


Abstract
Background: Postoperative pain management practices in breast surgery are variable, with recent evidence that approaches for minimizing or sparing opioids can be successfully implemented. We describe opioid filling and predictors of higher doses in patients undergoing same-day breast surgery in Ontario, Canada.
Methods: In this retrospective population-based cohort study, we used linked administrative health data to identify patients aged 18 years or older who underwent same-day breast surgery from 2012 to 2020. We categorized procedure types by increasing invasiveness of surgery: partial, with or without axillary intervention (P ± axilla); total, with or without axillary intervention (T ± axilla); radical, with or without axillary intervention (R ± axilla); and bilateral. The primary outcome was filling an opioid prescription within 7 or fewer days after surgery. Secondary outcomes were total oral morphine equivalents (OMEs) filled (mg, median and interquartile range [IQR]) and filling more than 1 prescription within 7 or fewer days after surgery. We estimated associations (adjusted risk ratios [RRs] and 95% confidence intervals [CIs]) between study variables and outcomes in multivariable models. We used a random intercept for each unique prescriber to account for provider-level clustering.
Results: Of the 84 369 patients who underwent same-day breast surgery, 72% (n = 60 620) filled an opioid prescription. Median OMEs filled increased with invasiveness (P ± axilla = 135 [IQR 90–180] mg; T ± axilla = 135 [IQR 100–200] mg; R ± axilla = 150 [IQR 113–225] mg, bilateral surgery = 150 [IQR 113–225] mg; p < 0.0001). Factors associated with filling more than 1 opioid prescription were age 30–59 years (v. age 18–29 yr), increased invasiveness (RR 1.98, 95% CI 1.70–2.30 bilateral v. P ± axilla), Charlson Comorbidity Index ≥ 2 versus 0–1 (RR 1.50, 95% CI 1.34–1.69) and malignancy (RR 1.39, 95% CI 1.26–1.53).
Interpretation: Most patients undergoing same-day breast surgery fill an opioid prescription within 7 days. Efforts are needed to identify patient groups where opioids may be successfully minimized or eliminated.
The rising use and misuse of opioids is a national and international crisis that contributes significantly to opioid-related deaths, particularly in young adults.1,2 In Canada, between January 2016 and June 2019, there were more than 13 900 apparent opioid-related deaths and 17 000 opioid-related hospital admissions.3 In Canada and the United States, physicians prescribe higher quantities of opioids than in other countries4,5 and the amount prescribed is often greater than is needed, as evidenced by the large numbers of unused opioids.6,7 This may lead to long-term use in opioid-naive patients,8,9 misuse by others in the household10,11 and diversion (i.e., transfer of a medication from a lawful to unlawful distribution or use).12 Surgeons commonly prescribe opioid analgesics to treat acute postoperative pain. In the US, despite writing only 1.8% of all medication prescriptions, surgeons accounted for 9.8% of all opioid prescriptions.13
Breast cancer is the most common cancer in women in Canada, occurring in 1 in 8 females, with 27 000 new cases in 2019.14 Breast surgery is commonly used to treat benign and malignant conditions. Postoperative pain management practices in breast surgery are variable among surgeons in the US,15,16 with high rates of opioid analgesic overprescription,5 despite recent literature that suggests 5 days is the appropriate length of time that opioids should be prescribed for breast surgery, if prescribed at all.17 A recent Canadian study showed that patients undergoing breast surgery can achieve adequate pain control with minimal to no postoperative opioids.18 To better evaluate prescribing practices, the Ontario Ministry of Health and Long-Term Care mandated data collection on opioid prescribing in 2012.19 Given the high volumes of breast surgery in Canada, the lack of detailed population-based data on prescribing and recent evidence from single-institution studies suggesting that lower opioid analgesic doses can be safely prescribed, we evaluated postoperative opioid filling in patients undergoing same-day breast surgery in Ontario, Canada.
