


Abstract
Background: Although clinical empathy — the ability of a physician to understand a patient’s illness experience, communicate this understanding and act collaboratively to create a treatment plan — provides substantial benefits to both physicians and patients, medical students typically experience a decline in empathy during training. The primary objective of this study was to generate a model of clinical empathy grounded in the perspectives of people with chronic illness living in Canada, to promote empathy-focused curricular development in Canadian medical education.
Methods: We conducted a qualitative focus group study using a constructivist grounded theory approach. We recruited adults (age ≥ 18 yr) with chronic illness who had recently seen a physician in Canada from virtual support groups. Six semistructured virtual focus groups with 3–5 participants each were scheduled between June and September 2021. We coded the transcripts using the constant comparative method, allowing for the construction of an overarching theory.
Results: Twenty patients (17 women and 3 men) participated in the focus groups; 1 group had 2 participants because 1 participant failed to appear. The majority of participants (14 [70%]) had at least a college degree. The mean rating for overall satisfaction with the Canadian health care system was 5.4/10.0 (median 5.0). The emergent theory showed that the perceived presence of physician empathy engendered positive internal processing by patients, leading to increased health care efficacy and enhanced mental health outcomes. Negative patient processing in response to the perceived absence of empathy led to reduced quality of health care delivery (e.g., ineffective referrals and more appointments), increased use of health care resources, disruptions in patients’ personal lives, and negative physical and mental health outcomes.
Interpretation: Clinical empathy can have life-altering impacts on patients, and its absence may increase resource use. As empathy involves understanding patients’ lived experiences, any valid intervention to improve clinical empathy must be informed by patient perspectives.
The physician–patient relationship is a key contributor to the quality of health care, with physician empathy benefiting patients and physicians alike.1 The construct of empathy has multiple components, namely, affective (experiencing others’ emotions), cognitive (understanding others’ feelings) and behavioural (communicating understanding), with the last 2 being most important in clinical scenarios.2,3 Clinical empathy can thus be defined as the physician’s ability to understand the patient’s illness experience, communicate this understanding and act on it to create a collaborative treatment plan with the patient.3–7
Empathetic care can improve patient mental health outcomes and coping,5,8,9 as well as physical health outcomes.6,10 Furthermore, empathetic care may promote patient understanding of and confidence in their care plans, increasing adherence and reducing the perceived need for additional referrals and interventions.7,9 From the physician’s perspective, higher patient-rated physician empathy scores are associated with reduced burnout,3,11–13 lower risk of litigation14 and improved resource stewardship.15
Despite the clear benefits of empathy to both physicians and patients, medical students experience a decline in empathy throughout training.1,16 Various interventions have been attempted to mitigate this, including written reflections, dramatizations of clinical scenarios and interpersonal skills training.17 However, there is no consensus on the efficacy of these interventions, and their development has largely lacked systematic input from patients with lived experiences. Patient partnerships are increasingly recognized as central to designing health care interventions, and already feature prominently in research design, health policy and medical education in other countries.16,18,19 Studies examining patient experiences of clinical empathy have also been primarily restricted to specific illness contexts.20–22 However, we hypothesize that patients’ experiences of clinical empathy are not unique to particular diagnoses and that it is these universal factors that are the most useful in informing undergraduate medical education, since they are relevant to all future clinicians. Furthermore, data on clinical empathy in biomedicine have largely been drawn from the United States and United Kingdom;16,23 given that patient experiences are highly unique within each health care system, we aimed to develop findings specifically applicable to the Canadian health care system.
The primary objective of the present study was to generate a novel theoretical model of clinical empathy grounded in the perspectives of patients with a variety of chronic illnesses receiving health care in Canada. The study was part of a larger project that aims to promote clinical empathy training in Canadian medical education. This involved elucidating how patients with chronic illness characterize clinical empathy, their experiences of empathy from physicians in Canada, and subsequent impacts on their health and quality of life. The secondary objective of the present study was to collect patient recommendations on how medical education can be improved to address deficits in empathy.
Methods
Design
This was a virtual, focus group–based qualitative study conducted using Charmaz’s constructivist grounded theory methodology. 24 Grounded theory is an iterative methodology characterized by minimal preconception of results, which permits the generation of a theory grounded in participants’ lived experiences.25 Constructivist grounded theory views the theory as a construct resulting from the interplay of researchers with research participants.24,26
This study is part of the Empathy in Medical Professionals: Augmenting Curriculum and Training (EMPACT) project, a student-led initiative that seeks to amplify the voices of patients in Canada and inform innovation in medical education.
