


Article Figures & Tables
Figures
- Figure 1:
PRISMA flow diagram.
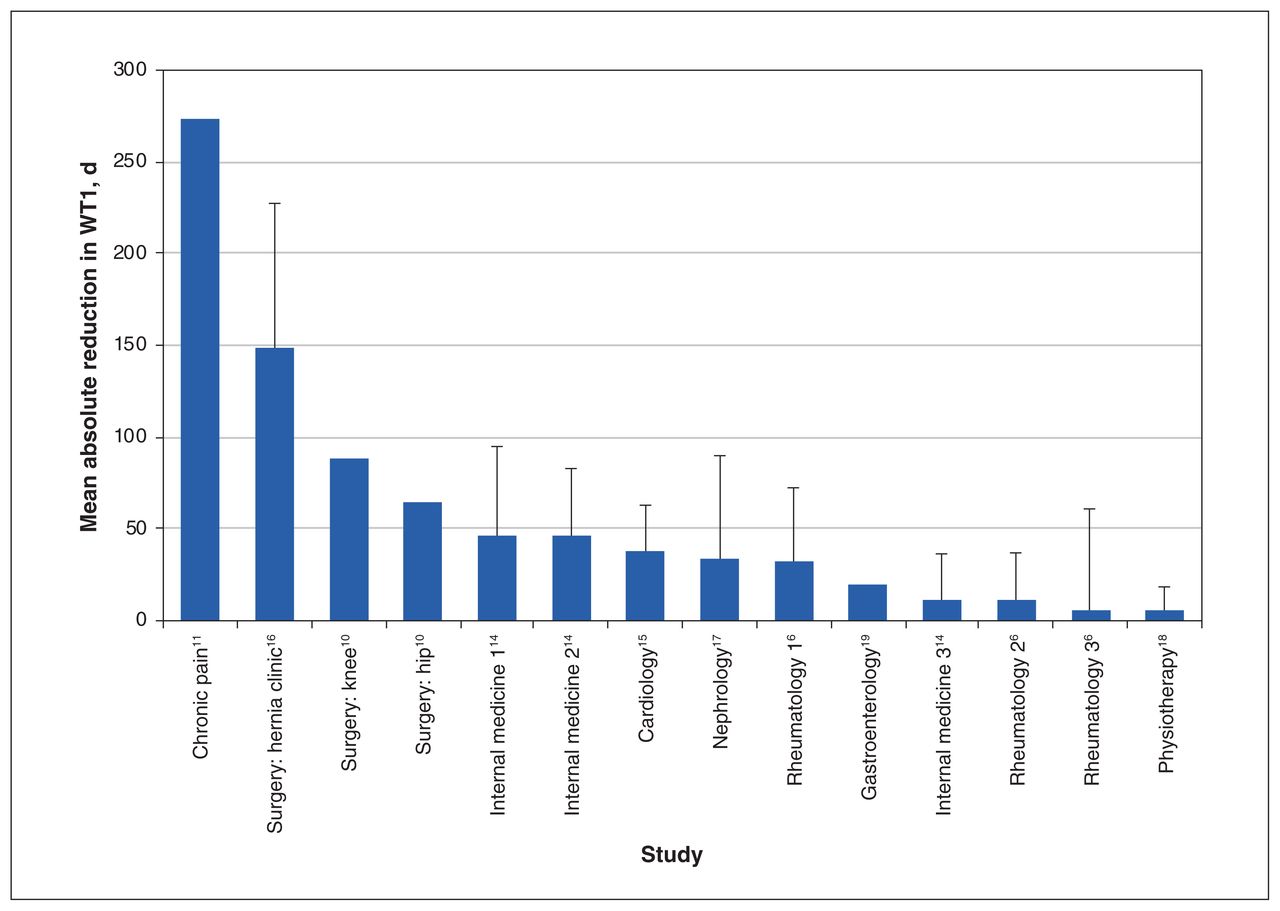
- Figure 2:
Absolute reduction in wait time 1 (WT1) across the included studies. For purposes of this figure, the total number of studies was 9; the study by Leach and colleagues (12) was omitted because the published report lacked continuous data. Error bars represent the standard deviation, where it was reported in the included studies. Note: For internal medicine, 1 = routine, 2 = moderate, 3 = urgent; for rheumatology, 1 = moderate, 2 = urgent, 3 = routine.