Methods
Study cohort and setting
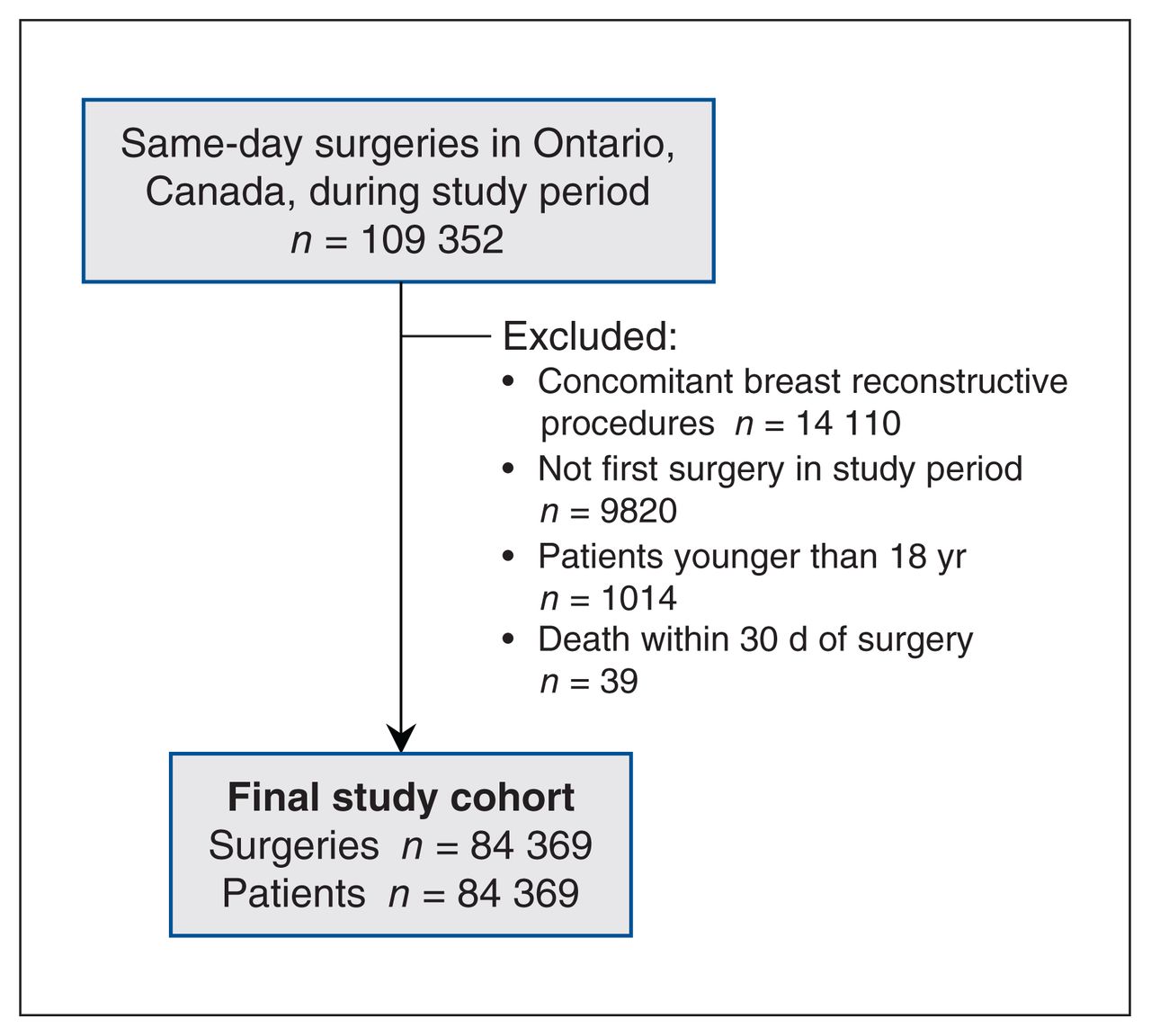
We conducted a retrospective population-based cohort study in which we identified patients aged at least 18 years in Ontario, Canada, who underwent same-day breast surgery, with or without axillary intervention, from July 1, 2012, to June 30, 2020. Ontario has a population of about 14 million people, which represents nearly 38.8% of the Canadian population. 20 Ontario has a universal health insurance plan that covers basic health care services (e.g., costs associated with physician visits, inpatient hospital admissions). We excluded patients if they had concomitant breast reconstructive surgery (anticipated higher pain levels), died within 30 days of surgery or were younger than 18 years. We captured the first breast surgery per patient during the study period, and the number of unique surgeries is therefore the same as the number of patients (Figure 1).
