


Abstract
Background: Early in the COVID-19 pandemic, efforts to decrease risk of viral transmission triggered an abrupt shift from ambulatory health care delivery toward telemedicine. In this study, we explore the perceptions and experiences of telemedicine among socially vulnerable households and suggest strategies to increase equity in telemedicine access.
Methods: Conducted between August 2020 and February 2021, this exploratory qualitative study involved in-depth interviews with members of socially vulnerable households needing health care. Participants were recruited from a food bank and primary care practice in Montréal. Digitally recorded telephone interviews focused on experiences and perceptions related to telemedicine access and use. In our thematic analysis, we employed the framework method to facilitate comparison, and the identification of patterns and themes.
Results: Twenty-nine participants were interviewed, 48% of whom presented as women. Almost all sought health care in the early stages of the pandemic, 69% of which was received via telemedicine. Four themes emerged from the analysis: delays in seeking health care owing to competing priorities and perceptions that COVID-19–related health care took precedence; challenges with appointment booking and logistics given complex online systems, administrative inefficiencies, long wait times and missed calls; issues around quality and continuity of care; and conditional acceptance of telemedicine for certain health problems, and in exceptional circumstances.
Interpretation: Early in the pandemic, participants report telemedicine delivery did not accommodate the diverse needs and capacities of socially vulnerable populations. Patient education, logistical support and care delivery by a trusted provider are suggested solutions, in addition to policies supporting digital equity and quality standards to promote telemedicine access and appropriate use.
The COVID-19 pandemic provoked a rapid shift in ambulatory health care delivery toward telemedicine to enable health care access and reduce the risk of viral transmission.1–3 The transition was abrupt, with accompanying challenges owing to limited telemedicine-related technology and training for physicians and other health care workers.3,4 In Quebec, within the month of July 2020, an unprecedented 1.5 million telemedicine consultations occurred in family medicine, the large majority among physicians with no prior experience with this modality of care.5 The ubiquitous uptake of telemedicine was accompanied by both enthusiasm and caution — enthusiasm about its postpandemic utility in triaging and managing patients with nonurgent conditions, and facilitating access especially among remote populations,6 and caution regarding clinical, organizational, professional, economic, legal and regulatory complexities, including the potential of medical errors, duplication of visits and issues with patient confidentiality. 7–10 In Quebec, several family doctors serving high-needs, multicultural and low-income patient populations observed their absence among those receiving telemedicine during the initial waves of the pandemic. Of concomitant concern was evidence indicating growing racialized inequities in COVID-19–related health care and health outcomes.11,12 Technological, socioeconomic and cultural factors limiting access to primary care, including telemedicine, are possible explanations that require research and policy attention.10
Although a substantial body of literature has explored physicians’ perceptions and needs surrounding telemedicine13–17 and challenges of providing virtual care during the pandemic, 4,18–21 comparatively little attention has focused on the perspectives of patients, much less socially vulnerable patients. In this study, we explore the perceptions and experiences of telemedicine among these individuals and their families early in the pandemic, with the aim of increasing the accessibility and appropriate use of telemedicine going forward.
Methods
This exploratory qualitative study consisted of in-depth interviews with individuals from socially vulnerable households needing health care that elicited their perceptions of and experiences with telemedicine. The patient-centred accessibility framework by Levesque and colleagues22 provided initial guidance on key patient and organizational dimensions of likely relevance in enabling or constraining appropriate access to telemedicine services. Research team members included 2 researchers (A.M.A. and J.H.), 3 graduate students (K.K.A.W., J.C.L. and L.G.T.) and 3 family doctors (M.A., I.L. and K.M.) working with 3 McGill University–affiliated family medicine teaching sites located within the Herzl Family Practice Centre, St. Mary’s Family Medicine Centre and CLSC Parc-Extension.
