


Abstract
Background: Medical assistance in dying (MAiD) was legalized in Canada in 2016, with legislation updated in 2021. It is unclear whether resources are available to help patients make this difficult decision; therefore, we sought to identify and quality appraise Canadian MAiD resources for supporting patients making this decision.
Methods: We conducted an environmental scan by searching Canadian websites for online MAiD resources that were published after the 2016 MAiD legislation, patient targeted, publicly accessible and able to inform decisions about MAiD in Canada. We excluded resources that targeted health care professionals or policy-makers, service protocols and personal narratives. Two authors appraised resources using the International Patient Decision Aids Standards (IPDAS) criteria and the Patient Education Materials Assessment Tool (PEMAT) for health literacy. Descriptive analysis was conducted. We defined resources as patient decision aids if 7 IPDAS defining criteria were met, and we rated resources as adequate for understandability or actionability if the PEMAT score was 70% or greater.
Results: We identified 80 MAiD resources. As of March 2023, 62 resources (90%) provided eligibility according to the 2021 legislation and 11 did not discuss any eligibility criteria. The median IPDAS score was 3 out of 7; 52% discussed alternative options and none provided benefits or harms. Of 80 resources, 59% were adequate for understandability and 29% were adequate for actionability.
Interpretation: Although many resources on MAiD were updated with 2021 legislation, few were adequate to support patients with lower health literacy. There is a need to determine whether a patient decision aid would be appropriate for people in Canada considering MAiD.
Never have people in Canada been confronted with so many difficult decisions, including those who are the most vulnerable owing to serious illnesses negatively influencing their length of life and/or quality of life. In February 2015, the Supreme Court of Canada ruled (Carter v. Canada) that parts of the Criminal Code would need to change to satisfy the Canadian Charter of Rights and Freedoms and that parts of the Criminal Code that prohibit medical assistance in dying (MAiD) would no longer be valid.1 Responding to the Supreme Court’s call for a new law, the Canadian government legalized MAiD (Bill C-14) in June 2016 to allow for the safe and intentional end of life of patients suffering from grievous, incurable diseases and whose death is reasonably foreseeable.1 In March 2021, Bill C-7 broadened the eligibility criteria for MAiD to include patients whose death is not reasonably foreseeable, but this requires a 90-day waiting period.2 MAiD involves the administration of medications to safely and intentionally end the life of an adult who was eligible for MAiD and specifically requested it.1
End-of-life decisions, including MAiD, were identified in a recent Canadian survey of difficult decisions.3 According to the MAiD legislation, patients requesting MAiD are expected to receive information about all options available to them.1 However, it is unclear the extent to which Canadians actively making the decision about MAiD are supported in considering alternative end-of-life care options.4 Some people may question if MAiD is an informed, values-congruent choice or if MAiD is chosen because there is inadequate access to palliative care. Patient decision aids are effective evidence-based resources to support patients to participate in making informed values-congruent choices.5 At a minimum, patient decision aids make explicit the decision, provide information on options (including benefits and harms) and help clarify values for outcomes of options.6
Although there are MAiD resources available for people in Canada, it is not clear to what extent they can support decision-making or if they are adequate for people with lower health literacy. Therefore, we sought to identify Canadian MAiD resources for patients and appraise their quality.
Methods
We conducted an environmental scan using online searches following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses reporting guidelines.7 The environmental scan included seeking, gathering and interpreting information to answer the research objective.8–10 Three searches were conducted in August 2021, April 2022 and March 2023. We identified eligible resources by searching the online websites, extracted the data on them, appraised their quality and analyzed findings. The interpretation was informed by the quality appraisal.
Setting
In Canada, there was a total of 31 664 reported MAiD deaths from 2016 to 2021 with year-over-year increases.11 In 2021 alone, MAiD accounted for 3.3% of all deaths, with the highest proportions occurring in Quebec and British Columbia (4.7% and 4.8%, respectively). There were more men who received MAiD (52.3%) than women, and the average age was 76.3 years.11 The most common underlying medical conditions were cancer, cardiovascular conditions, chronic respiratory conditions and neurologic conditions, consistent with leading causes of death in Canada.
Search strategy
We conducted the environmental scan using Google searches and handsearching Canadian government and organization websites. These organization websites were identified in consultation with stakeholders in our professional networks. We did not handsearch websites for Canadian hospitals, long-term care centres or hospices, given the large number of these organizations in Canada.
