variability as measured by the R2 statistic.33 Given these assumptions, we would need about 2997 patients with 303 repeat revascularizations, 11 349 patients with 150 strokes, 5027 patients with 208 myocardial infarctions and 5134 patients with 206 deaths. This corresponds to about 12, 6, 8, and 8 events per predictor parameter in the respective models. Sample size calculations were performed using the pmsampsize package for R statistical software (version 4.0.4; R Foundation for Statistical Computing).
Ethics approval
This study has been approved by the University of British Columbia Clinical Research Ethics Board (UBC CREB H17-00505).
Interpretation
Using the conceptual framework for an observational study described in this methodology paper, we are seeking to assess treatment outcomes under various scenarios of revascularization method and timing as if they had been implemented for the same patient population. We will use mediation analysis to distinguish between the effect of choosing CABG and the effect of its timing, by contrasting CABG and PCI outcomes when both treatments are performed within the time typical for PCI. Replacing CABG-induced times with PCI-induced times is not equivalent to setting the times to treatment by means of a randomized experiment.20,34 Following Robins and Greenland,27 we submit that randomization of patients to various combinations of treatment method and treatment timing would fail to distinguish the effect of choosing CABG from the effect of treatment timing induced by this choice. Instead, we will deactivate the influence of the revascularization method on time to treatment through mediation analysis.
Determining the appropriate treatment for patients with stable multivessel and left main disease when the cardiac anatomy is suitable for either CABG or PCI is a complex decision process. 1 Recent guidelines stratify the appropriateness of the revascularization method according to anatomic complexity, risk of postoperative mortality, presence or absence of diabetes, presence or absence of left main disease and severe left ventricular systolic dysfunction.5,7 However, Head and colleagues35 have argued that other contributing factors, such as local expertise and patient preference, could favour a particular revascularization method.35 In health systems where budgetary considerations may delay patients’ planned treatments,19 the time to treatment is a factor that has not been studied in the context of comparative treatment effectiveness.14 However, there is a strong argument that doctors have a duty to inform their patients of the expected delays and the associated risks when choosing between treatments.36
Our projections will quantify the effect of changes in time to treatment for CABG on differences between CABG and PCI outcomes. We will obtain effect measures of mediation analysis: the total effect, the natural indirect effect and the natural direct effect. The total effect will show the difference in outcomes between PCI and CABG produced through direct influence of the treatment method and through influencing the time to treatment, which in turn may influence outcomes. The indirect effect will show the difference in outcomes that is attributable to timing and the direct effect will show the difference in outcomes that is attributable solely to the chosen method. The partitioning of the total effect will further allow us to estimate the proportional reduction in the risk of an outcome if the time to CABG was similar to PCI.
Understanding the extent to which time to treatment mediates the relation between method of revascularization and outcome will have implications for treatment selection, resource allocation and planning benchmarks.
Limitations
We use administrative data known to underreport comorbidity. 37 Comorbidity is an important confounder as it can affect timing of treatment and in-hospital death owing to the increased risk of complications. The study population includes only patients who had treatment; therefore, our analysis does not consider events that occurred before treatment can be given.38 We are examining delays that occurred after the booking request was submitted because the date of treatment decision is not in the data set. This can lead to misclassification of mediator values. Finally, we use the evidence-informed causal diagram to select adjustment variables.39 However, this diagram reflects only existing knowledge and may omit the unknown relations between pretreatment factors that may influence treatment-outcome, treatment-mediator and mediator-outcome associations.
Conclusion
The choice of treatment for patients with an indication for coronary revascularization is routinely made without robust evidence about the effect of treatment timing. We offer a conceptual framework of mediation analysis for estimating the extent to which changes in time to treatment may affect the difference in outcomes between CABG and PCI. The findings on benefits and risks of performing revascularization within a certain time will guide multidisciplinary teams in determining whether PCI or CABG is the appropriate method for individual patients.
Acknowledgements
The authors wish to thank Guy Fradet, MD, and Simon Robinson, MD, for useful discussions of ideas; Peggy Robinson, ELS, for presubmission assistance with the manuscript and Sean Hardiman for literature search assistance.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Boris Sobolev and Lisa Kuramoto contributed to the conception and rationale of the study, and to the selection of statistical methodology. Boris Sobolev and Lisa Kuramoto drafted the manuscript and revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This research was funded by the Canadian Institute for Health Research (PJT-159686). This funder had no role in the design of this study, execution, analyses, data interpretation or decision to submit results for publication.
Data sharing: There are no data to be shared.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/10/4/E1052/suppl/DC1
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use) and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2022 CMA Impact Inc. or its licensors
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.