The study was conducted in the Côte-des-Neiges neighbourhood of Montréal, Quebec, during the first 2 waves of the COVID-19 pandemic from August 2020 to February 2021, when social distancing measures were most restrictive, including the closure of public facilities,23,24 and health systems were struggling to accommodate the burdens of COVID-19–related hospitalizations.25,26 Côte-des-Neiges ranks among the most diverse neighbourhoods in Canada and is the most economically disadvantaged in urban Quebec.27 Like in the rest of Quebec, the large majority of nonurgent in-person primary care services in the neighbourhood reverted to telemedicine during this period, with 80% or more of primary care providers reporting frequent use of telemedicine to reduce the risk of SARS-CoV-2 transmission.3
The study was reported using the Consolidated Criteria for Reporting Qualitative Research checklist.28
Participants
Inclusion criteria for the study were adults aged 18 years and older who were able to communicate in English, French or Spanish; registered with the Québec Health Insurance Plan; and living in socially vulnerable households in which a need for health care had been experienced since the onset of the COVID-19 pandemic. Individuals lacking Quebec health insurance (new arrivals or refugees), living in a household without health care needs or not qualifying as socially vulnerable (defined here as using a food bank or being identified as low income by their family physician) were excluded from the study. Eligible participants were identified by means of an in-person screening questionnaire developed by the research team and delivered in English, French or Spanish to individuals visiting a community food bank in late August and early September 2020. Following consent, potential participants were asked a series of screening questions, which included their Quebec health insurance status, language, access to Internet, length of time in Canada, family structure and whether a household member needed health care since the beginning of the pandemic (Appendix 1, available at www.cmajopen.ca/content/11/2/E219/suppl/DC1). Screening questions about age group and gender identity were not asked directly of potential participants, but rather assessed by the screeners. Screening was conducted by members of the team (A.M.A., K.K.A.W., J.H. and a research associate) and the research coordinator during regularly scheduled food basket pickups. After screening, individuals were asked if they would consent to be contacted for a telephone interview regarding their health care decisions during the pandemic. Among eligible participants, we purposively sampled individuals belonging to households needing health care for a chronic or new health problem, irrespective of whether or how care was received (telemedicine or in person). In October 2020, the sample was supplemented by the inclusion of several high-needs patients identified by family physicians and their residents working at Herzl Family Practice Centre, St. Mary’s Family Medicine Centre and CLSC Parc-Extension. Clinicians employed their own judgment in participant selection based on their knowledge of the patient’s chronic conditions and personal circumstances. The average length of time between recruitment and interview was 2 months, largely owing to challenges in accommodating participant family and work responsibilities.
Data source
The interview guideline was collaboratively developed by researchers and clinician partners, with reference to Levesque and colleagues’ patient-centred accessibility framework22 and the clinical experience of our colleagues (Appendix 2, available at www.cmajopen.ca/content/11/2/E219/suppl/DC1). The interview explored the health care needs of household members during social distancing and lockdown measures, and how they were addressed. Additional questions explored their perceptions and experiences with respect to telemedicine and in-person delivery modalities and how access to health care might be improved. The guideline was piloted on several participants whose data were not included in the study. Adaptations included the inclusion of additional probes to assist less verbal participants. Basic demographic data collected through the screening questionnaires were updated at the beginning of the interview.
Data collection
Based on eligibility as identified by the screening questionnaire, participants were contacted by telephone to request a date and time for interview and to obtain informed consent. Subsequent individual in-depth interviews were conducted by telephone. They were led by 3 English-speaking female, graduate-level, qualitatively trained interviewers (K.K.A.W., J.C.L. and L.G.T.), 2 of whom had prior interview experience. Two interviewers were able to conduct interviews in French (K.K.A.W. and L.G.T.) and 1 in Spanish (L.G.T.). In advance of formal data collection, the interviewer with no interview experience (K.K.A.W.) observed and participated in several pilot interviews led by an experienced member of the team. To accommodate the participants’ preferred language, interviews were conducted in English, French and Spanish. Language preferences were indicated in the screening questionnaire and an appropriate interviewer was assigned before the interviews. Each interviewer took detailed notes during the interview, supplemented by an audio-recording if permission was granted. Digital recordings were transcribed using a summary approach whereby the main points of each interview were captured in English at regular 30-second intervals.29
Data analysis
Team-based analysis was conducted using the framework method,30 a form of thematic analysis that uses data displays to sort, sift and systematically examine and visualize emerging patterns and themes across respondents, categories and concepts. To manage potential researcher biases, analysis was conducted by 3 members of our research team, and intercoder reliability checks were performed to ensure consistency of coding across transcripts.