We limited the search to Canadian websites given that the resources identified would also need to reflect the Canadian MAiD legislation.1 Two authors (A.K. and Q.Z.) independently conducted the searches using popular searched keywords according to Google Trends. Google Trends allows researchers to streamline their search results by selecting the most popular keywords used by the public when looking for information online.12 Multiple keywords were entered in the search bar of Google Trends by one author (A.K.). Google Trends indicated that MAiD was a common topic in Canadian health care from 2020 to 2021, as evidenced by the number of search hits (Figure 1, Figure 2). The output graphs showed a Canadian trend, which could be adjusted by time range. As a result, key terms searched independently were as follows: medical assistance in dying, assisted suicide, voluntary euthanasia, MAiD and dying, and physician assisted suicide. For the March 2023 search, we added “aide médicale à mourir.” We did not use Boolean operators, which are typically used for medical database searches. Our search strategy in 2023 was verified a priori by an academic librarian (L.S.).

Google Trends of keywords graph. Data source: Google Trends.
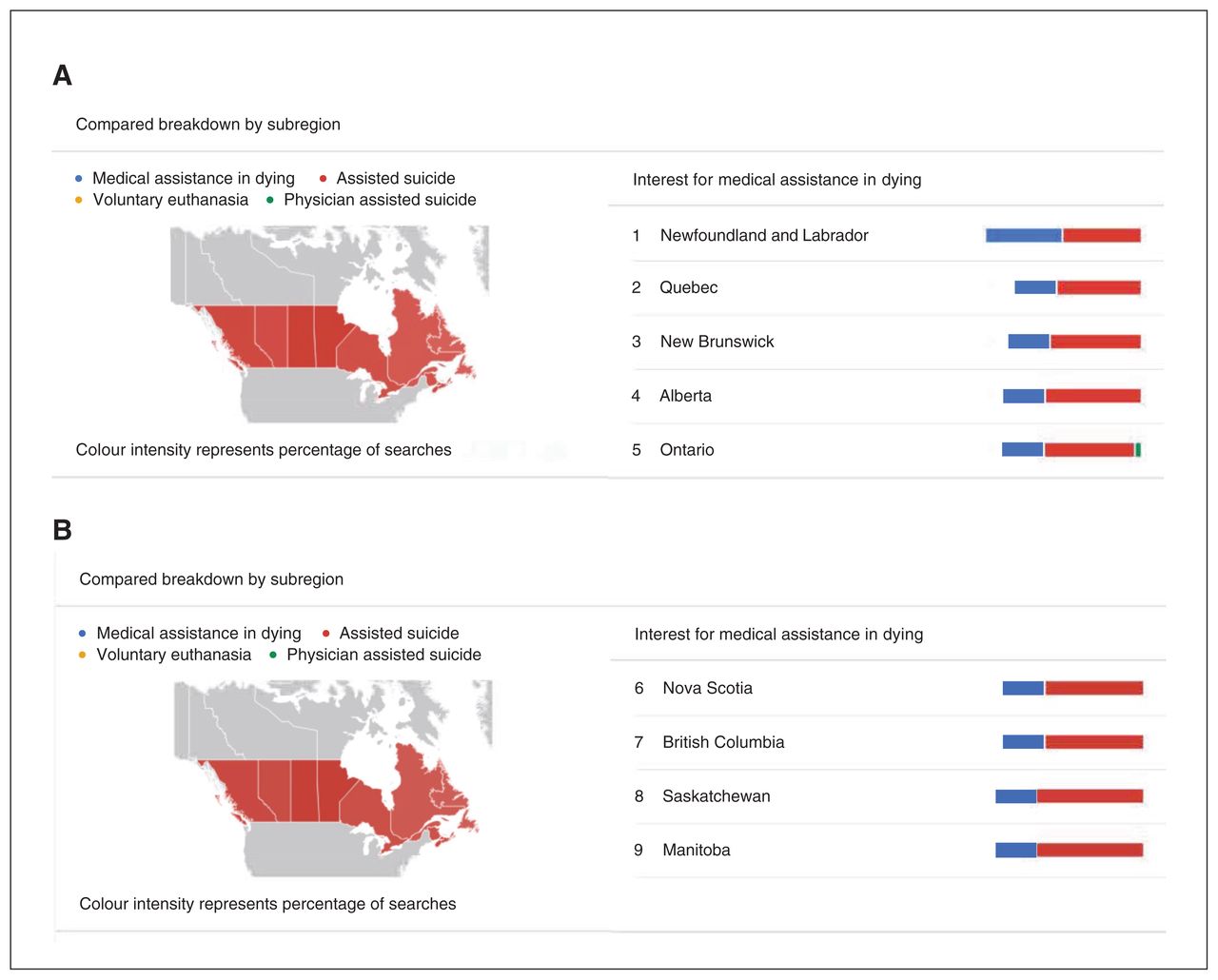
Google Trends of keywords diagram. (A) Google Trends results for keywords of subregions 1–5. (B) Google Trends results for keywords of subregions 6–9. Note: Coloured bars show the prevalence of which search term was used in which subregion. Data source: Google Trends.