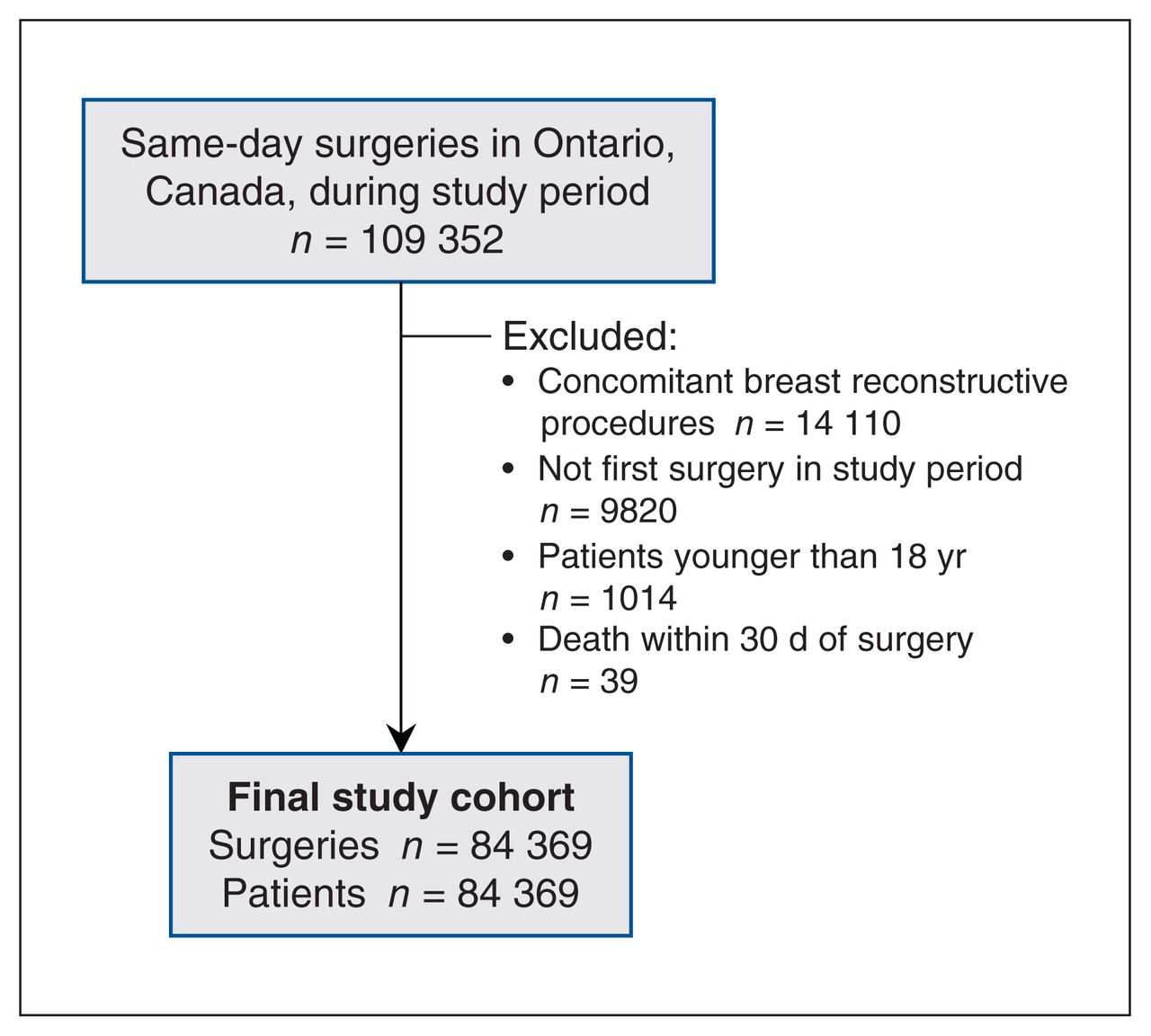
Cohort creation flowchart for patients undergoing same-day breast surgery in Ontario, Canada, during the study period (July 1, 2012, to June 30, 2020). Final cohort of n = 84 369 represents number of unique first surgeries and number of patients.