- Figure 3:
Mean absolute reduction in wait time 1 (WT1) across specialties. For purposes of this figure, the total number of studies was 9; the study by Leach and colleagues (12) was omitted because the published report lacked continuous data. The estimates of absolute reduction stratified by specialty were derived from multiple studies. For internal medicine (IM), the first data point represents a mean of all levels of referral from multiple studies, whereas other IM data points represent specific values for different levels of referral, as reported in the cited studies. Note: “other” = chronic pain and physiotherapy.
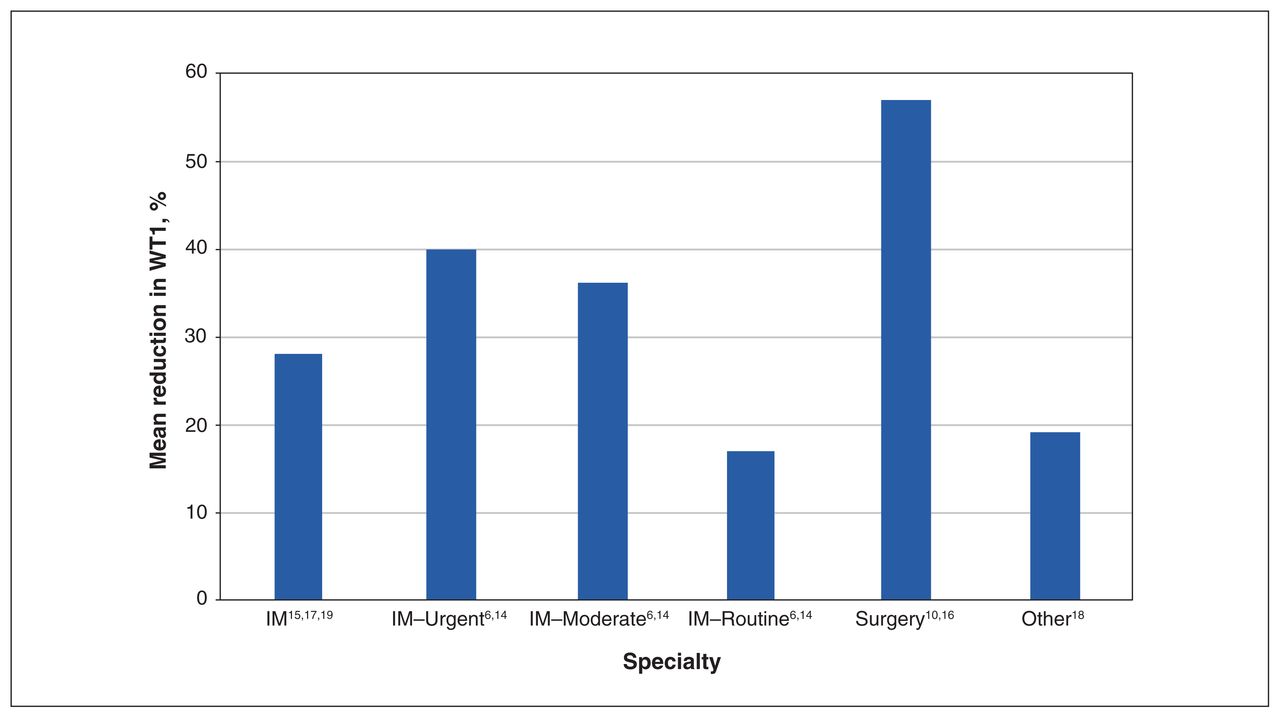
- Figure 4:
Mean percent reduction in wait time 1 (WT1) across specialties. For purposes of this figure, the total number of studies was 8; the studies by Clark (11) and Leach and colleagues (12) were omitted because percent reduction in WT1 could not be calculated from the published data. For internal medicine (IM), the first data point represents a mean of all levels of referral from multiple studies, whereas other IM data points represent specific values for different levels of referral, as reported in the cited studies. Note: “other” = physiotherapy.