We conducted searches in a new private window in the Internet browser Safari to prevent caching of results from previous searches.13 We discontinued the searches when no new resources were identified within the next 50 Internet hits. We searched the Canadian federal, provincial and territorial governments’ websites, as well as relevant Canadian organizations’ websites (i.e., Dying with Dignity Canada and Canadian Association of MAiD Assessors and Providers) using the same search terms. Additionally, we reviewed Google Advanced Search using the same keywords.
Eligibility of resources
Two authors (A.K. and Q.Z.) independently assessed identified MAiD resources for eligibility. Eligible MAiD-focused resources were published after the 2016 MAiD legislation, able to inform decisions about MAiD, patient-targeted and publicly accessible. We determined that a resource could inform decisions if it provided information on MAiD as an end-of-life option, including details about the procedure. Format for eligible resources included printed materials (e.g., web pages and downloadable documents) and video recordings. We excluded resources if they were targeting health care providers or policy-makers, were personal narratives (e.g., personal websites, blogs and public forums) or were health care service protocols (e.g., request forms and instructions for completion of health care providers roles). We documented reasons for exclusion.
Data extraction
We extracted information on eligible resources using a standardized data extraction spreadsheet in Excel Version 16.48 (Microsoft). Two authors (A.K. and Q.Z.) independently extracted the following data: resource title, target audience, author/developer, year of last update, languages in which the resource is available, URL, pathway to the resource and date accessed.
Quality appraisal
Two of 3 authors (A.K., L.P.-B. and Q.Z.) independently appraised the eligible resources. Discrepancies were resolved through consensus or consultation with a third author (D.S.) as necessary. We assessed the accuracy of MAiD information on eligibility criteria through comparison with the 2021 Bill C-7: An Act to Amend the Criminal Code (medical assistance in dying) at 5 months (August 2021), 13 months (April 2022), and 24 months (March 2023) after legislation passed. We scored it as yes (updated), no (not updated) or not applicable if eligibility was not discussed.
We used the 6 International Patient Decision Aids Standards (IPDAS) criteria to determine whether the resource qualified as a patient decision aid.14 We included a seventh criterion of “target audience” as proposed by Martin and colleagues.15 We scored the IPDAS criteria as present (yes) or absent (no).
To assess health literacy, we used the Patient Education Materials Assessment Tool for Printable Materials (PEMATP) or Audiovisual Materials (PEMAT-AV). The PEMAT assesses resources on 2 domains: understandability (PEMATP includes 17 items; PEMAT-AV includes 13 items) and actionability (PEMAT-P includes 7 items; PEMAT-AV includes 4 items).16 We scored the items as 0 (disagree), 1 (agree) or NA (not applicable) according to the PEMAT User’s Guide.16,17 PEMAT scores were calculated as percentages of total possible points (excluding not applicable).16 According to PEMAT, materials are considered understandable when consumers of diverse backgrounds and varying levels of health literacy can process and explain the key messages. Resources were considered actionable when consumers of diverse backgrounds and varying levels of health literacy can identify what actions are possible to take based on the information provided. The PEMAT individual scores were standardized on a scale out of 100.
Data analysis
We used descriptive statistics to report characteristics of the resources. As data were not normally distributed, we analyzed findings using median, interquartile range (IQR) and range. Resources had to meet all 7 criteria to be defined as a patient decision aid.18 An overall score of 70% or greater indicated the resource was adequate for being understandable or actionable.16
Ethics approval
Ethics approval was not required for this environmental scan.