Verbatim quotes (word-for-word in English) were used for passages where the direct voice of respondents was deemed memorable and worth preserving, especially those related to health care experiences. Both recordings and narrative summaries were verified by another member of the team and uploaded into Dedoose, a data management software, to expedite coding and analysis. A priori codes based on the interview guideline and Levesque and colleagues’ patient-centred accessibility framework22 were systematically defined and applied through the development of a shared code book. Twice-monthly meetings occurred between all members of the study team to discuss new codes, themes and patterns, and their implications. In addition, code reports and data displays were generated to identify higher-level themes and to compare participant perceptions and experiences using deductive and inductive analytic approaches.
Results were shared with family doctors, nurses and administrators from participating clinics, as well as community organizations working with vulnerable populations, at a series of 5 deliberative dialogues that identified priority actions to ensure that telemedicine meets the health care needs of the socially vulnerable (Appendix 3, available at www.cmajopen.ca/content/11/2/E219/suppl/DC1).
Ethics approval
Ethics approval was obtained from the research ethics board of the Centre intégré universitaire de santé et de services sociaux de l’Ouest-de-l’Île-de-Montréal — biomedical subcommittee.
Results
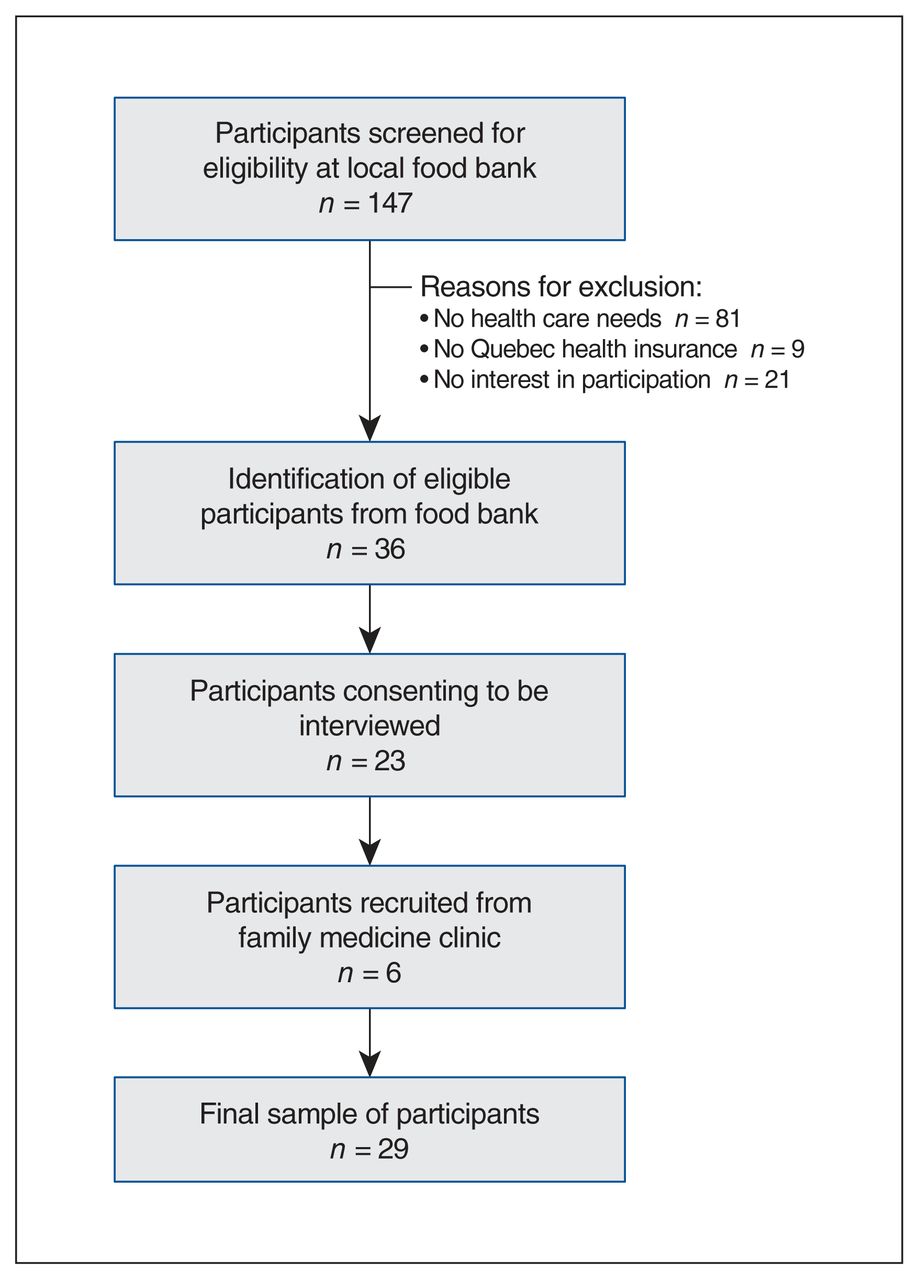
We screened 147 individuals at the local community food bank. A total of 36 eligible households were identified, 23 of which participated in the study. The principal reasons for exclusion included no health care needs reported, no health insurance card and no interest in participation. Six additional households were recruited by clinicians, for a total of 29 interviews. Each interview lasted between 30 and 45 minutes, and all but 2 were recorded (Figure 1).
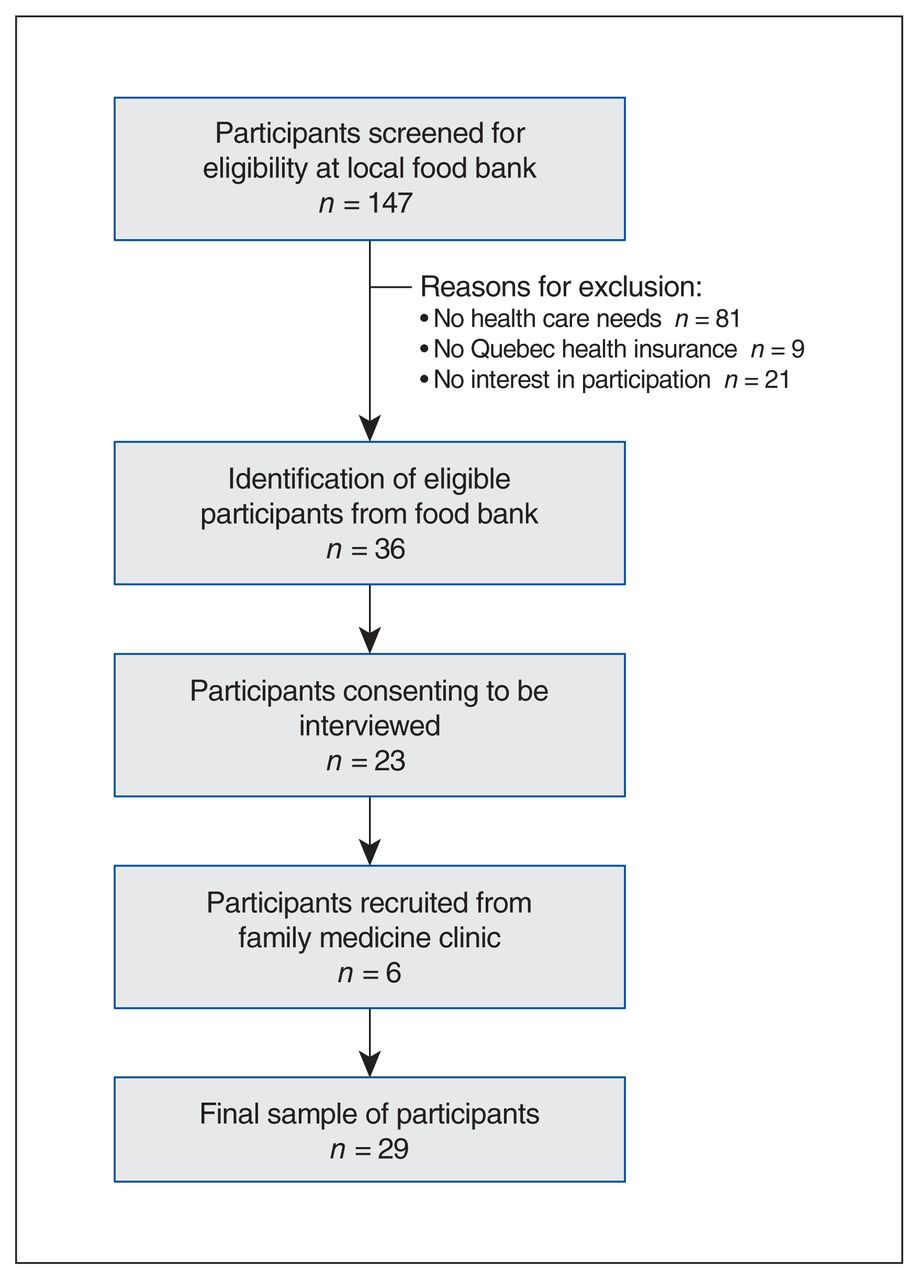
Participant recruitment flow diagram.