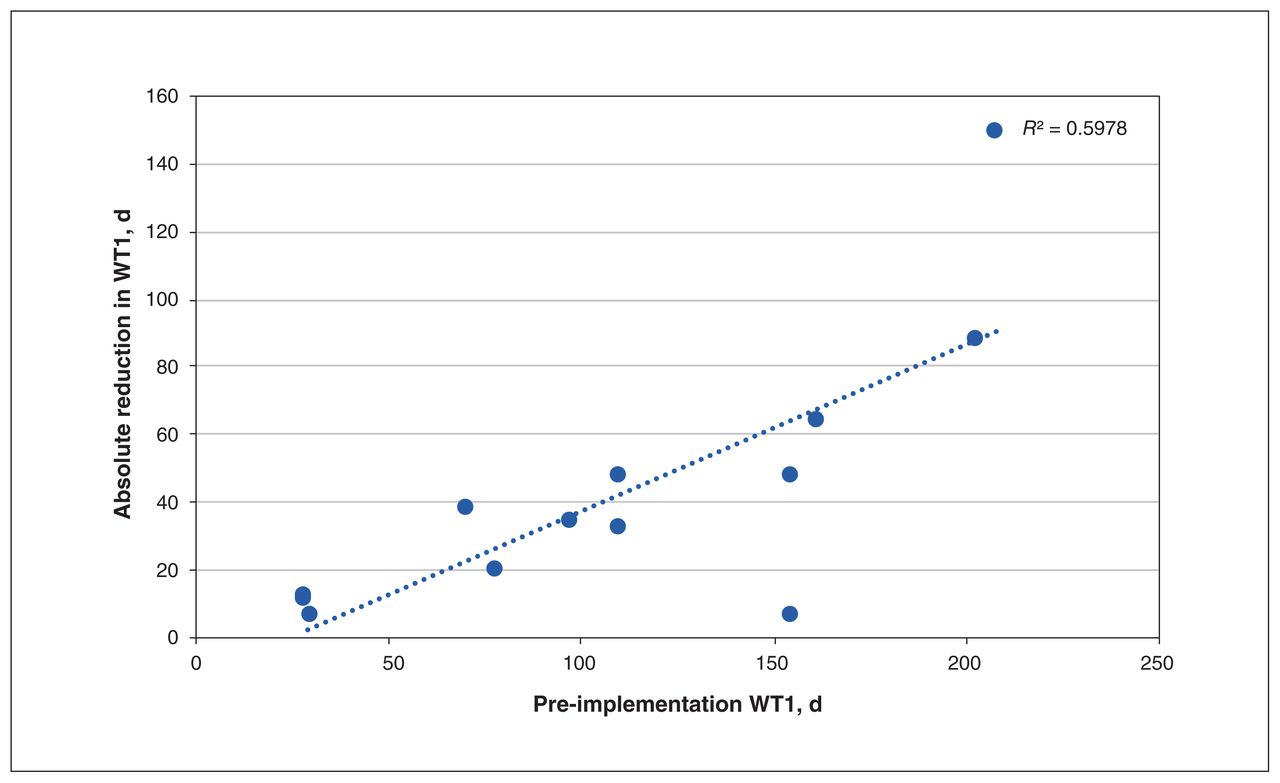
- Figure 5:
Relation between absolute reduction in wait time 1 (WT1) and pre-implementation WT1. For purposes of this figure, the total number of studies was 8; the studies by Clark (11) and Leach and colleagues (12) were omitted because continuous data were not available.



Tables
Reference (year) and country Study design Sample size Health system and specialty setting Characteristics of SEM Implementation process and fidelity Leach et al. (2004), (12) England Simple pre–post with non-equivalent group, time series NA Single payer, surgery: spinal Pooled list, optional A managed generic waiting list was implemented for initial outpatient appointment and subsequent surgery, and a computerized MRI booking system was integrated with outpatient follow-up appointments. As part of the managed generic waiting list, a consultant screened all new outpatient GP spinal referrals to assess suitability for a pooled waiting list, and patients were referred to next available physician. Same process was applied for managed generic waiting list for surgery.
Implementation fidelity: NABichel et al. (2009), (14) Canada Simple pre–post with no equivalent groups, time series 8289 patients Single payer, internal medicine Central access and triage, mandatory The conference model preceded and allowed for development and implementation of the central access and triage system. The latter involved pooling referrals by specialty, using standardized information requirements and policy for confirmation of receipt of referral, as well as for acceptance of appointment. Wait times were measured in weeks to appointment, based on triage priority.
Implementation fidelity: NABungard et al. (2009), (15) Canada Simple pre–post with non-equivalent groups, time series 3096 patients Single payer, cardiology Single point of entry, optional Cardiac EASE (January 2004–December 2006) was the single-point-of-entry model. Referrals were tracked through the MedTech database. All referrals were sent via fax to a single EASE intake service location and reviewed by EASE NP. Patients and referring FP were offered the choice of enrolling in EASE. Cardiologist involvement was voluntary, and most chose to participate. There was no advertising of the program. There was prompt feedback to the referring physician.
Implementation fidelity: NAMacleod et al. (2009), (10) Canada Simple pre–post with non-equivalent groups, time series NA Single payer, surgery: hip and knee Central intake, optional The HKRP was a centralized intake model in which referrals were registered and triaged by an advanced practice physiotherapist. Six hospitals within the TC LHIN implemented the HKRP. There was a single wait list, with technology to support referral management.