Results
In March 2023, we searched a total of 1666 Web hits on Google, and 80 were eligible to be included (Figure 3). Fifty-two resources were available in English only, 23 in English and French, 5 in French only and 1 (published by Vancouver Coastal Health; resource 29) was available in 6 languages (English, Chinese Traditional, Chinese Simplified, Punjabi, Spanish and Vietnamese). Resources were developed by the federal government (n = 3), national organizations (n = 15), provincial governments (n = 9), provincial health authorities (n = 33), hospitals (n = 16) and territorial governments (n = 4) (Table 1). Of 80 online resources, 75 were available in print and 5 were available as a video.
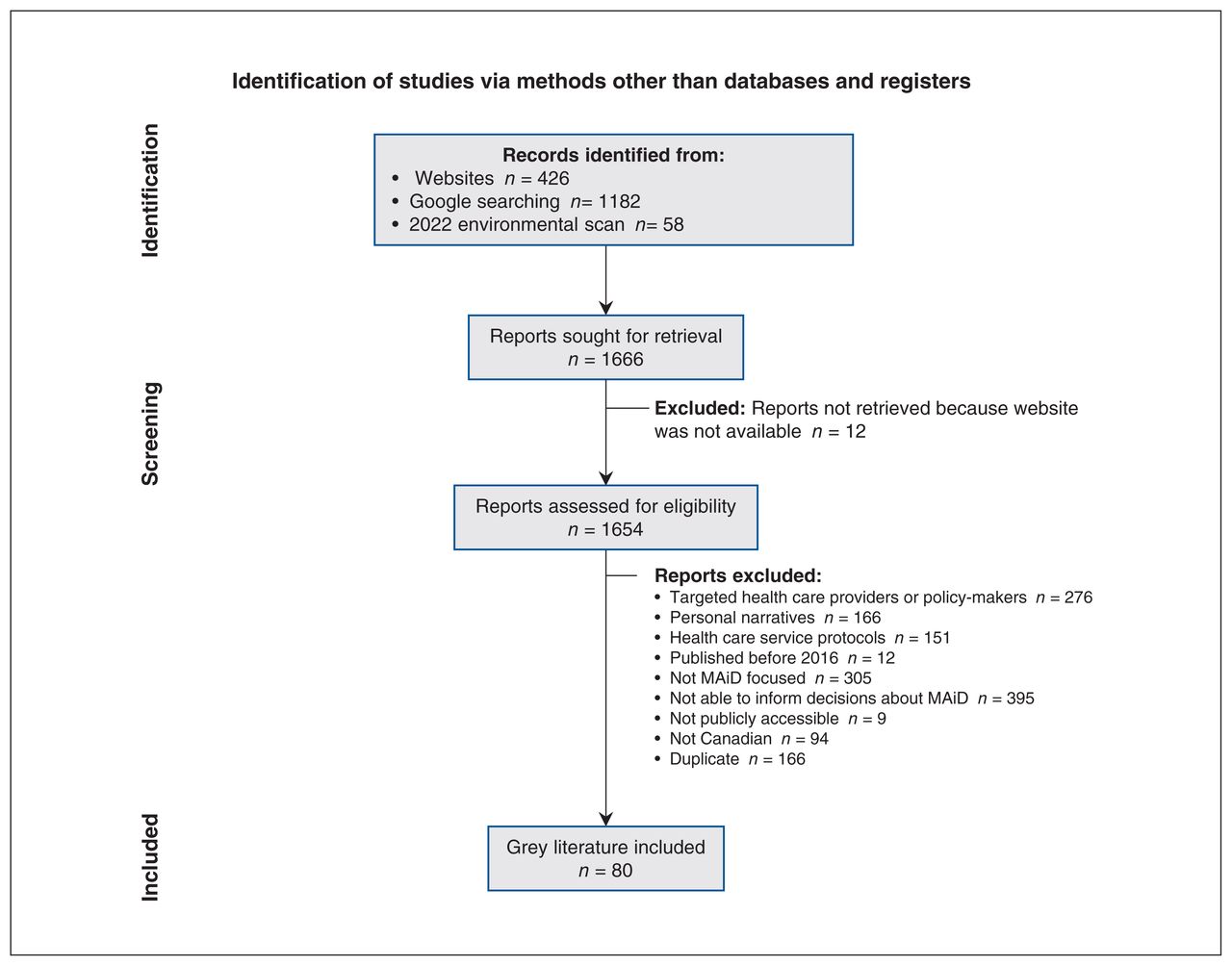
PRISMA diagram of search results. Note: MAiD = medical assistance in dying, PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Main characteristics of publicly available MAiD resources*
Quality appraisal of resources
By March 2023, 24 months after Bill C-7 was approved, 62 of 69 (90%) resources were updated with eligibility criteria to reflect this 2021 legislation, and 11 resources did not discuss any eligibility criteria. Our earlier searches indicated that fewer resources were updated in August 2021 (38 of 49; 78%) or April 2022 (40 of 49; 82%).