Nearly half (48%) of the 29 participants presented as women, 17% were Canadian-born and 72% reported having a family physician (Table 1). More than half (52%) of participants appeared middle-aged, 28% appeared older and 21% appeared younger. Health care needs were indicated by all participants in the period between the start of the pandemic in March 2020 and the time of recruitment (as per inclusion criteria), and 90% had sought health care. Of participants, 69% used telemedicine; 62% had received telemedicine by telephone and 10% by video (Table 1).
Characteristics of members of socially vulnerable households needing health care during early stages of the COVID-19 pandemic
Four overarching themes emerged from the analysis, which describe the health care perceptions and experiences of socially vulnerable households in our sample. Associated quotations are presented in Table 2.
Representative quotations from members of socially vulnerable households needing health care during early stages of the COVID-19 pandemic
Pandemic-related delays in seeking health care
Evidence of delayed care seeking was widespread. Many participants downplayed their own health care needs, with the intention of enabling health care providers to prioritize COVID-19–related illness, or patients with more serious health care needs than their own. Some reported overlooking their health problems when faced with competing concerns such as food insecurity and child care due to job loss and school closures, while others delayed seeking care for fear of contracting SARS-CoV-2. Delays in care seeking owing to difficulties finding out how to organize care during the pandemic, and hesitancy about use of telemedicine, were mentioned less, but were often conveyed in a manner that indicated distress.
Challenges with appointment booking and logistics of encounter
Many participants noted that appointment booking is a pervasive barrier to care seeking even in normal times; however, during the pandemic, anxieties were heightened by not knowing what to do in the context of shifting administrative practices and pandemic restrictions. Making an appointment often required multiple attempts before a receptionist was reached. According to 1 participant, the anticipated time and effort to fix an appointment further contributed to delayed or forgone care.
As the pandemic continued, many health care institutions pivoted to online appointment-booking, a particularly stressful and exclusionary prospect for socially vulnerable people lacking access to necessary technology (computer, Internet, smartphone), know-how or support.31,32 In our sample alone, 4 participants indicated they lacked access to the Internet.
Among study participants using telemedicine, many expressed being insufficiently prepared for what to expect in the consultation. Some presented in person, not having understood that it was scheduled as a telemedicine appointment, and were obliged to restart the appointment-booking process. Others missed calls from receptionists, often while at work, resulting in telemedicine consultations not being confirmed. In a few instances, consultations were missed altogether as patients were not forewarned that their physician would call from an unidentified number, which was widely employed to protect provider and patient privacy.
Notable delays in the start time of telemedicine appointments were also reported, leading many to worry that they had missed their consultation but lacking a means to check on its status. In instances of missed or delayed appointments, some participants explained how old problems had resolved or new ones had emerged by the time their appointment took place. A small number of participants indicated unease about the lack of privacy within their household, and discomfort with telemedicine as a result.