Population and recruitment
Recruitment was open to residents of all provinces and territories. Participants were recruited from virtual support groups for patients with chronic illness in Canada (general chronic illness/disability or any of the 10 most prevalent chronic diseases according to the Public Health Agency of Canada27) (Appendix 1, available at www.cmajopen.ca/content/11/5/E859/suppl/DC1). We selected this population because patients with chronic illness are major users of health care services and typically have experiences with multiple physicians. 28,29 We chose Facebook as the primary recruitment platform given its large and diverse user base, accessibility to patients who may be housebound and prevalent use by people with chronic illness.30–33 Owing to a paucity of male participants, promotion was expanded to the Prostate Cancer Support Canada e-newsletter.
Volunteers completed a screening survey and were included if they were at least 18 years of age, were English-speaking, self-identified as having a chronic illness for at least 24 months, used the Canadian health care system as their primary source of medical care and had had an appointment with a physician in Canada in the previous 12 months. The end point for recruitment corresponded to the point of theoretical saturation (i.e., the point at which no new themes that contributed meaningfully to the theory being constructed were identified from newly collected data).24
Study procedures were explained to interested participants over the telephone, and consent was obtained verbally and by electronic signature before enrolment.
Data collection
All participants completed an anonymous questionnaire that captured demographic information and overall satisfaction with the Canadian health care system (Appendix 2, available at www.cmajopen.ca/content/11/5/E859/suppl/DC1).
We developed a semistructured focus group interview guide (Appendix 3, available at www.cmajopen.ca/content/11/5/E859/suppl/DC1) based on our study objectives and literature. The guide questions were piloted with a group of 4 first-year medical students for rehearsal and assessment of clarity of the questions; we modified the questions based on their feedback. In addition, during and after each focus group, participants were given opportunities to provide verbal feedback and anonymous written feedback about any elements of the focus group, including guiding questions; all feedback was incorporated into subsequent groups. General prompting phrases such as “Would you like to elaborate on that?” were used at the moderator’s discretion. We modified, reordered or reworded questions as appropriate based on participants’ feedback.
Six 90-minute focus groups with 3–5 participants each were scheduled. Focus groups were conducted via Zoom by 2 members of the study team (S.G., I.C.E., S.P., A.L. and/or M.M.: 1 followed the guide while allowing participants to steer the discussion as appropriate, and the other asked follow-up questions and took reflective notes for memoing and triangulation purposes. S.G. comoderated every group to ensure consistency. The definition of clinical empathy was explained to participants verbally and in writing, and was revisited frequently throughout the focus group. To reduce the influence of participants’ pre-existing definitions of this construct, the word “empathy” was not used by the moderators. Focus groups were recorded with participant consent and transcribed verbatim by 2 undergraduate student volunteers.
Data analysis
Iterative coding was performed concurrently with data collection. Initial line-by-line coding of transcripts by means of the constant comparative method24 was done independently by M.M. and S.P., who subsequently conferred to reach consensus on common themes. Theoretical saturation was reached after 6 focus group transcripts had been coded. Codes were verified with the live interview notes. Member-checking was done by sending descriptions of the codes derived from each transcript to the participants of the corresponding focus group for feedback (Appendix 4, available at www.cmajopen.ca/content/11/5/E859/suppl/DC1), which was subsequently incorporated into the data.
During focused coding, we prioritized codes based on relevance to the emerging theory and grouped them into categories, using constant comparison throughout.24 S.G. reviewed individual quotations that corresponded to each code to determine subthemes within codes (deductive analysis) and compared them to determine multidirectional linkages between codes (inductive analysis); several new codes were obtained in this process. S.G. then implemented axial coding through a constructivist lens,24 using mind-mapping software (MindMeister, MeisterLabs) to visually represent linkages between subcategories, as well as through written reflections on each category. The associations that emerged facilitated construction of an overarching model of the impacts of clinical empathy on patients with chronic illness receiving health care in Canada.