None of the 80 eligible resources met the criteria to be defined as patient decision aids (Table 2). The median IPDAS score was 3 out of 7 (IQR 2–4, range 0–5) (Figure 4). In the 80 resources, the IPDAS criteria that were most often met were as follows: describes the health condition (n = 67; 84%), information on the target audience (n = 59; 74%) and states the decision to be made (n = 43; 54%). Forty-two (52%) resources provided options and none provided information on the potential benefits or potential harms of the options.
Appraisal results using International Patient Decision Aids Standards defining criteria and Patient Education Materials Assessment Tool scores

Percentage of medical assistance in dying resources for patients that met criteria to qualify as a patient decision aid* (n = 80). *Appraised by International Patient Decision Aids Standards criteria and a criterion proposed by Martin and colleagues.15
The median PEMAT understandability score was 75% (IQR 67%–84%, range 50%–100%) (Table 2; Figure 5). Of 80 resources, 47 (59%) achieved an adequate understandability rating of 70% or greater. The applicable PEMAT understandability items met by most resources were as follows: numbers appearing in the material are clear and easy to understand (39 of 40; 98%), the material breaks information into short sections (74 of 77; 96%) and the material uses visual cues to draw attention to key points (74 of 77; 96%). PEMAT understandability items met by few resources were as follows: provides a summary (2 of 73; 3%, visual aids have clear titles or captions (2 of 26; 8%) and the visual aids reinforce rather than distract from the content (4 of 26; 15%).
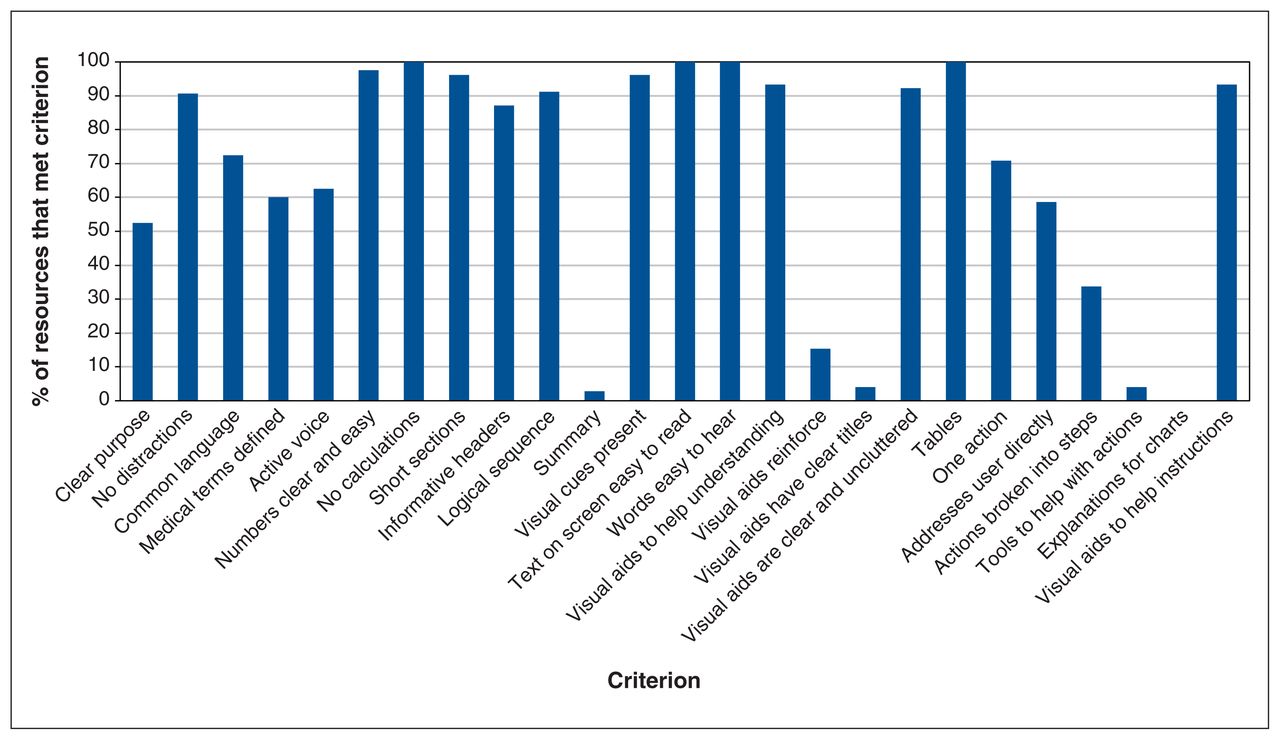
Percentage of medical assistance in dying resources for patients that met criteria for understandability and actionability* (n = 80). *Appraised by the Patient Education Materials Assessment Tool.