Concerns about quality and continuity of care using telemedicine
Communication is a challenge in telemedicine especially among those with limited language proficiency, hearing or cognitive difficulties. Among those who had experienced a telephone consultation, virtually all participants expressed concerns regarding their ability to effectively explain their health problems or to understand the explanations of clinicians without the assistance of visual and nonverbal cues. A few participants described their discomfort when asked to perform self-examination, while others expressed a lack of confidence in their diagnosis, and a sense that they “hadn’t been seen.” In addition to reduced trust in the quality of care, lack of physical examination and focused, face-to-face discussion may lead to ambivalence in following recommendations. Several participants noted that less attention may be given to instructions delivered virtually owing to the patient being distracted and not listening, or, more fundamentally, to doubts about the legitimacy of telemedicine as a modality of medical care.
Complaints regarding lack of continuity of care also surrounded the pivot to telemedicine early in the pandemic. This was especially noted in teaching centres where residents were engaged to help facilitate virtual health care delivery. Participants described their frustration and discomfort when telemedicine encounters were with unfamiliar providers, and not their regular family doctor.
Conditional acceptance of telemedicine
Our low-income and socially vulnerable study participants recognized the advantages of telemedicine in reducing potential exposure to SARS-CoV-2, and saving time and expenses related to travelling to and from health care facilities. They also recognized its utility for certain issues, such as minor health problems, prescription refills and, for some, mental health challenges. However, their acceptance was conditional. For the majority, telemedicine services were considered a pandemic-specific solution, and inappropriate for complex health care needs or consultations that would normally require a physical examination. Even if not ideal, participants considered telemedicine acceptable in circumstances when a previous trusting relationship was established through in-person care, enabling human connection and touch. Conversely, trust in telemedicine was undermined when an established doctor–patient relationship was problematic or lacking. Several described how interpersonal conflicts (such as rudeness or lack of empathy) were exacerbated in the telemedicine encounter, or when dealing with an unknown provider.
Interpretation
Consistent with clinician observations of delayed or forgone care, widespread apprehension regarding early pandemic health care seeking was evident among socially vulnerable households. Many of our participants described how pressing non–health-related demands related to food and job security took precedence over health care seeking. Others explained their decision to delay care seeking as a response to beliefs that COVID-19 was being prioritized and that those with more urgent health care issues should come first.
Although study participants perceived certain advantages of telemedicine, most considered it a pandemic-specific care delivery modality. Supporting the existing literature,4,16,17,19–21 advantages included time efficiencies related to work and travel, protection from risk of infection, and its utility for routine follow-up and minor health conditions. Indeed, for socially vulnerable populations, certain features of telemedicine conferred accessibility advantages over in-person care. Nonetheless, participant experiences with telemedicine point to appointment booking and communication during the consultation as areas needing improvement. Critiques related to appointment booking included systems inefficiencies, lack of clear messaging regarding wait time and inadequate efforts to ensure patient readiness for the telemedicine encounter. For our socially vulnerable participants, language barriers, inflexible work schedules, and limited privacy or computers to access patient portals or take video calls made these challenges even more difficult.
Consistent with our findings, the literature documents a range of concerns related to doctor–patient communication during the telemedicine encounter, such as patient confidentiality, lack of physical examination, and the need for an existing and trusting patient–provider relationship to assure quality and continuity of care.17,21,33–36 Many participants in our study expressed frustration at not being able to effectively articulate their health concerns in the absence of a physical examination or in the privacy of a doctor’s office. Others perceived that the lack of face-to-face contact during telephone consultations impeded the ability of providers to appraise their needs and provide appropriate reassurance and clarification. In this regard, a strong preference was voiced for telemedicine delivered by a known and trusted provider, a finding supported elsewhere in the literature.37 Lending support to the value of continuous care, a retrospective cohort study on virtual patient–provider communication found that 81% of virtual visits required no follow-up when a patient connected with their own primary care provider.38 Communication challenges were further exacerbated among socially vulnerable patients due to limited language proficiency and challenges related to access to and comfort with technology. Together, these findings emphasize that clinicians be especially attentive to establishing a patient connection, exploring the patient’s perspective and clarifying key recommendations within the telemedicine encounter.36,39,40