Reflexivity
The research team comprised 6 first-year medical students (S.G., I.C.E., S.P., A.L., M.M., I.S.) and 2 supervising professors (J.S., C.W.). Both supervisors had extensive experience with the design, performance and supervision of qualitative research including grounded theory, and 5 students had previous experience performing qualitative research. All 4 team members who comoderated focus groups had completed training on focus group moderation, and 2 had previous experience conducting individual or group interviews. Four students on the research team identified as patients with chronic illness in addition to their developing identities as health care professionals. We consulted 1 patient partner with experience in patient advocacy and patient-led medical education for input on study objectives and methodology.
We engaged in a variety of reflexivity practices to enhance the rigour and trustworthiness of our findings. Regular reflective conversations were conducted among members of the study team throughout study design and analysis, and after each focus group. Detailed memoing24 was performed throughout analysis and was reviewed with other team members. In addition to member-checking by patients, team members verified codes, categories and concepts in a process of investigator triangulation. To avoid projection of researcher-assumed phenomena, we included mapped linkages during axial coding only in cases in which participants explicitly described connections.
Ethics approval
This study was approved by the Hamilton Integrated Research Ethics Board (no. 12912).
Results
Twenty patients participated across the 6 focus groups; 1 group contained only 2 participants because the third participant failed to appear. Participant demographic characteristics are summarized in Table 1. Participants’ diagnoses were not formally elicited, but diagnoses that were voluntarily mentioned included rheumatoid arthritis, asthma, cancer and fibromyalgia. Participants rated their overall satisfaction with the Canadian health care system as a mean of 5.4/10.0 (median 5.0).
Demographic characteristics of focus group participants
Clinical empathy model
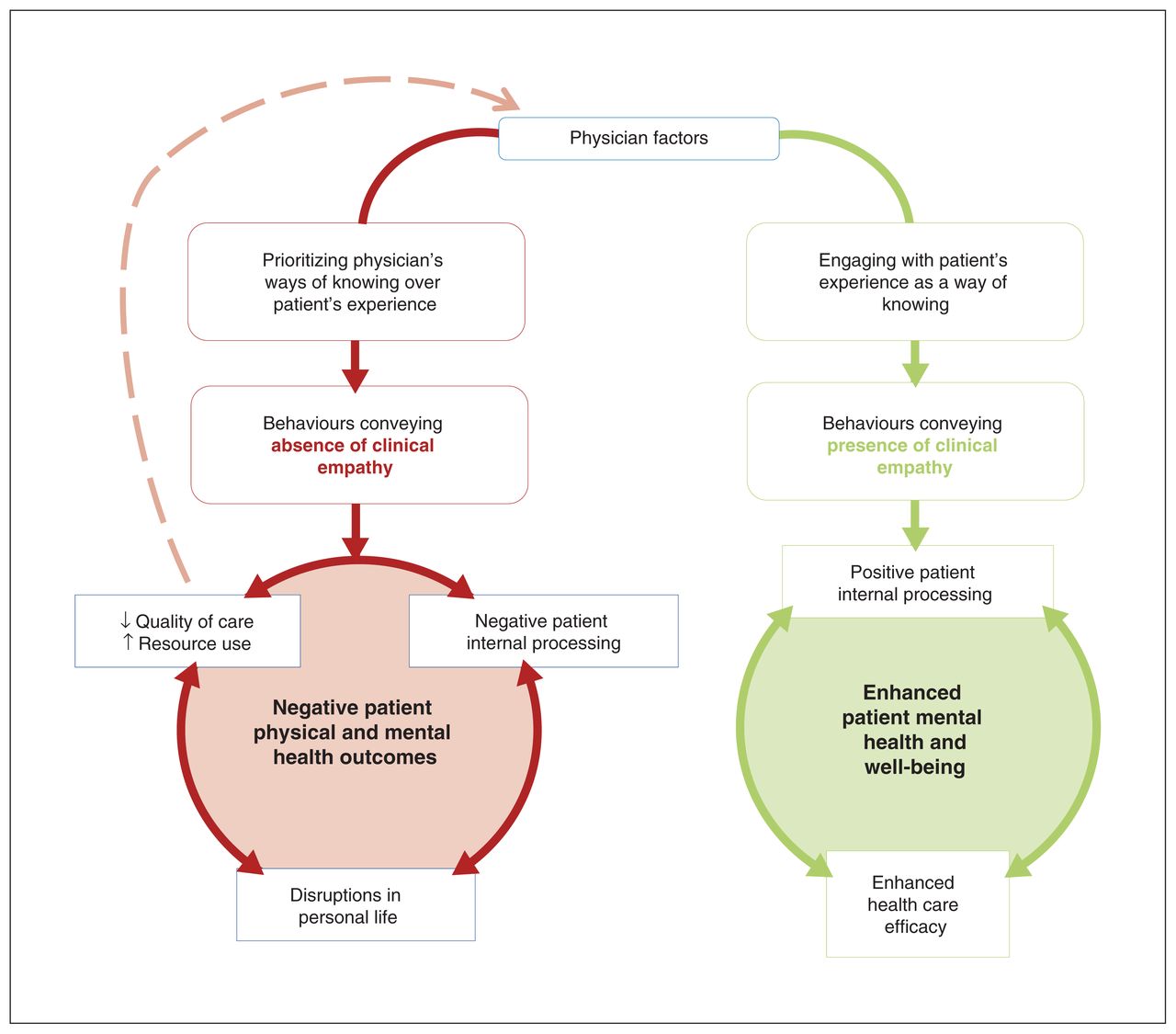
Primary concepts that emerged during analysis are presented in Table 2 and Table 3, together with illustrative quotations. Further details regarding patient-perceived phenomena are presented in Appendix 5 (available at www.cmajopen.ca/content/11/5/E859/suppl/DC1). The theory abstracted from these concepts is depicted in Figure 1.