Administrative databases
We used the linked administrative databases housed at ICES (https://www.ices.on.ca). We captured same-day surgeries using the Canadian Institute for Health Information (CIHI) Same Day Surgery database, which includes mandatory submissions from hospitals to the Ministry of Health. Between 2012 and 2020, Same Day Surgery records with valid linking numbers ranged from a low of 98.67% to a high of 98.77%. This database may include a small proportion of patients who were admitted after surgery. We selected codes for partial (P) (i.e., lumpectomy, excisional biopsy), total (T) (i.e., mastectomy), radical breast excision (R) (i.e., mastectomy with removal of axillary lymph nodes) and simultaneous axillary intervention (axilla) from the Canadian Classification of Health Interventions (Appendix 1, Appendix Table 1, available at www.cmajopen.ca/content/11/2/E208/suppl/DC1).21 We used International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) diagnostic codes to identify malignancy, with the remainder classified as benign (Appendix 2, Appendix Table 2, available at www.cmajopen.ca/content/11/2/E208/suppl/DC1). We identified opioid prescriptions from the Narcotics Monitoring System (NMS) database. Established in July 2012 through the Ontario Narcotics Strategy, the NMS records information on controlled drug prescriptions issued to Ontario residents, regardless of payment method. The NMS database collects information from prescription dispensers, and therefore includes only information recorded by the pharmacy where a prescription was filled. We categorized the opioids, including combinations, as codeine, tramadol, oxycodone, morphine, hydromorphone, methadone and other (Appendix 3, Appendix Table 3, available at www.cmajopen.ca/content/11/2/E208/suppl/DC1). Demographic characteristics including age and sex were captured in the Registered Persons Database (RPDB). We used the CIHI Discharge Abstract Database, which includes mandatory submissions from hospitals to the Ministry of Health, to capture patient comorbidities. These data sets were cleaned and linked using unique encoded identifiers and analyzed at ICES. Data were reported in accordance with recommendations from the Reporting of Studies Conducted Using Observational Routinely-Collected Data (RECORD) statement.22
Characteristics of patients undergoing same-day breast surgery in Ontario, Canada, during the study period, categorized by filling of opioid prescriptions within 7 days of surgery date (n = 84 369)*
Median oral morphine equivalents (mg) filled within 7 days of same-day surgery in the cohort by procedure, institution and year of surgery during the study period*
Unadjusted and adjusted analyses of factors associated with filling of opioid prescription within 7 days of same-day breast surgery (n = 84 369)
Variables
We characterized patients by sex (male, female), age (18–29 yr, 30–39 yr, 40–49 yr, 50–59 yr, 60–69 yr, 70–79 yr, ≥ 80 yr) and Charlson Comorbidity Index ([CCI] 0–1, ≥ 2) in the 5 years before the index breast surgery. The CCI categorizes ICD diagnosis codes into predefined comorbid conditions and assigns a weight based on disease burden and its relative importance to patient prognosis.23 We used postal codes linked to the postal code conversion file to assign area-level income quintiles, where quintile 1 represents the lowest incomes. We defined residence as either rural (community size < 10 000) or urban, using the postal code conversion file. We defined institutions as those providing instruction to medical trainees (teaching hospitals), those that do not (small [< 100 beds] and community [≥ 100 beds] hospitals) and pediatric hospitals, which typically provide care to patients younger than 18 years. We categorized diagnoses as benign or malignant, and procedure types by increasing invasiveness of surgery: partial, with or without axillary intervention (P ± axilla); total, with or without axillary intervention (T ± axilla); radical, with or without axillary intervention (R ± axilla); and bilateral. We also categorized the year of breast surgery.
Outcomes
The primary outcome was filling an opioid prescription within 7 days of surgery (days 0–7), where day 0 was day of surgery. We selected the 7-day time frame based on clinical judgment and previous studies in this domain.18,24,25 Secondary outcomes were total oral morphine equivalents (OMEs) filled (mg, median and interquartile range [IQR]; i.e., Q1 to Q3) and more than 1 prescription filled within 7 days of surgery.
Statistical and sensitivity analysis
We compared patient characteristics, procedure type, year of surgery and institution classification by opioid prescription filled using the standardized difference, where a difference of 0.10 or more indicates a meaningful difference between groups.26 We noted missing data for “location of residence” (0.2% of the cohort) and “hospital type” (3.6% of the cohort). We did not exclude patients based on missing data27 and included them in all analyses. Associations (adjusted risk ratios [RRs] and 95% confidence intervals [CIs]) between the above covariates chosen a priori based on substantive relevance to opioid prescribing and filling (age, breast cancer diagnosis, CCI status, hospital type, location of residence, sex, socioeconomic status, type of procedure, year of surgery) and outcomes (filling of any opioid prescription, filling of > 1 opioid prescription) were estimated in multivariable models using modified Poisson regression.28 Because the opioid analgesic dose may better indicate extent of opioid exposure and potential for subsequent harm, we performed sensitivity analyses to estimate associations between our covariates and higher OMEs filled, predetermined as 75th percentile or higher (Appendix 4, Appendix Table 4, available at www.cmajopen.ca/content/11/2/E208/suppl/DC1). The analyses (i.e., filling of > 1 prescription, filling ≥ 75th percentile of OMEs) were restricted to those patients who filled an opioid prescription and those for whom OMEs could be calculated (n = 73 excluded, owing to injectable route of opioid delivery). Because of the potential for provider-level clustering with high- (or low-) dose prescribing, we used a random intercept for each unique prescriber in NMS. If any patient filled more than 1 prescription from different providers, we randomly assigned 1 of the providers to the patient. We examined differences in median OME dose by procedure, institution and year of surgery, using Kruskal–Wallis tests.