Implementation fidelity: TC LHIN was accountable for the HKRP. The organization monitored wait lists under the Wait Times Strategy and worked collaboratively with hospitals to improve TC LHIN wait list management processes.Van den Heuvel et al. (2012), (16) Canada Cross-sectional 94 patients Single payer, surgery: hernia clinic Common waiting list, optional Patients were put on a common waiting list to await next available physician. Clinic was run by 4 surgeons, as well as fellows, residents and students. All administrative data were input into a single database. Triage was performed by surgeon.
Implementation fidelity: Letter was sent to FPs informing them of the new initiative. Patients received letter with date and time of appointment, along with information about the hernia clinic, health questionnaire and QoL questionnaire.Schachter et al. (2013), (17) Canada Prospective, pre–post with non-equivalent groups, time series 920 patients Single payer, nephrology Central triage, optional A physician-led provincial change strategy was implemented. Wait time issue was brought up in a preliminary survey at a BC nephrology conference in 2009. In addition, through a modified Delphi process, in-person meetings and surveys, wait time targets were established. Time targets took into account comorbidities, eGFR, BP and albuminuria. A priority score from 1 to 4 was assigned for referred conditions. Finally, the benchmark targets were approved by BC nephrologists at the BCPRA Medical Advisory Committee meeting and were then disseminated to all nephrologists in BC. A hard-copy reference sheet was provided for use during triage of new patients.
Implementation fidelity: NAClark (2015), (11) Canada Simple pre–post with non-equivalent groups, time series NA Single payer, chronic pain Central intake, optional All referrals were triaged by a nurse and administrative staff. Wait lists at 3 different sites were centralized, duplicates were identified, and a single wait list was formed.
Implementation fidelity: NAHazlewood et al. (2016), (6) Canada Simple pre–post with nonequivalent groups, time series 8414 referrals Single payer, rheumatology Central intake, optional CReATe Rheum was a centralized referral system. Referrals were sent via a single fax number. A standardized referral form was given to the RP, but the form was not enforced if all required information was given in the referral letter. A nurse with > 15 yr experience and 2 clerical support persons processed referrals to physicians. Any concerns with referrals were directed to 2 senior rheumatologists. A multiuser database was developed to track referrals, and missing information was obtained by sending a standardized form to the RP. Evaluation was conducted to determine impact over the short term (2 yr) and the long term (until 2013). Implementation fidelity: The 2 senior rheumatologists were involved in providing training to other rheumatologists to ensure easy transition to new system. Wittmeier et al. (2016), (18) Canada Simple pre–post with nonequivalent groups, time series 1399 patients Single payer, physiotherapy Central intake, mandatory A central intake system was implemented by the Child Health Physiotherapy team at the Health Sciences Centre in Winnipeg for children with complex needs.
Implementation fidelity: NAGoodsall et al. (2017), (19) Australia Simple pre–post with nonequivalent groups, time series 1118 referrals Two-tier, gastroenterology Single point of entry, mandatory A pooled waiting list and centralized intake and triage with a “week on” roster for staff specialists was implemented. Intake and triage were categorized as “urgent” or “routine.” Patients were seen by the next available provider, and a rapid access clinic was established for urgent cases.
Implementation fidelity: NANote: BCPRA = BC Provincial Renal Agency, BP = blood pressure, CReATe Rheum = Central Referral and Triage in Rheumatology, EASE = Ensuring Access and Speedy Evaluation, eGFR = estimated glomerular filtration rate, FP = family physician, GP = general practitioner, HKRP = Hip and Knee Replacement Program, MRI = magnetic resonance imaging, NA = not available, NP = nurse practitioner, QoL = quality of life, RP = referring physician, SEM = single-entry model, TC LHIN = Toronto Central Local Health Integration Network.