Components of the patient-derived clinical empathy model corresponding to the absence or deficiency of clinical empathy, and illustrative quotations
Components of the patient-derived clinical empathy model corresponding to the presence of clinical empathy, and illustrative quotations

Model of patient-perceived clinical empathy and its downstream effects on health care delivery and patient outcomes when absent or present. Note that many physician–patient interactions combine elements of both sides of the model.
Participants postulated that internal factors (burnout, biases) and external factors (setting, specialty, patient load, ableist culture of medicine) predisposed physicians to interact with them with a lack of trust and understanding. This was thought to manifest in a failure to display supportive behaviours or even in antagonistic behaviours such as name-calling and patient-blaming. Participants processed these experiences in ways that reduced their trust in physicians and the health care system, and compromised their self-image. Ripple effects affected elements of their personal lives, including work and family relationships (Figure 1).
These processes were also interrelated with decreased quality of health care delivery despite increasing resource use (e.g., ineffective referrals and more appointments). For instance, nonempathetic care made participants more likely to delay seeking care until they were severely ill owing to fears of retraumatization, and promoted nonadherence to prescribed treatment regimens. These outcomes amplified the preexisting factors inhibiting physician empathy by increasing the use of health care services and physician frustration.
Impacts on patient cognition, personal life and health care formed a vicious cycle that contributed to negative physical and mental health outcomes. Mental health was a dominant theme, with participants describing exhaustion, hopelessness, helplessness, anxiety, depression and suicidal ideation as downstream effects of a deficiency of clinical empathy.
Participants believed that factors such as having had a patient-centred medical education, and adequate support and resources allowed physicians to engage with patients’ experiences in ways that displayed clinical empathy (Figure 1). Empathetic behaviours included listening, honest and supportive communication, and collaborative formulation of a care plan. This engendered a positive internal response in patients, characterized by feelings of hope and empowerment, and trust in their physicians and treatment plans, which promoted a cycle of improved treatment adherence and more effective resource use. Participants said that the hope provided by physician validation was the most crucial thing for patients living with chronic illness: with this, patients felt motivated to self-manage their health via lifestyle improvements, adherence to treatment, appropriate consumption of health care services and self-education. Overall, the downstream effects of clinical empathy enhanced participants’ health and well-being by improving their self-image and self-efficacy, mental health, and perception of symptoms and pain.
Recommendations for medical education
Participants shared suggestions on changes to medical school admission and training that they believed could improve clinical empathy (Table 4). They also acknowledged that supporting physicians’ mental health and mitigating burnout are essential for any intervention to have a sustainable impact.
Participant recommendations for medical education to improve clinical empathy in future physicians
Interpretation
Patients with chronic illness perceived the presence and absence of clinical empathy as initiators of positive or negative health outcome cycles, respectively. Some outcomes were seen to be mediated by the impact of empathy on treatment and the disease course, but others were described as direct, independent consequences of clinical empathy.