A substantial body of literature has examined the potential of telemedicine in various areas of specialized health care.41–45 This has been supplemented by more recent research on its deployment during the COVID-19 pandemic, largely from a clinical or provider perspective.4,19,46–48 Comparatively lacking are studies that consider patients’ perspectives and experiences with telemedicine as a modality of primary care service delivery, particularly among socially vulnerable groups.49 This is partly due to Canada’s slow adoption of telemedicine before the pandemic, with most provision occurring in the private sector.50 This study fills this gap by eliciting the perspectives of high-need populations whose diverse social realities may hinder access to care. Study findings emphasize that equitable primary health care services delivered by telemedicine must accommodate the needs and capacities of people with a wide range of ethnocultural, linguistic, generational and socioeconomic characteristics. Strategies may include patient education about the appropriate use of telemedicine services, ascertaining patient capacities to receive a telemedicine call, ensuring that a trusted provider delivers telemedicine care and implementing necessary actions to improve equity.17,51 Equitable access would be further enabled if underserved and diverse communities were meaningfully represented in telemedicine design, implementation management and evaluation. Such efforts would facilitate telemedicine effectiveness, relevance and appropriate use.52 Clear parameters of quality must also be established based on evidence and best practice,52 with a strong emphasis on actions to promote digital equity.53,54 Policy that supports such efforts is critical at both national and provincial levels. This includes guidelines to standardize best telemedicine practices, and training for health care providers and the public regarding its appropriate use.3 Policy priorities must also include measures to ensure the rights, safety and needs of patients, as well as support around technology access and use among vulnerable populations.55 Finally, to effect policy reforms, health systems investments are crucial to address many of the technical, human and organizational challenges identified by our participants, and to maximize the appropriate deployment of telemedicine in the postpandemic period.56
Limitations
In the context of social distancing and containment measures during the COVID-19 pandemic, several adaptations were required in our study that may have biased results. First was our use of telephone interviews, effectively excluding the participation of people without access to a telephone or unlimited calling minutes, and diminishing opportunities for human connection. Conducting interviews by telephone also inhibited the observation of nonverbal cues essential to probing or interpretating our interviewees’ narratives and the contexts in which they were being shared.57 We also did not offer participants the opportunity to review transcripts before analysis.
Other limitations included failure to collect exact data on participant gender or age, and not representing a full range of socially vulnerable participants, including those living in long-term assisted care and those experiencing homelessness.
Conclusion
The pivot to telemedicine during the COVID-19 pandemic provoked a number of challenges for socially vulnerable individuals and their families, including issues with appointment booking owing to technological and work-related constraints, as well as frustration in conveying health care needs and receiving care that is appropriate and trusted. An erosion in equitable access to quality care was the result. Efforts are needed to facilitate informed patient choice, by supporting digital literacy and access to technology, ensuring necessary clarity about the logistics of appointment making and the consultation itself, and providing care that is trusted and understood. Our findings clarify that telemedicine has the potential to exacerbate or alleviate access barriers for certain patients and for certain services depending on how it is implemented and supported. However, if appropriately used, the integration of telemedicine in primary care may enhance the delivery of patient-centric and quality services for socially vulnerable and equity-deserving populations.
Acknowledgements
The study team acknowledges the valuable contributions of Sonia Lussier, study coordinator, and Laura Gallos Tapis, research assistant.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Jeannie Haggerty and Isabelle Leblanc conceived the study. Alayne Adams conceptualized the study design. Khandideh Williams and Jennifer Langill performed the data collection. Alayne Adams, Khandideh Williams and Jennifer Langill conducted the data analysis. Alayne Adams, Jeannie Haggerty and Khandideh Williams drafted the manuscript, and all authors contributed to the interpretation of the data and to the critical revision of the manuscript. All authors approved the final version to be published and agreed to be accountable for all aspects of the work. Alayne Adams assumed the role of guarantor to the work, ensuring that questions related to any part of the work are appropriately investigated and resolved.
Funding: This research was funded by the Research Chair in Family and Community Medicine, St. Mary’s Research Centre.
Data sharing: The data that support the findings of this study are available from the corresponding author (Alayne Adams) on reasonable request.
Supplemental information: For reviewer comments and the original submission of this manuscript, please see www.cmajopen.ca/content/11/2/E219/suppl/DC1.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
- © 2023 CMA Impact Inc. or its licensors
In this issue

{kind=link}
Article tools



Related Articles
Cited By...
- No citing articles found.