The median PEMAT actionability score was 60% (IQR 20%–80%, range 0–100). Of 80 resources, 23 (29%) achieved an adequate actionability rating of 70% or greater. Applicable PEMAT actionability items that were mostly met were as follows: uses visual aids whenever it could to make it easier to act on actions (70 of 75; 93%), clearly identifies at least 1 action the user can take (56 of 79; 71%) and addresses the user directly when describing actions (47 of 80; 59%). PEMAT actionability items that were rarely met were as follows: explains how to use the charts, graphs, tables or diagrams to take actions (none); provides a tangible tool whenever it could help the user take actions (3 of 76; 4%); and breaks down the action into manageable, explicit steps (27 of 80; 34%).
Interpretation
Of 80 publicly available resources on MAiD in Canada, most reported on 2021 updated eligibility criteria according to Bill C-7. According to the PEMAT appraisal tool, approximately half of the resources were understandable and few were actionable. Despite the fact that MAiD is a preference-sensitive decision having at least 1 alternative option, no resources were patient decision aids. These findings lead to the following discussion points.
With the finality and legal aspects of MAiD, it is essential that MAiD resources for patients are continually updated as legislation changes.12,19 Most MAiD resources were updated 24 months after Bill C-7 legislation was released, but fewer were updated at 5 and 13 months after this new legislation.1 It is reassuring that MAiD resources were updated given the increased complexity with this revised legislation and challenges with ensuring educational resources are up to date as new evidence emerges.20 If publicly available MAiD resources are outdated, newly eligible individuals may be deterred from seeking more information about MAiD or may seek access to MAiD on the basis of unrealistic expectations.
Our findings demonstrate the need to improve both the understandability and actionability of patient education resources on MAiD to make them more accessible for people in Canada of lower health literacy. Understandability of resources may be improved by providing a summary of key points, presenting resources in an active voice, and using visual images or diagrams.16,21,22 Actionability of decision-support resources may be improved by breaking down actions into manageable steps and providing a tangible tool to help the user take action.16,23 Tools, such as checklists, improve understanding and recall when provided in patient resources.21 Patient decision aids are often structured in a series of steps to guide the process of deliberating and communicating with others.24 A recent review of 73 education resources for adults with osteoarthritis revealed that resources structured as patient decision aids scored higher for actionability than other resources.25
No Canadian resources met the IPDAS criteria to be defined as a patient decision aid, an effective intervention to support preference-sensitive decisions.18 Our findings were consistent with the Ottawa Hospital Research Institute’s A to Z Inventory of Patient Decision Aids, which has no decision aids on MAiD-related topics.26 However, it is possible that authors of MAiD decision aids have not registered them in the A to Z inventory. This inventory includes several decisions aids focused on advanced care planning for end-of-life and other life and death decisions, such as starting or stopping dialysis. Previous studies have reported that patients who used patient decision aids for end-of-life decisions about their goals of care often experienced less decisional conflict and were more comfortable discussing the decision.27–29 A key element of patient decision aids is providing information on all reasonable options.14 However, only half of the identified Canadian MAiD resources listed alternative options, despite there being other treatments that could be considered for relieving or easing unbearable suffering, including palliative care, counselling services, mental health care, disability support services and community services.30 Our findings cause us to reflect on the unusual nature of patient decision aids for people considering MAiD when one of the possible options involves death. User-testing of a draft patient decision aid to guide pastoral workers discussing end-of-life care options revealed that some pastoral workers were reluctant to use it, as they were morally and religiously against MAiD (Dr. Louisa Blair, Anglican Church of Canada, Toronto, Ont.: personal communication, 2022).