Unadjusted and adjusted analyses of factors associated with filling more than 1 opioid prescription within 7 days of same-day breast surgery
We also performed a sensitivity analysis excluding patients with known opioid use disorder in the previous 5 years (ICD-10 codes: F11.1X, F11.2X, F11.9X) and those prescribed buprenorphine and methadone during the study period (n = 124). The results of these analyses were similar to the primary analysis and therefore we report only the results of the primary analysis. We used SAS version 9.4.5 (SAS Institute).
Ethics approval
This study was approved by the Health Sciences and Affiliated Teaching Hospitals Research Ethics Board at Queen’s University.
Results
A total of 109 352 same-day breast surgeries were performed in Ontario from July 1, 2012, through June 30, 2020. After we applied exclusions, 84 369 patients comprised the study cohort (Figure 1). Most patients (72%, n = 60 620) filled an opioid prescription, with a minority (4%) of these patients filling additional prescriptions within 7 days of surgery (1 additional = 3.2%, 2 additional = 0.3%, ≥ 3 additional = 0.2%).
Most of the patients in the cohort were female (98%), with a median age of 58 (IQR 48–68) years. Most had a CCI of 0–1 (91%, indicating low comorbidity) and resided in an urban setting (89%). Surgery was most often performed in a community hospital (69%), and less often in teaching (27%), small (0.7%) and pediatric (0.2%) hospitals. More than half (56%) of patients had malignancy. Types of procedures were P ± axilla (87%), T ± axilla (6%), R ± axilla (3%) and bilateral surgery (4%). The number of patients undergoing surgery per study year was similar, except for 2012 and 2020, in which data for only 6 months were captured (Table 1).
Table 2 shows OMEs filled by procedure type, hospital type and year of surgery for 60 547 patients. The OMEs filled increased with invasiveness of surgery (P ± axilla = 135 [IQR 90–180] mg; T ± axilla = 135 [IQR 100–200] mg; R ± axilla = 150 [IQR 113–225] mg, bilateral surgery = 150 [IQR 113–225] mg, p < 0.0001). The OMEs did not differ between teaching and community hospitals (135 [IQR 90–180] mg, p = 0.83), even when examined by procedure type (data not shown). For all procedures, OMEs decreased over the study period, from 135 (IQR 113–225) mg in 2012 to 75 (IQR 50–113) mg in 2020 (p < 0.0001).
Figure 2 shows the most common opioid prescriptions filled. Codeine was the most common (39%), followed by oxycodone (23%), tramadol (22%), hydromorphone (12%), morphine (2%), methadone (0.7%) and others (0.5%).

Categorization of opioids filled by patients within 7 days of same-day breast surgery during the study period. For a listing of agents included in the “Other” category, see Appendix 3, Appendix Table 3 (available at www.cmajopen.ca/content/11/2/E208/suppl/DC1).
Figure 3 shows filling of opioid prescriptions by postoperative day, with most prescriptions being filled on the day of surgery (postoperative day 0).