Congruent with previous evidence,34–36 physician doubt and dismissal had negative impacts on patients’ self-worth, identities and mental health. There is evidence that personalized invalidation by physicians increases patient depression, mediated by reduced self-esteem.36 Physician disbelief of patient symptoms can erode patients’ senses of reality and themselves, which many patients perceive as mental manipulation or “gaslighting.”37,38 It has been suggested that physician-induced “medical posttraumatic stress” may be a strong contributor to anxiety during medical encounters independent of trauma from illness itself.34
Although we report patients’ experiences of the presence and absence of clinical empathy discretely in this study, real clinical interactions are more likely to involve a mix of the negative and positive phenomena identified in Table 2 and Table 3, respectively. Whereas many positive experiences may be required to rebuild medical trust, a single negative experience can cause substantial regression to a position of fear and insecurity.34 Our findings suggest that anxiety born from negative experiences is often generalized to systems and other physicians, whereas positive experiences build trust only in the enacting physician. Moreover, the relative authority of physicians makes patients’ confidence in self-assessment particularly vulnerable to damage from even small expressions of physician doubt and increases the likelihood of resultant depression.35,39 Comorbid physical and mental illness is associated with significantly higher use of health care resources,40,41 and, in the present study, clinical empathy had a strong perceived link to mental health in patients with physical illnesses; thus, enhancing clinical empathy may be an important target for reducing health care burden as it has no financial cost, need not require substantially more time per visit,42 and may even save time by minimizing miscommunication and repeated appointments.
Our participants agreed that clinical empathy should be an essential component of medical school training and suggested increasing patient involvement in medical education, a strategy that was shown to enhance student empathy and knowledge in a recent systematic review.16 Our participants also suggested that admission of more students with personal illness experiences may foster better understanding of patients with chronic illness.43,44 Currently, medical students with chronic illness and disability are frequently undersupported and excluded from medical training.45 First steps would be including patients in the development and implementation of medical school curricula, and increasing the accessibility of the medical field to students with medical conditions.43,46 In future phases of the EMPACT project, data will be collected from Canadian medical schools and medical students to characterize current clinical empathy training in Canada and inform the development of improved educational interventions. All this must be done with recognition and confrontation of the systems that disempower physicians from displaying clinical empathy, such as a strained health care system that produces physician burnout.47,48
Limitations
Participants in this study were self-selected members of illness support groups. The use of social media to find and share health information in such groups is associated with higher levels of education and female gender.33 This may explain why, despite researcher attempts to increase sample diversity, the study sample consisted primarily of women with postsecondary education. All participants required access to a device with Internet, most lived in urban areas, only 20% self-identified as being a member of a visible minority, and none identified as Indigenous. As discrimination was commonly identified as a barrier to clinical empathy by our participants, it is likely that marginalized populations would face the issues described by participants to an even greater extent, in addition to unique barriers such as those related to race, ethnicity, gender, sexual orientation or socioeconomic status. Future studies in other patient groups are needed to explore these differences.
Conclusion
Our findings show that the absence of clinical empathy on the part of physicians may cause considerable harm to patients with chronic illness and may increase use of health care resources. The knowledge that clinical interactions can affect a patient’s health, self-concept and quality of life should be treated with the same responsibility as any other medical intervention. As empathy involves understanding patients’ lived experiences, any valid intervention to improve clinical empathy must be informed by patient perspectives.
Acknowledgements
The authors thank Ophira Calof for providing a patient perspective on the study objectives and design, Aurgho Datta and Gerry Huynh for their hard work transcribing focus group recordings, Ally Hoffman, Emiliyan Staykov, Emily Au and Erin Vink for participating in the pilot focus group and offering feedback, Sarah Klapman for editing a previous version of the manuscript and Sabrina Rioux for designing the beautiful EMPACT logo.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Shira Gertsman conceived the study. All of the authors designed the study. Shira Gertsman, Ioana Cezara Ene, Sasha Palmert, Amy Liu and Mallika Makkar acquired the data, and Shira Gertsman, Ioana Cezara Ene, Sasha Palmert, Amy Liu, Mallika Makkar, Johanna Shapiro and Connie Williams analyzed the data. Shira Gertsman interpreted the data and drafted the manuscript, with contributions from Ioana Cezara Ene and Sasha Palmert. All of the authors revised the manuscript critically for important intellectual content, approved the final version to be published and agreed to be accountable for all aspects of the work.
Funding: This work was funded by a McMaster Medical Student Research Excellence Scholarship.
Data sharing: To ensure participant confidentiality, full focus group transcripts are not publicly available. Deidentified codes with applicable quotations are available from the corresponding author on reasonable request.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/5/E859/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.