Little is known about whether a patient decision aid can address patients’ or their families’ decision-making needs. This knowledge gap requires further research. Ideally, patient decision aids should be developed with a user-centred design or be co-produced with patients and families to ensure the final product is relevant to those for whom it is targeted and subsequently used in clinical practice.31,32 Developers should also follow health literacy guidance, including adhering to PEMAT thresholds for understandability and actionability, aiming for grade 5 to 8 reading level, using plain language and providing alternative formats that do not require reading.33 Finally, evaluation of the patient decision aid should initially focus on acceptability and, if acceptable, evaluate the effect on decision quality (e.g., informed and values-based choice) and the decision-making process (e.g., decisional conflict, decision regret and confidence in the decision).5,34
Limitations
Our environmental scan has strengths and limitations to consider when interpreting the findings. The search strategy was comprehensive for Canadian federal, provincial and territorial governments, as well as relevant Canadian organizations’ websites. However, given the changing nature of websites, it is possible that previously published resources may no longer be available or be moved to different web pages, making them harder to locate. Another strength was that the search, data extraction and appraisal of resources was conducted independently by 2 of 3 authors. It is possible that we missed some non-English or non-French resources given that the search was done with terms in English and French, and once a resource was identified we looked for its availability in other languages. Finally, we did not specifically search websites of all health care organizations in Canada (e.g., hospitals, long-term care centres and hospices).
Conclusion
Our environmental scan identified and quality appraised 80 Canadian resources about MAiD for patients. Most resources accurately reflected the 2021 legislation on eligibility criteria but none were patient decision aids. Only about half met the adequate PEMAT health literacy scores for understandability and few for actionability. Therefore, current MAiD resources are limited for guiding decision-making or for supporting people in Canada. Our research findings suggest that developers from national and provincial governments, and health care organizations need to improve the quality of MAiD resources to better support people in Canada with lower health literacy or who speak languages other than English or French, and consider ways of structuring the information to help them make this preference-sensitive decision. Future research should investigate whether patient decision aids are an effective resource for the preference-sensitive nature of MAiD decisions.
Acknowledgement
The authors acknowledge Anwar Parbtani for his support while writing this study.
Footnotes
Competing interests: Krystina Lewis reports grant funding (payments made to institution) from the Canadian Institutes for Health Research (CIHR), Canadian Cardiovascular Society, Cardiovascular Network of Canada (CANet), and Heart and Stroke Foundation of Canada. Lissa Pacheco-Brousseau reports CIHR grant funding. Dawn Stacey holds a University of Ottawa Research Chair in Knowledge Translation to Patients, grants from CIHR, and Canadian Cancer Society honoraria for a Canadian Lung Cancer conference and support to attend meetings from German Neurological Society and the University of Southern Denmark. She is an unpaid member of the Shared Decision Making Advisory Board, Denmark. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Alda Kiss was the first author. Alda Kiss and Dawn Stacey made substantial contributions to the design of the work, completed the environmental scan, completed the collection and appraisal of resources, completed the interpretation of the data and drafted the manuscript. Krystina Lewis, France Légaré and Laura Wilding made substantial contributions to the manuscript by interpretation of data and reviewing it critically for important intellectual content. Lissa Pacheco-Brousseau and Qian Zhang made substantial contributions to the manuscript by appraising the resources (data acquisition) and reviewing it critically for important intellectual content. Lindsey Sikora made substantial contributions to the manuscript by verifying the search strategy (data acquisition) and reviewing it critically for important intellectual content. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding: Dawn Stacey holds a University of Ottawa Research Chair in Knowledge Translation to Patients, and France Légaré holds a Canada Research Chair in Shared Decision Making and Knowledge Translation. No funding was received to support this study.
Data sharing: Data are available on request to the corresponding author.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/5/E869/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools