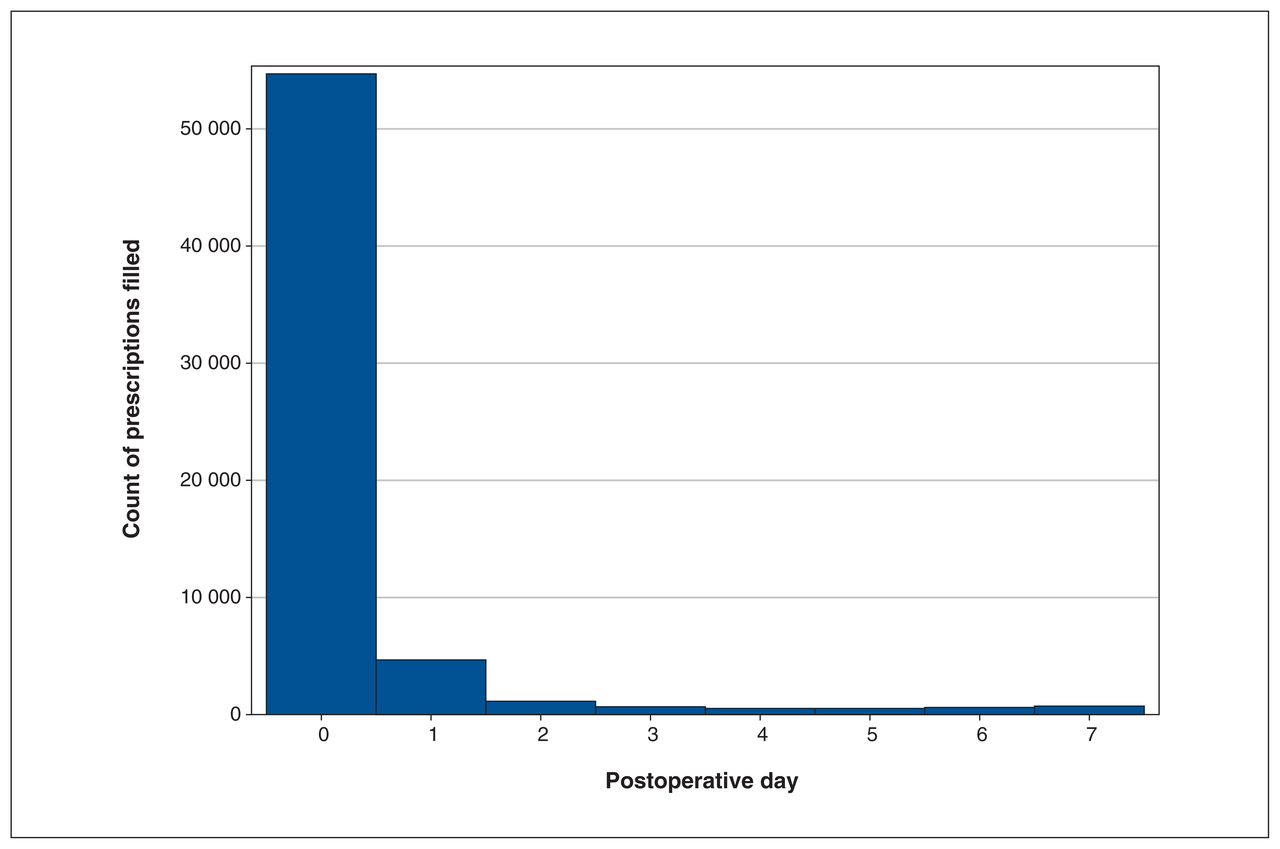
Filling of opioid prescriptions by postoperative day. Most prescriptions were filled on the day of surgery (postoperative day 0).
Table 3 shows factors associated with prescriptions filled within 7 days of breast surgery among all patients in the cohort. In adjusted models, factors associated with filling an opioid prescription were malignancy (RR 1.16, 95% CI 1.15–1.17) and increased invasiveness of surgery (RR 1.12, 95% CI 1.10–1.14 for bilateral surgery, R ± axilla and T ± axilla v. P ± axilla). Factors associated with a decreased likelihood of filling an opioid prescription were age 80 years or older (RR 0.80, 95% CI 0.78–0.83), 70–79 years (RR 0.89, 95% CI 0.87–0.91), 60–69 years (RR 0.93, 95% CI 0.91–0.95) and 50–59 years (RR 0.97, 95% CI 0.95–0.99), all versus age 18–29 years, CCI of 2 or greater (RR 0.90, 95% CI 0.89–0.92 v. CCI 0–1), all non-community hospitals (i.e., teaching hospital [RR 0.90, 95% CI 0.89–0.91] v. community hospital), and surgery in 2020 (RR 0.97, 95% CI 0.94–0.99 v. 2012).
Table 4 shows factors associated with filling more than 1 opioid prescription within 7 days of surgery among the 60 620 patients who filled at least 1 prescription. In the adjusted models accounting for provider-level clustering, factors significantly associated with filling more than 1 prescription were age 30–59 years (v. age 18–29 yr), malignancy (RR 1.39, 95% CI 1.26–1.53), CCI of 2 or greater (RR 1.50, 95% CI 1.34–1.69 v. CCI 0–1) and increased invasiveness of surgery (RR 1.98, 95% CI 1.70–2.30 bilateral surgery v. P ± axilla). Teaching hospital (RR 0.78, 95% CI 0.68–0.90) was associated with a decreased likelihood of filling more than 1 prescription.
In the sensitivity analysis accounting for provider-level clustering, factors associated with higher (≥ 75th percentile) prescription filling were similar to those observed for filling more than 1 prescription, with the exception of a small increased likelihood in males (RR 1.09, 95% CI 1.01–1.18), decreased likelihood in age 80 years or older (RR 0.85, 95% CI 0.76–0.95, compared with age 18–29 yr) and more recent years of surgery (RR 0.23, 95% CI 0.18–0.30 in 2020 compared with 2012) (Appendix 4, Appendix Table 4). There was some overlap between patients who filled more than 1 prescription and those in the 75th or higher percentile of filled opioids, as among 2240 patients who filled more than 1 prescription, 1907 (85%) of patients filled the 75th or higher percentile of opioids.
Interpretation
We describe opioid filling in patients undergoing same-day breast surgery without reconstructive procedures in Ontario. Most patients (72%) filled a prescription for opioid medication, with variability in the agent and amount prescribed. Although there is a trend in decreased OMEs filled in more recent study years, certain patient and clinical factors were associated with higher OMEs filled.
Despite recent small studies showing that opioids can be successfully eliminated in breast surgery, most patients in Ontario who underwent same-day breast surgery between July 2012 and June 2020 filled an opioid prescription. Moo and colleagues29 showed that routine opioid analgesic prescriptions were not necessary after excisional biopsy or lumpectomy if patients were encouraged to use nonsteroidal anti-inflammatory agents. Rojas and colleagues30 reported similar pain scores in patients who underwent lumpectomy and who received opioid analgesics compared with those who did not. Although these studies were limited to patients undergoing lumpectomy, most (87%) of the patients in our cohort also underwent partial excision, suggesting that if an opioid-sparing approach was developed for these patients, then opioid prescribing would be significantly reduced.
Although elimination of opioids in this population may be a desirable goal, there are factors that may suggest a need for opioid medications. As anticipated, the amount of OMEs filled correlated with increased invasiveness of surgery, with patients who underwent total or radical resection or bilateral surgery being most likely to fill an opioid prescription and require more than 1 opioid prescription. Similarly, Murphy and colleagues31 reported that patients undergoing breast resection and concomitant reconstructive procedures were most likely to seek additional opioid prescriptions. Park and colleagues16 also reported that higher OMEs were prescribed and used with increased invasiveness of surgery and was highest in patients undergoing concomitant reconstructive procedures. We also report that younger patients, males, those with malignancy, greater comorbidities, and undergoing more invasive surgery were more likely to require additional opioid medication or higher OMEs within 7 days of surgery. Kulkarni and colleagues32 similarly found that younger age and bilateral procedures, as well as severity of preoperative pain, anxiety and depression, were associated with more severe postoperative pain after breast reconstruction. Younger women may desire or require more extensive breast surgery, which may increase the need for opioid medications.33,34 It is possible that the need for higher OMEs in males is related to differences in pain perception between the sexes, although this is controversial.35 Patients with malignancy require more extensive surgery (i.e., margins, axillary surgery for staging or disease removal), which may contribute to increased pain. Lastly, psychological distress associated with a cancer diagnosis may affect pain perception and contribute to individual variation in pain experience.36
The observation of lower OMEs and fewer patients filling more than 1 prescription in teaching compared with community hospitals is interesting, and has also been observed by others.37 Teaching hospitals may be more likely to have enhanced awareness and protocols pertaining to opioids, leading to decreased likelihood of overprescribing. Community hospitals may also suffer from a lack of local resources to enhance awareness pertaining to opioids. Those with greater comorbidities may have higher opioid requirements for reasons other than breast surgery. For example, Cronin and colleagues38 reported that comorbid mood disorders such as depression and anxiety resulted in increased opioid use postoperatively in patients undergoing rotator cuff repair. These studies suggest that while opioids can potentially be eliminated in less invasive breast surgery such as lumpectomy, other factors — such as age, sex, malignancy, presence of comorbidities and extent of surgery — may require health care providers to be aware of higher pain needs. Preoperative awareness is essential so that expectations can be managed, education can be provided and the patient can be offered an individualized approach to pain management.39
While flexibility in prescribing is important to accommodate individual needs, we show significant variability in the type and amount of agent filled in Ontario. We demonstrate large differences in minimum and maximum values in the amounts filled for each type of procedure. Large variations in prescribing have also been observed in patients in Ontario who underwent otologic surgery.40 The variation in agent filled is also noteworthy, as some patients in our cohort received powerful narcotics such as oxycodone, hydromorphone and morphine, known to contribute to opioid-related deaths in Ontario.41 An approach that reduces narcotic prescribing can be successfully introduced and implemented. For example, Hartford and colleagues18 found that a multipronged initiative that reduced opioid analgesic prescribing in patients undergoing outpatient breast surgery did not affect the average pain reported.
In more recent years of the study, we observed a decreased likelihood of filling higher quantities (i.e., ≥ 75th percentile) of opioid medications. This has also been observed in patients undergoing pediatric,42 dental43 and general surgical procedures44 and may be a result of increasing provider awareness pertaining to the opioid crisis,45 national efforts to address the crisis46,47 and awareness of interventions to reduce prescribing. 48,49 Surgeons are interested in interventions that reduce prescribing,50 and studies suggest that such interventions can be successfully implemented. Hill and colleagues48 provided information for surgeons and residents about the number of pills that patients need for postoperative pain control after 5 general surgical operations. They subsequently observed that the number of opioids initially prescribed by the same group of surgeons and residents decreased by more than half. In a systematic review, Zhang and colleagues49 identified behavioural interventions that resulted in a statistically significant decrease in the amount of opioid analgesic prescribed after surgery without negatively affecting pain control. This behooves individuals, institutions and professional organizations to carefully examine opioid-prescribing practices within specific populations with a plan to implement strategies to effect change.
Limitations
Although our study provides new and detailed data on opioid prescribing after same-day breast surgery in Ontario, there are limitations. We were able to capture only opioid filling, which is a proxy for opioid prescribing. It is possible that the rates of opioid prescribing are even higher than we report (i.e., if a provider writes a prescription, but it is never filled by the patient). Furthermore, studies have shown that many patients consume less than the amount prescribed7 and therefore, our reported estimates may overestimate what is being consumed. Some of the OME maximum values are staggeringly high and may reflect a longer supply of medication (i.e., 30-day supply) or those who have underlying opioid use disorder. Although we did not exclude those who may have an opioid use disorder, our sensitivity analysis excluding these patients did not significantly affect the study results. Patient-reported outcomes such as pain scores and satisfaction with pain management are critical in understanding the pain experience. These data are unavailable in the health administrative database, and filling could therefore not be correlated with these important outcomes. The pain experience may also be affected by patient race and ethnicity.32 These data are currently limited in health administrative databases at ICES. There was likely some miscoding of procedure types, as radical resection implies simultaneous removal of axillary lymph nodes; however, a very small percentage of our patients underwent axillary intervention coded separately from radical resection and this likely does not affect our findings.
Conclusion
Our study provides robust data highlighting the variation in opioid filling after same-day breast surgery in Ontario, Canada. Most patients undergoing same-day breast surgery fill an opioid prescription to manage postoperative pain, contrary to recent literature suggesting that opioids can be significantly reduced, if not eliminated. Although the amount of opioid filled postoperatively has decreased in recent years, there remains significant variability in filling. Further efforts are required to better understand in whom opioids can be appropriately reduced or eliminated and whether the observed variation in agent and OMEs filled is harmful to patients.
Acknowledgement
The authors thank IQVIA Solutions Canada Inc. for use of its Drug Information File.
Footnotes
Competing interests: Shaila J. Merchant reports holding an unpaid position as treasurer for the Canadian Society of Surgical Oncology, a nonprofit organization. No other competing interests were declared.
This article has been peer reviewed.
Contributors: All of the authors contributed to the conception and design of the work, and the acquisition, analysis and interpretation of data. All of the authors drafted the manuscript, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This work was funded by a grant to Dr. Shaila Merchant from the Clinical Teachers’ Association of Queen’s University, Endowment Fund.
Data sharing: The data set from this study is held securely in coded form at ICES. Although legal data-sharing agreements between ICES and data providers (e.g., health care organizations and government) prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at https://www.ices.on.ca/DAS (email: das{at}ices.on.ca). The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). Parts of this material are based on data and information compiled and provided by MOH, the Canadian Institute of Health Information (CIHI). The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/2/E208/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.