- Table 2:
Assessment of risk of bias, based on the Risk of Bias in Nonrandomized Studies of Interventions tool (13)
Article Type of bias Conflict of interest Funding* Confounding Selection of participants Classification of interventions Deviations from interventions Missing data Measurement of outcomes Selection of results Overall Leach et al. (2004) (12) Serious Moderate Low Low Low Moderate Low Serious Unclear Unclear Bichel et al. (2009) (14) Serious Low Low Moderate Moderate Low Low Serious Unclear Low Bungard et al. (2009) (15) Serious Low Low Moderate Low Low Low Serious Unclear Low Macleod et al. (2009) (10) Serious Critical Low Low Moderate Low Low Critical Unclear Unclear Van den Heuvel et al. (2012) (16) Critical Low Low Moderate Moderate Moderate Moderate Critical High Unclear Schachter et al. (2013) (17) Serious Moderate Low Moderate Moderate Low Low Serious Unclear Low Clark (2015) (11)† Serious Low Low Moderate Moderate Low Low Serious Unclear Unclear Hazlewood et al. (2016) (6) Serious Low Low Moderate Serious Low Low Serious Unclear Low Wittmeier et al. (2016) (18) Serious Low Low Moderate Moderate Low Moderate Serious Low Low Goodsall et al. (2017) (19) Serious Moderate Low Moderate Moderate Low Low Serious Unclear Unclear Reference WT1, mean ± SD* Reduction, mean ± SD* Patient volume WT1 for control group Before SEM After SEM Absolute Relative, % Before SEM After SEM Leach et al. (2004) (12) No. of patients waiting > 26 wk: 85
No. of patients waiting 13–26 wk: 90No. of patients waiting > 26 wk: 0
No. of patients waiting 13–26 wk: 15No. of patients waiting > 26 wk: 85
No. of patients waiting 13–26 wk: 75% of patients waiting > 26 wk: 100
% of patients waiting 13–26 wk: 83.3NA NA NA Bichel et al. (2009) (14) Urgent: 29 ± 46 d
Moderate-level: 110 ± 57 d
Routine: 155 ± 88 dUrgent: 17 ± 14 d (p < 0.05)
Moderate-level: 63 ± 42 d (p < 0.00005)
Routine: 108 ± 37 d (statistical test not performed)Urgent: 12 ± 48 d
Moderate-level: 47 ± 71 d
Routine: 47 ± 95 dUrgent: mean 41.4
Moderate-level: mean 42.7
Routine: mean 30.3Increases in referral volume: 75% for endocrinology, 50% for gastroenterology, 26% for general internal medicine; no change in referral volume for rheumatology and hematology NA NA Bungard et al. (2009) (15) 71 ± 45 d 33 ± 19 d (p < 0.001) 38 ± 49 d 53.5 Increase by about 50% from 2004 to 2005 and by 19% from 2005 to 2006 NA NA Macleod et al. (2009) (10) Knee: 203 d
Hip: 162 dKnee: 115 d
Hip: 98 dKnee: 88 d
Hip: 64 dKnee: 43.3
Hip: 39.5NA NA NA Van den Heuvel et al. (2012) (16) 208 ± 139 d 59 ± 70 d 149 ± 156 d 71.6 NA NA NA Schacter et al. (2013) (17) 98 ± 84 d 64 ± 73 d 34 ± 111 d 34.7 NA NA NA Clark (2015) (11) About 24 to > 48 mo 9-mo overall reduction 274 d NA NA NA NA Hazlewood et al. (2016) (6) Routine: 155 ± 88 d
Moderate-level: 110 ± 57 d
Urgent: 29 ± 46 dRoutine: 149 ± 65 d (p = 0.11)
Moderate-level: 78 ± 56 d (p < 0.001)
Urgent: 18 ± 23 d (p = 0.01)Routine: 6 ± 109 d
Moderate-level: 32 ± 80 d
Urgent: 11 ± 51 dRoutine: 3.87
Moderate-level: 29.1
Urgent: 37.9NA NA NA Wittmeier et al. (2016) (18) Children with complex needs (neurodevelopmental conditions): 29.8 ± 17.9 d Children with complex needs: 24.3 ± 17.0 d (p < 0.0001) 5.5 ± 25 d 18.5 Complex needs: same referral volume Comparison groups: increased referral volume Comparison group (orthopedic conditions): 20.4 ± 14.3 d Comparison group: 22.1 ± 13.1 d (p < 0.0001) Goodsall et al. (2017) (19) 78 d 58 d (p < 0.01) 20 d 25.6 NA NA NA Note: NA = not available, SD = standard deviation, SEM = single-entry model, WT = wait time, WT1 = wait time 1.
↵* Except where indicated otherwise.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools



Related Articles
Cited By...
- Streamlining lung cancer management in Nova Scotia amid COVID-19: pooled triaging for expedited curative-intent oncologic surgery
- Ce nest pas au service des urgences que devrait etre annonce un diagnostic de cancer
- The emergency department is no place to be told you have cancer
- Perceptions of Ontario health system leaders on single-entry models for managing the COVID-19 elective surgery backlog: an interpretive descriptive study